Atrial Fibrillation And Sleep Apnea: Considerations For A Dual Epidemic
Patricia Tung, MD1, Elad Anter, MD2
1Atrius Healthcare, Department of Cardiology, Boston, MA.2Harvard-Thorndike Electrophysiology Institute Cardiovascular Division, Department of Medicine Beth Israel Deaconess Medical Center Harvard Medical School, Boston, MA.
Atrial fibrillation (AF) is the most common cardiac arrhythmia and shares many of the same risk factors as another common clinical condition, sleep apnea. The estimated prevalence of sleep apnea has increased over the past decade, and reflects a parallel increase in the most prominent risk factors of obesity and overweight. Both obstructive and central sleep apnea have been associated with AF in multiple studies, with the risk of AF increasing 2-4-fold compared to those without sleep breathing disorder. Continuous positive airway pressure (CPAP) has been shown to reduce the rate of AF recurrence following catheter ablation in patients with sleep apnea. However, the mechanisms by which sleep apnea precipitates AF or vice versa, remain unclear. In this Review, we examine the current date linking AF and sleep apnea, discuss the existing data supporting a mechanistic link between the two conditions, present the existing evidence for the effectiveness of CPAP in this growing population, and suggest approaches to screen AF patients for sleep breathing disorders.
Key Words : Sleep Apnea, Atrial Fibrillation, CPAP, Outcomes, Arrhythmia Control.
Correspondence to: Elad Anter,Harvard-Thorndike Electrophysiology InstituteBeth Israel Deaconess Medical Center185 Pilgrim Rd, Baker 4, Boston, MA 02215.
Atrial fibrillation (AF) is the most commonly encountered arrhythmia in clinical practice. There are an estimated 33 million individuals with AF worldwide, with approximately 5 million new cases annually. The incidence and prevalence of AF increases with age, with a 2-3-fold increase between ages 60 and 80.1,2 Sleep disordered breathing (SDB), characterized by respiratory pauses of at least 10 seconds during sleep that result in oxyhemoglobin desaturation, is estimated to affect 17% of men and 9% of women aged 50-70.3 These estimates are significantly increased compared to two decades ago, and reflect a parallel increase in the most prominent risk factors for SBD, overweight and obesity.3 SDB encompasses a broad clinical spectrum ranging from mild airway resistance to prolonged apnea.
Obstructive sleep apnea (OSA), characterized by recurrent partial or complete collapse of the upper airway during sleep and associated with excessive daytime sleepiness, is estimated to affect 14% of men and 5% of adult women.3 In the developed world, the majority of OSA cases are secondary, occurring as a result of overweight and obesity.3 In secondary OSA, local fat deposition in the neck has been implicated as the cause of upper airway collapse and impaired neuromuscular control of the airway. In a small proportion of patients with clinical evidence of OSA, no abnormality of the upper airway can be identified on routine clinical examination. These individuals are considered to have idiopathic OSA. Previous work utilizing acoustic ultrasound and x-ray demonstrated that these individuals often have relatively small mandibles and posterior displacement of the mandibular symphysis, both of which affect the support to the anterior pharyngeal wall.4
Central sleep apnea (CSA) is characterized by diminished or absent respiratory effort during sleep, also associated with oxygen desaturation and daytime somnolence. In some cases of CSA, very shallow breathing can alternate with very deep breathing, as is the case with Cheyne-Stokes respiration. The estimated prevalence of CSA varies, but has been thought to account for up to one-fifth of all cases of SDB.5 Similar to OSA, CSA occurs most often secondary to an underlying condition such as heart failure, neuromuscular dysfunction or narcotic use. Primary or idiopathic CSA is quite rare, and results from decreased input to respiratory motor neurons. The causes of idiopathic CSA are not known.
