Development Of A Novel Scoring System That Determines The Success Of Atrial Fibrillation Ablation As Part Of Cardiac Surgery
Norton A1, Schlosshan D2, Ahmed I3, Tayebjee MH2
1Brighton and Sussex Medical School, Royal Sussex County Hospital, Eastern Road, Brighton.2Department of Cardiology, Leeds General Infirmary.3Royal Sussex County Hospital, Eastern Road, Brighton.
Background: Radiofrequency ablation therapy for the treatment of atrial fibrillation (AF) can be performed as a concomitant procedure alongside cardiac surgery, but carries the risks of increased bypass time and damage to the sinoatrial node. This study aims to assess the efficacy of concomitant surgical AF ablation and develop a novel scoring system to predict post-procedural return to sinus rhythm.
Methods: A review of the Leeds General Infirmary surgical database was conducted to list all patients who had undergone valvular or coronary bypass surgery with concomitant AF ablation between Jan 2012 – Dec 2013 (n = 76). Follow-up was obtained retrospectively using patient notes, clinic letters and echocardiographic data. Primary outcome was freedom from AF at median follow up (383 days). A novel scoring system was created through analysis of previous literature and evaluated using a receiver operating characteristic (ROC) curve.
Results: At median follow up 50.9% of patients undergoing the procedure were free from AF. The novel scoring system was shown to adequately predict post-procedural return to sinus rhythm (ROC AUC = 0.7708).
Conclusion: A novel scoring system was shown to predict procedural success in patients undergoing concomitant AF ablation alongside cardiac surgery. These results can be further validated using larger patient cohorts.
Key Words : AF, Concomitant, Surgical, Ablation, Score.
Correspondence to: Dr MH Tayebjee
Department of Cardiology,
Leeds General Infirmary,
Leeds
LS1 3EX
Atrial Fibrillation (AF) is the most common sustained cardiac arrhythmia in the western world and affects approximately 1-2% of the UK population. The number of patients admitted to NHS hospitals in AF has risen by 60% in the past 20 years, with an approximate healthcare expenditure of 2.2 billion pounds per annum.1
Surgical AF ablation by the creation of a ‘Maze’ of lines within the atria and around the pulmonary veins can be used to treat patients who have AF undergoing cardiac surgery. The rationale of this lesion set is to interrupt arrhythmogenic macro-reentry circuits.2 However, surgical ablation is not appropriate for all patients as it carries a certain degree of risk. This is partially linked to an increase in bypass and crossclamp time.3 There is also a risk of damage to the sinoatrial node; retrospective studies have estimated a 7.2% median risk of pacemaker requirement following the procedure.4 Identifying predictive factors for procedural success can enable clinicians to identify subgroups where medium to longer-term maintenance of sinus rhythm (SR) is an achievable goal and prevent patients from being exposed to unnecessary risk. A number of previous publications have investigated individual preoperative variables that have an effect on predicting procedural success.2 However, few previous studies have proposed a scoring system combining these variables to predict restoration of SR following concomitant AF ablation. This study aimed to create a score system based on the results from previous literature and evaluate its efficacy on a small patient dataset.
i) To assess rates of return to sinus rhythm following concomitant AF ablation alongside cardiac surgery
ii) To evaluate a novel scoring system designed to predict medium to longer term maintenance of sinus rhythm
A review of the Leeds General Infirmary surgical database was conducted to list all patients who had undergone valvular or coronary bypass surgery with concomitant AF ablation between Jan 2012 – Dec 2013 (n = 76).
