Anemia, defined as a reduced hemoglobin concentration or hematocrit value, is one of the most common disorders globally affecting about 24.8% of the overall world population.1 The prevalence of anemia is higher in older people and seems to increase with aging and with increased comorbidity burden. For example, the prevalence of anemia is about 11% in men and 10.2% in women aged 65 years and about 25% in men and 20% in women above the age of 85 years.2 In the frail older population living in care homes the anemia prevalence is even much higher reaching around 48% to 63% of the total residents reflecting their multiple comorbidities and advanced age.3 Similarly, atrial fibrillation (AF), the most common sustained cardiac arrhythmia, is age dependent and its prevalence doubles with each decade of life from 0.55% at the age of 50 to 60 years reaching about 12% in those above the age of 75 years with an annual incidence of around 2%.4 Therefore, AF appears to affect mainly older people with about 80% of the total AF population are 65 years of age or older and by the year 2050, this percentage will increase to around 88%.5 Patients with AF have twice the mortality risk compared to those in sinus rhythm likely due to the associated comorbidities, including anemia, in AF patients.6 Anemia commonly coexists with chronic conditions such as heart failure and diabetes mellitus and appears to be an independent predictor of adverse outcomes associated with these conditions.7,8 AF, as a chronic condition, is not an exemption and this review explores the relationship between anemia and AF and its role as an independent predictor of adverse outcomes in patients with AF.
We have performed a search of Medline and Embase from January 1969 to November 2015 using keywords relating to anemia, atrial fibrillation and adverse outcomes. Only English language articles were selected. Articles were reviewed for relevance by abstract. A manual review of citations in retrieved articles was performed in addition to the electronic literature search. The final list of cited references was chosen on the basis of scientific quality and relevance to the topic of review.
Does anemia precipitate new onset AF?
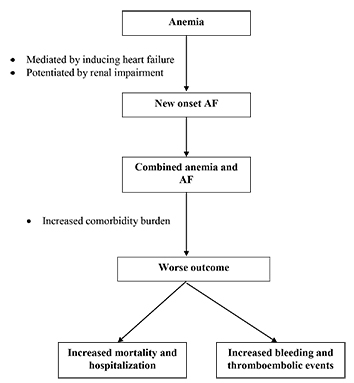
The answer to this question is still not clear. It appears that the relationship between anemia and new onset AF is complex especially in the presence of comorbid chronic kidney disease (CKD) or heart failure. Recently, it has been shown that anemia, defined as a hemoglobin of <13 g/dL, was 1.5 times more likely to be associated with new onset AF in a Japanese 15-year prospective cohort study of 132,250 subjects aged 40 to 79 {hazard ratio (HR) 1.50, 95% confidence interval (CI) 1.24 to 1.83, p<0.0001} compared to normal hemoglobin level. CKD, defined as an estimated glomerular filtration rate (eGFR) of <60 mL/min/1.73m2, was 2.56 times more likely to be associated with new onset AF (2.56, 2.09 to 3.13, p<0.0001) compared to normal kidney function. The combination of CKD and anemia conferred a synergistic threefold higher risk for new onset AF (3.22, 2.43 to 4.19, P<0.0003) which is higher than would have been expected from the individual effects of CKD or anemia alone. Borderline hemoglobin level increased the risk for new onset AF only in patients with CKD but not in patients with normal kidney function confirming the synergistic action between anemia and CKD in precipitating new onset AF. This may be due to the fact that the pathogenesis of both AF and CKD is associated with common risk factors such as advancing age, hypertension and diabetes mellitus in addition to the hemodynamic changes associated with anemia itself such as reduced oxygen carrying capacity which may contribute to the susceptibility of new onset AF development.9 In another retrospective cohort study of Medicare patients without pre-existing AF or end stage renal disease who were followed up from 2006 to 2008, advanced CKD and anemia were independently associated with incident AF (HR 1.13, 95% CI 1.09 to 1.18, p<0.0001 and 1.05, 1.03 to 1.07, p<0.0001 respectively). No synergistic effect between renal function and anemia was investigated in this