Association Between AF And Sleep Apnea
Obstructive Sleep Apnea And AF
OSA has been shown to contribute to increased AF burden.1,6 Epidemiologic studies have identified a strong association of OSA and AF, with an increased risk for AF that is 2 to 4 times that of those without SDB.7,8 In a large, prospective, community-based cohort, Mehra and colleagues found that individuals with SDB had 4
times the odds of AF as those without SDB (OR 4.02, 95% CI 1.03-
15.74) after adjustment for age, sex, BMI and prevalent coronary
heart disease. A secondary analysis of the same cohort found no
dose-response relationship between risk for AF and severe to very
severe SDB.7 In contrast, Tanigawa et al observed that the risk of
AF was linearly associated with severity of SDB in a communitybased
study of Japanese men; the odds of AF increased more than
2-fold for those with 5-15 apneic or hypopneic events per hour (2.47,
95% CI 0.91-6.69) and more than 5-fold for those with >15 apneic
or hypopneic events per hour (5.66, 95% CI 1.75-18.34).9 Gami
et al prospectively assessed the risk of OSA, as determined by the
Berlin questionnaire among 524 patients with AF or atrial flutter
referred to a tertiary care center for cardioversion. After adjustment
for risk factors, AF was significantly associated with OSA, with AF
conferring twice the odds of OSA (OR 2.19, 95% CI 1.40-3.42)
compared to a general cardiology population without AF.10 Not all
studies, however, have shown an association between OSA and AF. In
a case-control study of patients with lone AF that excluded diabetics,
Porthan and colleagues observed that the prevalence of sleep apnea
in AF patients did not differ from those without AF (32% versus
29%, p=0.67).11 However, the number of subjects in this study was
small and the power to detect an association was therefore limited.
Central Sleep Apnea And AF
In clinical practice, OSA and CSA often coexist. Generally,
patients are considered to have CSA when more than 50% of their
apneic and hypopneic episodes are associated with reduced or absent
respiratory drive.5 As discussed above, this condition is prevalent
among particular populations such as those with heart failure and
primary neuromuscular disorders, and has also been associated with
AF. Sin et al found AF to be associated with CSA in a retrospective
analysis of 450 individuals with CHF referred to a tertiary care sleep
center.12 In this analysis, AF conferred a 4-fold increase in the risk
of CSA (4.13, 95% CI 1.53-11.4), but no increased risk for OSA.
An association between CSA and AF has also been observed in
community-based cohorts without overt heart failure or underlying
cardiac dysfunction. In an analysis of the Sleep Heart Health Study,
we demonstrated that CSA conferred double the risk for incident AF
(OR 2.06, 95% CI 1.23-3.44, p=0.0057) in an unselected population
without clinical signs of SDB.13 This association was also confirmed
prospectively by Leung et al in a population with presumed idiopathic
CSA, free of heart failure, coronary artery disease or stroke. The risk
of AF was higher in those with CSA (3.3% versus 1.7%, p<0.001)
than in those without SDB.14
Although the majority of evidence supports a strong association between sleep apnea and AF, it remains unclear whether SDB is
causal in the development of AF, as the two conditions share many
of the same risk factors. Furthermore, the mechanism by which
this may occur remains unclear. For example, obesity is a common
risk factor for SDB and AF. But whether the link underlying the
association is obesity itself or resulting effects on left atrial pressure
and size, inflammatory and pro-fibrotic molecules, insulin resistance,
or increased mean arterial blood pressure and atrial fibrosis is
unknown. It has been suggested that the physiologic changes of
SDB including intermittent hypoxia, hypercarbia, and intrathoracic
pressure fluctuations predispose to arrhythmia through electrical and
structural remodeling.15
The proposed mechanism by which hypoxia promotes AF is via
autonomic nervous system dysfunction and electrical remodeling. In
a dog model of intermittent hypoxia, Lu and colleagues found that
hypoxia initially resulted in parallel changes in heart rate variability
(HRV) indices associated with sympathetic and parasympathetic
activity such that the atrial effective refractory period (AERP) and
AF vulnerability were not affected.16 However, with repeated hypoxic
episodes, the parasympathetic indices of HRV were increased to a
greater extent relative to sympathetic indices, and the AERP and
AF vulnerability were also increased. This suggests that autonomic
system imbalance may precipitate electrical changes in the atria
that predispose to AF. Autonomic nervous system dysfunction is
further supported in the development of AF based on studies of
CSA patients in whom increased concentrations of plasma and
urinary norepinephrine and epinephrine have been documented,
independent of left ventricular dysfunction.17
Hypercarbia has also been implicated in electrical remodeling. In
a sheep model, Stevenson et al found an inverse linear association
between the effective refractory periods of the right and left atria and
end-tidal CO2 levels in hypercarbic sheep that was not present in
the hypoxic or control sheep.18 In addition, atrial conduction times
during pacing at a constant cycle length and during extrastimulus
testing were significantly prolonged during and after resolution of
hypercapnia. In contrast, no corresponding changes in conduction
times were observed in the hypoxic or control sheep during or
after resolution of hypoxia. Interestingly, AF vulnerability was
eliminated during hypercapnia but was significantly increased
following resolution of hypercapnia and normalization of ERP. This
suggests that hypercapnia may not promote AF acutely, but rather
may promote electrical substrate remodeling over time after repeated
exposure.