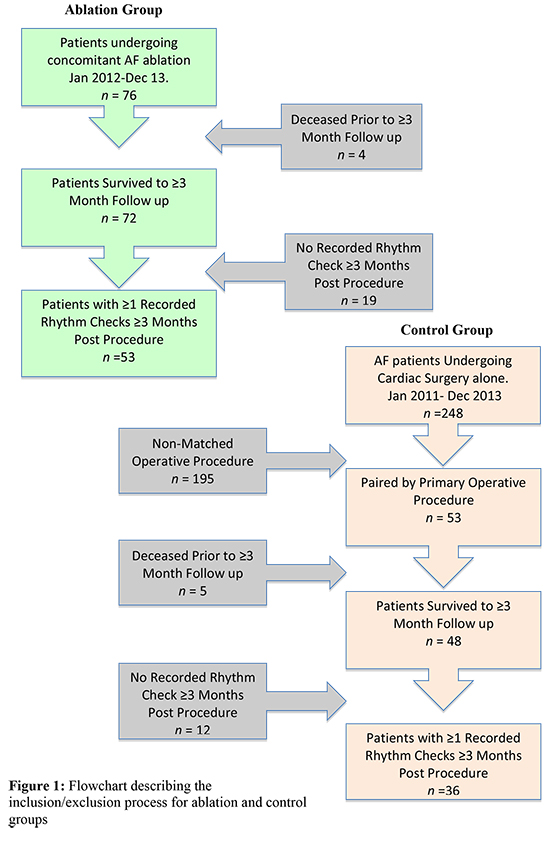
Patients with no prior ablative procedures and a preoperative diagnosis of AF ≥6 months prior to surgery were eligible to be included in the study. Follow up requirements were one or more documented rhythm checks at ≥3 months post procedure. Patients who died prior to 3-month follow up were not included in data analysis (Fig. 1).
Figure 1. a) Surface ECG of a patient in sinus rhythm with activated CCM. The corresponding CCM algorithm is pictured at the bottom of the figure. Abbreviations: RA= right atrial, RV= right ventricular. b) Illustration of the CCM device Optimizer IV with the external charging system. (The illustration was provided from Impulse Dynamics).
All patients were classified according to HRS guidelines in Paroxysmal, Persistent or Longstanding Persistent AF; in further analysis the two latter categories were combined to form a binary result of ‘Paroxysmal’ or ‘Nonparoxysmal’ AF.2
The primary endpoint was freedom from AF at median follow up post surgery (383 days). AF was defined as ≥1 documented episode of atrial fibrillation lasting for ≥30 seconds during the follow up period. A three-month ‘blanking’ period was maintained post surgery when any AF occurrences were not classified as treatment failure.2
Procedures were performed over a two-year period by two separate surgeons. Radiofrequency lesions were created using an Atricure Standard Jaw Isolator Synergy clamp at a frequency of 460kHz and amplitude of 0-30 Watts. An Atricure Isolator Linear pen was used to provide any additional lesions and test for entrance and exit block. The standard lesion set involved a left atrial incision followed by semilunar line of ablation around the right pulmonary ostia. The left pulmonary veins were identically ablated and a line was drawn to connect the 2 encircling lesions, the left atrial appendage and the mitral valve annulus. No right-sided lesions were performed.
A small subset of patients (n=2) underwent cryoablation of the isthmus line using an Atricure cryoICE ablation probe. One surgeon consistently used an Atriclip Gillinov-Cosgrove device (n=10) for closure of the left atrial appendage. The other opted for complete amputation (n=43).
Postoperative care was similar to that of routine heart surgery. All patients received prophylactic anti-arrhythmic therapy and constant rhythm monitoring. Intravenous amiodarone was introduced after weaning from cardiopulmonary bypass at 5 mg/kg up to a maximum of 1.2g in 24 hours. After discharge from intensive care, this was changed to a 200 mg/d oral dosage and adjusted according to heart rate.
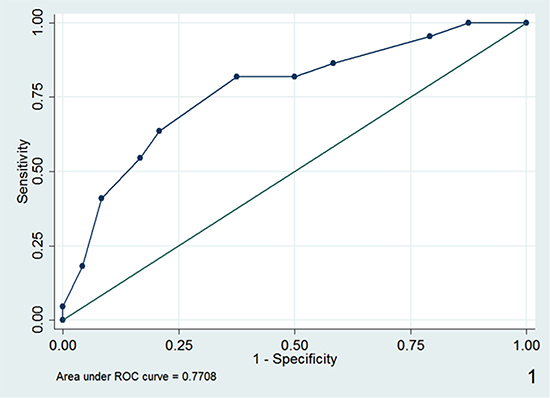
Figure 2. Receiver operating characteristic (ROC) curve for a novel predictive scoring system for concomitant surgical ablation.