study.10 The onset of anemia may be another determinant factor for the new onset AF precipitation. Chronic anemia alone was not directly associated with incident or prevalent AF in one study.11 In a single center community based retrospective study of 3,867 patients over the age of 65 years, new onset AF was found in 7.5 % of the anemic patients and 5.5% of the non-anemic patients however, after the adjustment for comorbid conditions, chronic anemia was not associated with new onset AF (p=0.922). Chronic anemia seems to require other comorbid factors like heart failure to precipitate AF as suggested in this study cohort.11 The cardiac effects of the acute onset may be different from the chronic onset anemia. Baseline cardiac status, severity and rapidity of the onset of anemia may affect cardiac hemodynamics. For example, in acute anemia hemodynamic stress occurs due to the acute drop in hemoglobin concentration leading to tachycardia, as a compensatory physiologic response, that may leave less time for the heart to adapt. On the other hand, the gradual decrease in hemoglobin levels in chronic anemia could allow the heart to adapt before heart failure or AF develops making chronic anemia better tolerated. Other factors specific to old age such as reduced muscle mass, reduced exercise capacity and reduced sympathetic responses may lead to reduced oxygen demands and assist in the adaptation to the gradual decrease in hemoglobin levels in chronic anemia. It is possible that chronic anemia, if left untreated, may reach a threshold to precipitate heart failure first as an intermediate stage and subsequently precipitates AF. Therefore, patients with combined heart failure and anemia are likely to be at a higher risk for incident AF compared to those with anemia alone. In summary, anemia especially with acute onset appears to precipitate new onset AF mediated by inducing heart failure first and potentiated by the presence of renal impairment.
Anemia increases the comorbidity burden of patients with AF
Patients with AF often have other cardiovascular comorbidities such
as chronic heart failure, stroke, valvular heart disease, hypertension
and diabetes mellitus.12 The co-existence of anemia and AF further
increases this comorbidity burden. For example, in the Fushimi-Japan
AF Registry, patients with anemia and AF had higher prevalence of
comorbidities compared to those with AF alone. They were older,
mean (SD) age 79.6 (10.3) vs. 73.4 (10.5) years, p<0.001, had more
prevalence of heart failure (43.1% vs. 25.8%, p<0.001), coronary
artery disease (19.5% vs. 14.8%, p=0.006), peripheral arterial disease
(6.2% vs. 4.2%, p=0.04), chronic kidney disease (52.5% vs. 22.3%,
p<0.001) and history of major bleeding (4.2% vs. 1.5%, p<0.001).
They tended to have a higher thromboembolic risk with greater
mean (SD) CHA2DS2-VASc scores, 4.22 (1.64) vs. 3.35 (1.68),
p<0.001, a higher prevalence of previous stroke (25.8% vs. 18.6%
p<0.001) and received less oral anticoagulation therapy (44.4% vs.
52.4%, p<0.001).13 In the prospective multicenter Atrial Fibrillation
undergoing Coronary Artery Stenting (AFCAS) study, anemic
patients with AF were older, more often had diabetes, CHA2DS2-
VASc score >4, HAS-BLED score ≥3, prior history of heart failure,
chronic renal impairment and acute coronary syndrome (p<0.05 for
all) compared to those with AF alone.14 Characteristics of patients
with combined AF and anemia compared to those with AF alone are
summarised in Box 1 .
Box 1. Characteristics of patients with combined anemia and AF.* 13,14
| • Older |
| • More prevalence of: |
| Heart failure |
| Coronary artery disease |
| Acute coronary syndrome |
| Peripheral arterial disease |
| Chronic kidney disease |
| Diabetes mellitus |
| Stroke |
| • Higher scores in bleeding risk scales |
| • Higher history of major bleeding events especially gastrointestinal bleeding. |
| • Higher scores on thromboembolic risk scales |
| • Higher thromboembolic events |
| • Receive less oral anticoagulation therapy |
| • Higher rate of oral anticoagulation therapy discontinuation |
| • Higher mortality rate |
| • Higher hospitalization rate |
*Compared to those with AF alone.