There is also data suggesting that hypercapnia can result in cardiac
structural changes. In studies of ventricular myocytes isolated from
rat hearts, White et al observed that exposure to medium with
high levels of CO2 resulted in decreased cell to cell conduction.19
Vorperian and colleagues exposed anesthesized dogs to an elevated
mixture of inhaled CO2 with resultant decrease in serum pH. They
found that hypercarbia resulted in slowed propagation of impulses
in the transverse direction, perhaps due to connexin dysfunction.20 However, it is unclear why these changes would occur selectively in the transverse rather than longitudinal direction and whether these
structural changes occur in the atrium as well.
Fluctuations in intrathoracic pressure have also been implicated
in electrical remodeling.21 Sympathetic stimulation during acute
episodes of tracheal obstruction can produce increased intracellular
calcium load, leading to shortening of action potential duration and
initiation of AF.22-24 In a porcine model, Linz and colleagues simulated
tracheal occlusion with and without the application of negative
intrathoracic pressure (NTP).25 They found a significant decrease
(161 versus 96 ms, p<0.0001) in the atrial effective refractory period
(AERP) after two minutes of tracheal occlusion with -100mbar. In
contrast, tracheal occlusion without NTP had no effect on AERP.
The change in AERP was associated with increased inducibility of
AF (0% normal breathing or tracheal occlusion without NTP versus
91% with NTP). Linz also investigated the effect of autonomic
changes; atropine prevented AERP shortening in NTP, did not affect
the AERP during normal breathing and decreased AF inducibility
with NTP from 91% to 17%. These data suggest that negative
intrathoracic pressure can precipitate electrophysiologic changes
that increase the inducibility of AF, and that these changes may be
mediated by an autonomic effect.
There is also evidence of structural remodeling resulting from
repeated episodes of OSA with fluctuating intrathoracic pressure.
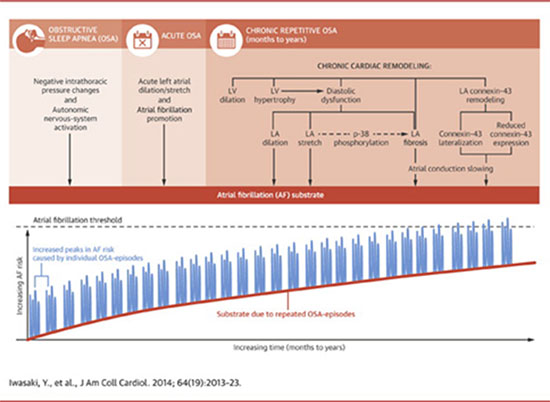
Iwasaki and colleagues created a rat model of OSA, in which the
airway of intubated rats was occluded at end expiration for 40s
followed by an 80s recovery period 20 times per day, 5 days per week
for 4 weeks. After OSA cycles, rats were ventilated with room air and
then extubated.26 This group was compared to rats subjected to the
same ventilator-arrest cycles but without airway closure, and to rats
ventilated with room air throughout the procedure. OSA produced a
statistically significant increase in left atrial dilation that was not seen
in the sham or control groups. No significant differences in atrial ERP
or sinus node recovery time was found between the groups. However,
conduction velocity was decreased, and AF inducibility and mean AF
duration were increased significantly (p<0.05) in OSA rats compared
with sham rats. The investigators also observed structural differences
between the groups; there was increased fibrosis, decreased expression
of connexin-43, and a lateralized distribution of this protein in OSA
rats compared to sham and control rats. These structural changes may
explain the changes in conduction velocity and inducibility of AF in
the absence of changes in atrial refractoriness.