Anti arrhythmic medication (mainly amiodarone) was continued for three months after surgery with the aim of stopping at the three month follow up appointment.
Data was obtained from a combination of patient notes, clinic letters and echocardiographic data.
All patients underwent a 12 lead ECG prior to discharge. This was followed by a minimum of one 24 ambulatory ECG (n=38) or 12 lead outpatient ECG (n=18). Median follow up time was 383 days.
Based on previous studies, a number of predictors for maintenance of sinus rhythm were documented (Table 1). Parameters were weighted differentially according to their relative contribution to procedural success. Increasing patient age has been identified as significant predictor of ablation failure in three separate case series.5–7 Patients were categorized into low (age <65 years), medium (age 65-74 years) or high-risk (age > 74 years) categories.
Table 1. Outline of a novel scoring system to predict return to sinus rhythm following concomitant AF ablation
| Score |
Weighting (points) |
| Patient Age (Years) |
65-74→ 1 ≥75 →2 |
| Type of AF |
Non Paroxysmal → 3 |
| Left Atrial Diameter (mm) |
40-44 → 1
45-49 → 2
50-54 → 3
55-59 → 4
60-65 → 5
≥65 → 6 |
| Ejection Fraction |
30-49% → 1
>30% → 2 |
| Mitral Stenosis |
Present → 1 |
The presence of nonparoxysmal AF was given a higher weighting as patients are at a higher risk of treatment failure due to well established and self perpetuating macro-reentry circuits.8–10 A number of studies have demonstrated increasing left atrial size to be a negative predictor for return to sinus rhythm.11,12 Weighting of this variable was defined in accordance to results from Chen et al. who reported that every 1mm increase in left atrial diameter corresponded to a 12.7% increase in risk of postoperative recurrence of AF.13
Two previous studies have shown that surgical ablation for AF is less effective in patients with a decreased left ventricular ejection fraction (LVEF).6,14 Patients were again categorized into low (LVEF ≥50%), medium (LVEF 30-49%) or high (LVEF < 30%) risk. Lastly the presence of mitral stenosis was deemed to be a significant but lower risk variable and therefore was assigned a reduced weighting.14
The score system was evaluated on a subgroup of 46 patients who had undergone surgical ablation. Seven patients were excluded from the initial cohort due to incomplete echocardiographic data.
The novel predictive score was compared against two risk stratification scores commonly used in cardiac surgery for predicting mortality; Euroscore and Parsonnet Score.15,16
Continuous data is presented as mean ± standard deviation and categorical data is presented as frequency and percentage unless otherwise stated. Univariate analysis of continuous data was performed using either Students two-sample t test or Wilcoxon Rank Sum. Normality was tested using the Shapiro Wilk test. Group comparisons for categorical variables were conducted using Chi square or Fisher’s exact test. Statistical significance was set at P<0.05.
Scoring systems shown to be significant on univariate analysis were analysed using a receiver operating characteristic (ROC) curve. This was used to determine cutoff points that yield the highest combined sensitivity and specificity for distinguishing procedural success and failure. Area under the graph was used to represent predictive power of the test.
Statistical analysis was performed using Stata SE version 12.1.
This study is in compliance with the Declaration of Helsinki. All data was collected as part of service evaluation.
Rate Of Return To Sinus Rhythm
A total of 50.9% (n = 27) of patients were recorded to be free from AF at median follow up. Twenty-six patients did not reach the primary endpoint as ≥1 episode(s) of atrial fibrillation lasting for ≥30 seconds were documented during the follow up period.