Anemia and adverse outcomes
Anemia is associated with chronic conditions and appears to increase the comorbidity burden of these conditions leading to
adverse outcomes including increased mortality.7-8 AF, as a chronic
condition, is not an exemption and patients with comorbid anemia
and AF appear to have a worse outcomes compared to those with
AF alone.
Hospitalization and mortality risks
Anemia is an independent predictor of mortality and hospitalizations
in older people with AF independent of the demographic factors,
comorbid conditions or the use of cardiovascular medications. In
a retrospective study of 13,067 Medicare beneficiaries in the US,
mean age 79.8 years, hospitalized with AF, Hematocrit (Hct) was
significantly (P <0.0001) associated with increased risk of death
and re-hospitalisation. Patients in the lowest Hct category (<25%)
had the worst survival, whereas patients with Hct’s of 40% to 44.9%
or 45% to 49.9% had the most favorable survival. The trend was
of an increasing risk of mortality with a decreasing Hct value. In
comparison to Hct of 40% to 44.9%, the adjusted HRs for all cause
mortality were 1.66 for Hct <25%, 1.50 for 25% to 29.9%, 1.28 for 30%
to 34.9% and 1.07 for 35% to 39.9%. The risk of re-hospitalization
was 1.28 fold higher in the Hct category 25% to 29.9% (adjusted
HR 1.28, 95% CI 1.15 to 1.43) compared to the category 40% to
44.9% after one year of follow up.15 In another prospective study
of 166 patients, mean (SD) age 71.0 (10.0) years, with persistent
AF referred for echocardiographic examination in Taiwan, low
hemoglobin concentration was also a predictor of cardiovascular
events (mortality and hospitalization). Fifty four patients had
anemia, mean (SD) hemoglobin 11.0 (1.4) g/dl compared to 112 non
anemic subjects, mean (SD) hemoglobin 14.6 (1.2) g/dl, p=0.001. In
the multivariate analysis hemoglobin was independently associated
with increased cardiac events (HR 0.83, 95% CI 0.71 to 0.96, P =
0.015) after an average of 20 months follow up. The addition of hemoglobin to the clinical and echocardiographic data significantly
improved the prediction of adverse cardiac events (P = 0.010).16 In a
Danish nationwide retrospective study, patients with AF were more
likely to be admitted to hospital compared to those in sinus rhythm.
When adjusted for age, sex and time period, patients with AF had
a relative risk of 8.6 (95%CI 8.5 to 8.6) for cardiovascular related
admissions and 4.0 (95% CI 4.0 to 4.0) for non-cardiovascular related
admissions. Anemia was identified as an independent predictor of
hospital admissions increasing hospitalization by almost 4 folds in
patients with compared to those without AF {Relative risk (RR) 3.8,
95% CI 3.7 to 3.8} and was also associated with a longer mean length
of hospital stay (6.3 vs 5.6days).17 Heart failure events defined as an
increased mortality or hospitalization were independently increased
by the presence of anemia in a prospective Japanese study of 1942
patients (HR 3.01, 95% CI 1.78 to 5.10, p<0.001). Anemia diagnosis
formed a part of a risk score to identify patients with AF who are
at risk for the incidence of new hospitalization or death with a
diagnosis of heart failure (the H2ARDD score: 2 points for heart
diseases, 1 point for anemia, 1 point for renal dysfunction, 1 point for
diabetes and 1 point for diuretic use).18 In the primary care, anemia
was also identified as a risk factor for hospitalisation or mortality
(HR 1.37, 95% CI 1.08 to 1.75, p=0.01) in a cohort of 798 patients
with AF followed up for a mean (SD) of 2.8 (0.7) years.19 The