Ramos et al also created a rat model of OSA and similarly
demonstrated increased atrial fibrosis (11.9 versus 8.32, p<0.01)
in OSA rats compared to sham rats.27 Amounts of angiotensinconverting
enzyme were significantly increased, and matrix
metalloproteinase-2 significantly decreased, in OSA rats compared
to sham rats.27 Thus, OSA may also predispose to AF through a
mechanism of left atrial fibrosis. Taken together, there is a growing
body of evidence that suggests that the physiologic effects of chronic
SDB predispose to AF via electrical and structural remodeling that
occurs over time (Figure 1)
Figure 1 Mechanisms by Which OSA Leads to AF
There is data from humans supporting electrical and structural
remodeling secondary to OSA. Dimitri et al compared
electrophysiologic parameters among 20 patients with OSA
and 20 without OSA undergoing ablation for paroxysmal AF.15
Electroanatomic maps of the right and left atria were obtained in all
patients to compare the voltage, conduction velocity and distribution
of complex atrial electrograms. There was no difference in the
right or left atrial refractory periods between those with OSA and
those without (p=0.9). However, patients with OSA had prolonged
conduction times along the coronary sinus and RA (p=0.02), a
longer corrected sinus node recovery time (p=0.02), and a greater
number (p=0.003) and duration (p=0.03) of complex electrograms
along the crista terminalis. OSA patients also had a longer p wave
duration (p=0.01), lower atrial voltage (RA p<0.01, LA p=0.02),
slower atrial conduction velocity (RA p=0.001, LA p=0.02) and
more complex electrograms in both atria (RA p=0.02, LA p=0.01)
compared to those without OSA.15 In prior studies, p wave duration
and dispersion, measures of prolonged and heterogeneous atrial
conduction have been found to correlate with severity of OSA.28,29
These data suggest a possible difference in underlying atrial substrate
between AF patients with and without sleep apnea.
Clinical Outcomes And Effect Of CPAP Treatment
In humans, OSA confers increased risk of recurrent AF that is
mitigated by CPAP therapy. In a population of patients with AF
and atrial flutter referred for electrical cardioversion, Kanagala
and colleagues found that untreated OSA was associated with
increased AF recurrence.30 Of the 39 patients with OSA, 27 were
not receiving CPAP therapy (n=25) or were using it inappropriately
(n=2). Among those with OSA, patients receiving CPAP had a lower
rate of recurrence of AF at one year than those not receiving CPAP
(42% versus 82%, p=0.013). Importantly, the recurrence rate among
CPAP-treated patients was similar to control patients without OSA.
Additionally, in the 25 patients with untreated OSA, the nocturnal
oxygen desaturation was greater among those with recurrent AF
(n=20) compared to those without AF recurrence (n=5, p=0.034).
The effect of OSA and CPAP has also been examined among
patients undergoing catheter ablation of AF. Patel et al evaluated
3,000 consecutive patients undergoing pulmonary vein isolation
between January 2004 and December 2007, of which 640 (21.3%)
were identified as having OSA. Overall, patients with OSA had
a statistically significant increase in procedural failures (p=0.024)
compared to patients without OSA. Among those with paroxysmal AF, OSA patients had more non-pulmonary vein triggers and
posterior wall firing than patients without OSA (20% versus 8%,
p<0.001). This was also true in non-paroxysmal AF patients; patients
with OSA had more non-pulmonary vein triggers than those without
OSA (31% versus 19%, p = 0.001). Importantly, treatment with
CPAP reduced the rate of AF recurrence (79% versus 68%, p=0.003).