Success Vs. Failure Characteristics
A greater proportion of patients who failed to reach the primary outcome were in nonparoxysmal AF (80.8% vs. 40.7% respectively, p=0.009). No other predictors of success in reaching the primary end point were statistically significant (Table 2).
Table 2. Preoperative characteristics and perioperative results in patients who have succeeded vs. patients who have failed in meeting the primary outcome.
| Demographic |
Primary Outcome: Success (n=27) |
Primary Outcome:
Failure (n=26) |
P Value |
| Mean Age |
64.2 ± 10.3 |
68.3 ± 9.2 |
0.165 |
| Female |
11 (40.7%) |
10 (38.5%) |
0.865 |
| BMI |
28.7 ± 3.6 |
28.6 ± 3.7 |
0.957 |
| *Left Atrial Diameter (mm) |
49.1 ± 6.7
(n=18) |
52.3 ± 6.5
(n=17) |
0.098 |
| Type of AF |
Paroxysmal: 16 (59.3%)
Persistent: 4 (14.8%)
Longstanding Persistent: 7 (25.9%) |
Paroxysmal: 5 (19.2%)
Persistent: 6 (23.1%)
Longstanding Persistent: 15 (57.7%) |
0.009 |
| NYHA Score |
2.4 ± 0.7 |
2.7 ± 0.6 |
0.094 |
| Ejection Fraction |
>50%: 22 (81.5%)
30-49%: 4 (14.8%)
<30%: 1 (3.7%) |
>50%: 15 (57.7%)
30-49%: 10 (38.5%)
<30%: 1 (3.8%) |
0.112 |
| Valve Disease |
25 (92.6%) |
26 (100%) |
0.236 |
| Haemodynamic Pathology |
Stenosis: 2 (8.0%)
Regurgitation: 14 (56.0%)
Mixed: 9(36.0%) |
Stenosis: 6 (23.1%)
Regurgitation: 18 (69.2%)
Mixed: 2(76.9%) |
0.270 |
| Hypercholesterolemia |
5 (18.5%) |
3 (11.5%) |
0.704 |
| Diabetes |
Insulin Controlled: 4 (14.8%)
Total: 4 (14.8%) |
0 |
0.111 |
| Hypertension |
8 (29.6%) |
10 (38.5%) |
0.497 |
| Procedure |
Mitral Valve: 23 (85.2%)
Aortic Valve: 1 (3.7%)
CABG: 2 (7.4%)
Combination: 1 (3.7%) |
Mitral Valve: 23 (88.5%)
Aortic Valve: 3 (11.5%)
CABG: 0
Combination: 0 |
0.356 |
| Mean Bypass Time (min) |
114.0 ± 41.9 |
116.8 ± 24.2 |
0.124 |
| Mean Cross Clamp Time (min) |
91.0 ± 45.3 |
88.1 ± 16.6 |
0.091 |
| Mean Post Op Stay (days) |
7.8 ± 3.9 |
8.9 ± 4.7 |
0.118 |
| Post Op. Stroke/TIA |
Stroke: 1 (3.7%)
TIA: 0
Total: 1 (3.7%) |
Stroke: 0
TIA: 1 (3.8%)
Total: 1 (3.8%) |
1.00 |
*Mean left atrial diameter was calculated from a smaller cohort (n=46) due to a lack of echocardiographic data. Left ventricular failure (LVF), New York Heart Association (NYHA), Myocardial Infarction (MI), transient ischaemic attack (TIA), estimated glomerular filtration rate (EGFR), deep vein thrombosis (DVT).
Results show both the novel predictive score (p=0.002) and the Parsonnet score (p=0.02) predict success in reaching the primary outcome. Euroscore was not shown to be a significant predictor (p=0.134) (Table 3).
Table 3. Results of univariate analysis comparing a novel predictive score for Procedural success against Euroscore and Parsonnet Score (pre-existing operative risk scores)
| Score |
Primary Outcome: Success (n=24) |
Primary Outcome:
Failure (n=22) |
P Value |
| Median Novel Predictive Score |
4.6 ± 2.6 |
7.4 ± 2.7 |
0.002 |
| Median Parsonnet Score |
11.0 ± 7.2 |
15.9 ± 8.2 |
0.020 |
| Median Euroscore |
5.1 ± 2.5 |
6.0 ± 2.0 |
0.134 |
ROC curve analysis is shown in figure 2. Area under curve (AUC) values show that the novel predictive scoring system has a predictive power of 0.7708. This was shown to be superior to Parsonnet score (0.6998). From this curve, a score of 8 points has the highest combined sensitivity and specificity and could potentially be used to distinguish between high and low risk of procedural failure.
Of 53 patients who received concomitant ablation therapy, 27 (50.9%) were recorded to be in sinus rhythm at a median follow up time of 12.6 months. This is consistent with randomised controlled trial data from Doukas et al. who found a 44.4% return at 12 months.18 However, a 2006 meta analysis by Barnett et al. (3225 patients) assessing the efficacy of concomitant surgical ablation found a higher mean of 84.5% freedom from AF at 1-year follow up.3
Lower rates of procedural success in this study could be linked to use of a restricted lesion set. All patients underwent pulmonary vein isolation with left atrial ablation and removal of the left atrial appendage. This is a safe and widely used method, as it requires only a single atriotomy, minimizing a patient’s time on bypass. Meta analysis has shown more complex biatrial ablation strategies are more effective in achieving long-term freedom from AF. Barnett et al. compared the results of 24 studies showing mean freedom from AF at one year post procedure was 88.9% in patients who had received biatrial ablation compared to 75.9% in those with left only.3
There was no difference in reduction of NYHA score between patients who succeeded or failed in reaching the primary endpoint. This may indicate that any symptomatic improvement is related to the primary procedure alone. It is however difficult to draw firm conclusions from NYHA score as it is a generalised score of functional capacity non-specific to AF.
The principle goals of returning patients to sinus rhythm are relieving the symptoms of AF and the reduction of thromboembolic risk. From the limited evidence presented here it could be suggested that the outcome of concomitant ablation has no effect on patient symptoms. In order to draw firm conclusions in future studies it would be necessary to use a more thorough score system with emphasis on symptoms related to AF.
Univariate analysis demonstrated that a larger proportion of patients who remained in sinus rhythm after a concomitant ablation procedure were originally suffering from paroxysmal AF. The reason for this is likely to be two-fold. Firstly it has been established that patients in nonparoxysmal AF are more treatment resistant due to more extensive changes in the electrophysiological substrate of the atria. Secondly due to the nature of paroxysmal AF, it is far more difficult to detect during follow up. Without the use of long term rhythm monitoring it is not possible to prove that paroxysms of AF are not present.
The novel scoring system proved to be superior to two well-established operative risk scores commonly used prior to cardiac surgery. It has the advantage of being based on a set simple criteria and can be applied to all patients in whom medical records and results of a preoperative echocardiogram are available.
Both univariate and receiver operating statistic analysis demonstrated the predictive power of our novel score system to be adequate. The next step in the evaluation of this system would be to test its use either prospectively, or in a larger retrospective cohort.
Levels of postoperative freedom from AF are likely to be overestimated. Due to poor attendance, only 27% of the total patients enrolled in the study received a 24-hour ECG or pacemaker rhythm check at their latest follow up. The remaining 73% were assessed using 12 or 3-lead ECG’s. A study by Ad et al. found that 12 lead ECG’s overestimated rates of procedural success by 12% when compared to 5 day rhythm monitoring. In the same trial 24-hour ECG’s were also shown to overestimate success by 7%. Long term rhythm monitoring (≥5 days) is the recommended strategy for accurately detecting paroxysms of AF.19 Some authors have suggested that internal loop recorders are the most accurate tool to assess AF burden.20 In a future prospective study longer term monitoring would be required to form a precise estimation of freedom from AF.
A novel scoring system was shown to predict procedural success in this small dataset. These results can be further validated through cooperation with other surgical centres and application of this score to larger patient cohorts.