The presence of non-pulmonary vein triggers and absence of CPAP
use strongly predicted ablation failure (HR 8.81, p<0.001).
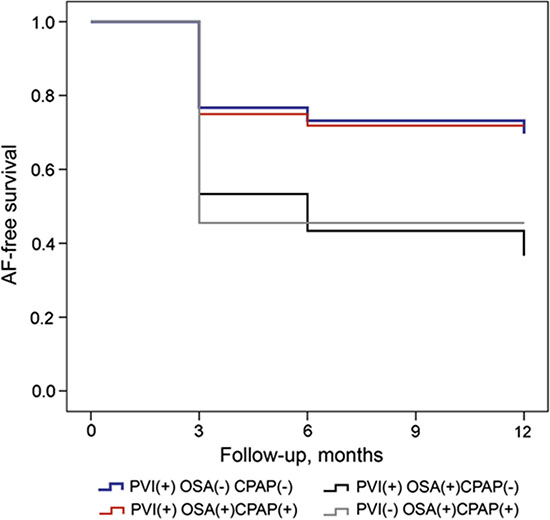
We found a similar pattern of outcomes when we examined 426
consecutive patients undergoing PVI between 2007 and 2010 at our
institution. Sixty-two patients had a diagnosis of OSA confirmed by
polysomnography, of which 32 were identified as receiving CPAP
therapy. At one year following first PVI, 71.8% of OSA patients using
CPAP were free of AF recurrence as compared to 36.7% of OSA
patients not using CPAP (p=0.01). Survival analysis demonstrated
that the rate of recurrence among CPAP-treated individuals was
similar to that of patients without OSA at 1 year (67% versus 71.8%,
p=0.94). In addition, AF-free survival off antiarrhythmic medications
was higher among CPAP users compared to non-users (65.6% versus
33.3%, p=0.02; Figure 2).
Figure 2 Kaplan-Meier Survival Curves According to Treatment Group
In another recent study, the results of polysomnography were
compared between patients with and without SDB who have
undergone catheter ablation for AF. Naruse et al obtained overnight
polysomnograms in 153 patients who had undergone pulmonary
vein isolation one week earlier.31 One hundred sixteen of the 153
patients (76%) were diagnosed with OSA. Over a mean follow-up
period of 18 months, AF recurrence in OSA patients not receiving
CPAP was higher than in those without OSA as well as those with
OSA on CPAP therapy (53% versus 22% versus 33%, respectively;
p<0.01). After controlling for LA volume, plasma NT-pro-BNP and
LVEF on multivariate analysis, CPAP use was found to decrease the
risk of AF recurrence. In Cox model analysis, there were higher rates
of AF recurrence following ablation in those with OSA, (HR 2.61,
p=<0.05) and improved rates of arrhythmia control among those
treated with CPAP (HR 0.41, p<0.01).31
A meta-analysis of the effect of OSA on outcomes following
catheter ablation of AF by Ng and colleagues found a 25% increased
risk of AF recurrence after ablation in OSA patients compared to
those without OSA (RR 1.25, 95% CI 1.08 to 1.45, p = 0.003). In
secondary analyses, this increase in risk appeared to be present among
those diagnosed with OSA according to overnight PSG (RR 1.40,
95% CI 1.16 to 1.68, p = 0.0004), but not among those diagnosed
with OSA by the Berlin Questionnaire (RR 1.07, 95% CI 0.91 to
1.27, p = 0.39).32 A more recent metaanalysis examined 7 studies
with a total population of 1,087 individuals.33 They found that the
relative risk reduction of CPAP on AF recurrence ranged from 30%
to 56%, with an overall risk reduction of 42% for CPAP (RR 0.58,
95% CI 0.51-0.67, p<0.001). Interestingly, the same magnitude of
risk reduction of CPAP on AF recurrence was observed in those who
underwent PVI as well as those who did not undergo ablation. Table 1 summarizes the studies that have evaluated the effect of OSA on
AF recurrence following catheter ablation.
Table 1. Summary of Studies Examining the Effect of OSA on AF Recurrence
| Study |
Number Patients |
Mean Age |
OSA Diagnosis |
Mean Follow-Up |
% PAF |
Ablation Strategy |
Method of AF Detection |
| Patel et al31 |
3,000 |
55.7 |
PSG |
32 mo |
53.4 |
PVI + LA linear ablation |
Event monitor + 48h Holter |
| Matiello et al47 |
174 |
52.5 |
PSG |
12 mo |
56.3 |
PVI + LA linear ablation |
Holter |
| Chilukuri et al48 |
109 |
605 |
Berlin |
11 mo |
68 |
PVI |
ECG + telephone, Event monitor for symptoms |
| Tang et al49 |
178 |
57.2 |
Berlin |
344 days |
100 |
PVI |
ECG + 24h Holter |
| Chilukuri et al50 |
210 |
58 |
Berlin |
25 mo |
57 |
PVI |
ECG + telephone, Event monitor for symptoms
|
| Jongnarangsin et al51 |
324 |
57 |
PSG |
7 mo |
72 |
PVI + CFAE |
ECG + 30d autotrigger monitor |
| Naruse et al33 |
249 |
60 |
PSG |
18.8 mo |
54 |
PVI + LA linear ablation |
ECG |
| Fein et al32 |
426 |
56.8 |
PSG |
12 mo |
57 |
PVI + LA linear ablation |
ECG and Event monitorr |
Finally, the effect of CPAP on AF progression was recently
examined in the Outcomes Registry for Better Informed Treatment
of Atrial Fibrillation (ORBIT-AF).34 In this analysis of 10,132
patients with AF enrolled in a nationwide registry, Holmqvist and
colleagues documented an 18% prevalence of OSA. Those with
OSA were more symptomatic, had greater rates of interventions
for AF and higher rate of hospitalization, but a comparable risk of
death, stroke, and myocardial infarction. The rate of AF progression
was similar between the OSA and no OSA group (HR 1.06, 95%
CI 0.89-1.28, p=0.51). Similarly, no difference in the risk of death,
stroke, and myocardial infarction was observed between those on
CPAP compared to those not receiving CPAP therapy. However, the
rate of AF progression for those receiving CPAP therapy was lower
than those with OSA not on CPAP, as well as those without OSA
(HR 0.66, 95% CI 0.46-0.94, p=0.02).
CPAP therapy may reduce AF recurrence by preventing or reversing
the structural changes of SDB. In a prospective, single center study
of patients undergoing cardiac MRI prior to PVI, patients with sleep
apnea on shorter duration of CPAP therapy were more likely to have
persistent than paroxysmal AF, as well as increased LV mass, larger LA
dimensions and lower right ventricular ejection fraction.35 Bayir and
colleagues obtained echocardiograms of 30 patients with moderate to
severe OSA and free of cardiovascular disease, at baseline and after
6 months of CPAP therapy. They found significant reductions in
inter-atrial (39.2 versus 28.7ms, P<0.0001, left atrial (20.5 versus
15.6ms, p=0.002) and right atrial (20.7 versus 13.1ms, p<0.0001)
conduction times. Measures of diastolic dysfunction (E/A ratio 0.9
versus 1.1, p<0.0001) were also improved after CPAP.(36) Effects
of CPAP have been shown to decrease LA volume as well as LV
systolic and diastolic dysfunction.37-39 One study of 37 patients with
chronic heart failure found that CPAP did not affect blood pressure,
heart rate or cardiac output significantly.40 Thus, CPAP may produce
physiologic changes that result in decreased LA size and filling, and
which reduce the rate of AF recurrence by decreasing filling pressures
and preventing substrate changes. However, this study was designed
to demonstrate that CPAP in patients with severe heart failure does
not lead to hemodynamic compromise, and thus was limited in its
ability to shed light on underlying mechanism of CPAP effect.
Alternatively, CPAP may reduce AF recurrence by mitigating
AF triggers. A temporal association between SDB and arrhythmic
events has been shown,41 in which the risk for AF is significantly
increased in the immediate post-apneic period, suggesting that SDB
may also constitute a trigger for AF. This again suggests that CPAP
may modulate the triggers, rather than the substrate for AF. These
findings have direct clinical relevance as AF ablation in patients
with OSA may require an ablation strategy that emphasizes nonpulmonary
vein triggers.
The American Academy of Sleep Medicine considers those with AF
to be high risk for SDB and recommends evaluation for sleep apnea
in these individuals.42 However, this has not yet become standard
practice primarily because sleep apnea remains under-suspected and
under-diagnosed by electrophysiology physicians treating patients
with AF. In addition, overnight sleep studies are cumbersome and
a mechanism for coordinating sleep apnea screening and treatment
referral has not been established in electrophysiology clinics. Given
the clear evidence for improved arrhythmia control with CPAP
therapy following cardioversion and catheter ablation of AF, it
remains to be seen whether ablation and antiarrhythmic therapy offer
benefit to patients with SDB in the absence of CPAP treatment.
In the future, a multidisciplinary approach that involves screening
all patients with AF for OSA, and referral to a sleep specialist may
become the standard of care.
The gold standard for the diagnosis of sleep apnea is overnight
polysomnography, typically conducted in a sleep laboratory, which
can be costly and cumbersome for patients. However, these are
cumbersome and are less and less covered by insurance companies.
Home sleep studies have recently obtained FDA approval for
diagnosis of sleep apnea and offer patients and treated physicians
the opportunity to assess the presence of SDB in a natural sleeping
environment, and often time in timely fashion. All currently available
home sleep study devices are able to diagnose OSA, though not
all have been validated for use in patients with AF. Some home
sleep testing devices also have thoracic impedance bands to allow
diagnosis of CSA. Comparisons of portable sleep devices and
polysomnopgraphy for the diagnosis of OSA demonstrated good
sensitivity and specificity (95.3% and 75%, respectively)43 and
correlation and accuracy (AUC difference=0.04)44 between major
clinical indices such as apnea hypopnea index and respiratory
disturbance index.
Atrial fibrillation is the most common cardiac arrhythmia and shares
many of the same risk factors as another common clinical condition,
sleep apnea. There is a clear association between both obstructive and
central sleep apnea and risk for AF. Several studies have shown a link
between some of the physiologic changes of SDB and AF, and CPAP
has in some cases been shown to reduce the rate of AF incidence
and recurrence following catheter ablation in patients with SDB.
However, further study is needed to establish a clear mechanistic link
between the two conditions.
There are an estimated 5 million new cases of AF per year,
which represents a significant proportion of health care costs and
morbidity.1 Gaining insight into the mechanistic role of SDB in the development of AF is key to successful AF prevention and treatment
strategies. Additional studies are needed to better understand the
mechanism underlying the associations between SDB and AF. In
particular, prospective studies examining the feasibility and impact of
universal screening for diagnosis and treatment of SDB in patients
with AF on arrhythmia outcomes and patient well being are needed.
Atrial fibrillation (AF) and sleep apnea have been associated in
multiple studies, with a risk for AF that are 2 to 4 times that of those
without sleep disordered breathing. There is emerging evidence from
animal and human studies that the physiologic changes of sleep
apnea including hypoxia, hypercapnia and intrathoracic pressure
fluctuations precipitate electrical and structural changes. Some of
these changes occur acutely after an apneic episode, while others
occur with repeated exposure over time. There is also evidence that
continuous positive airway pressure (CPAP) may reverse some of
these changes, thereby reducing the risk for AF recurrence after
cardioversion and ablation. However, a detailed understanding of
the mechanisms by which sleep apnea precipitates electrical and
structural remodeling remains unknown. Further studies are needed
to evaluate the feasibility of universal screening for SDB, and the
effect of therapy on both the development and progression of AF.