presence of anemia was associated with the composite endpoint of
all-cause mortality or myocardial infarction (adjusted HR 1.50, 95%
CI 1.32 to 1.71) in a retrospective analysis of the RE-LY study, allcause
mortality (adjusted HR 1.68, 95% CI 1.46 to 1.93, p<0.0001)
in the Apixaban for Reduction in Stroke and Other Thromboembolic
Events in Atrial Fibrillation (ARISTOTLE) trial and of all-cause
mortality at 12-month follow-up (HR 1.62, 95% CI 1.05 to 2.51,
p=0.029) in the AFCAS study.20,21,14 Anemia likely to increase
hospitalization through increasing adverse events. For example, after
one year of follow up of the Fushimi-Japan AF Registry, patients
with anemia had more heart failure related (7.4% vs 3.7%, p<0.01)
and more major bleeding related hospitalisation (3.2% vs 1.3%,
0.01) and in a national registry study of 26,345 patients with AF,
anemia was an independent risk factor for major bleeding that led to
hospitalisation (HR 2.36, 95% CI 1.76 to 3.17).22,23 (
Table 1)
Table 1. Studies on anemia as a predictor of mortality or hospitalization in patients with AF
| Study |
Population |
Aim To |
Main findings |
| Puurunen, 2014 14 |
861 patients with AF undergoing PCI |
Analyse impact of anemia on outcome of patients with AF undergoing PCI |
Anaemia predicted all cause mortality (HR 1.62, 95% CI 1.05 to 2.51, p=0.029) |
| Sharma, 2009 15 |
13,067 Medicare beneficiaries hospitalized with AF |
Investigate the association of
anemia with mortality and hospitalizations in patients with AF |
Anemia predicted mortality (HR 1.66, 95% CI 1.28 to 2.17) and hospitalization (1.28, 1.15 to 1.43) |
| Lee, 2015 16 |
166 patients with AF |
Investigate role of anemia in predicting CV outcome. |
Anemia predicted mortality and hospitalization (HR 0.83, 95% CI 0.71 to 0.96, P=0.015). |
| Christiansen, 2013 17 |
729,088 patients with AF associated hospitalization |
Examine the excess risk of hospitalization
in patients with AF
|
Anemia increased risk of hospitalization (RR 3.8, 95% CI 3.7 to 3.8) |
| Suzuki, 2012 18 |
1942 patients with AF |
Identify predictors of heart failure events in patients with AF |
Anemia increased risk of mortality or hospitalization (HR 3.01, 95% CI 1.78 to 5.10, p<0.001) |
| Vidal-Perez, 2013 19 |
798 patients with AF in primary care. |
Describe predictors of mortality or hospitalization. |
Anemia predicted end points (HR 1.37, 95% CI 1.08 to 1.75, p=0.010) |
| Westenbrink, 2015 20 |
18,113 patients with AF in RE-LY study |
Determine if anemia predicts
CV events
|
Anemia predicted all cause mortality or myocardial infarction (HR 1.50, 95% CI 1.32 to 1.71) |
| Westenbrink, 2014 21 |
18,201 patients with AF in ARISTOTLE study |
Test whether anemia predicts CV outcomes |
Anemia predicted all cause mortality (HR 1.68, 95% CI 1.46 to 1.93, p<0.0001) |
| Takabayashi, 2014 22 |
3,821 patients with AF in Fushimi study |
Test relationship between anemia and heart failure in patients with AF |
Anemia predicted heart failure hospitalization (OR 1.6, 95% CI 1.00 to 2.36, p=0.049) |
PCI= Percutaneous coronary intervention, CV=Cardiovascular, HR=Hazard ratio, CI=Confidence interval, RR=Relative risk, OR=Odds ratio.
Bleeding and thromboembolic risks
Anemia has been shown to be associated with an increased risk
of thromboembolic and bleeding events in anticoagulated patients
with AF. A retrospective analysis of 17,796 patients with available
hemoglobin results in the RE-LY study showed that anemia was
present in 12% of the population at baseline and the presence of
anemia was associated with stroke or systemic embolism (adjusted
HR 1.41, 95% CI 1.12 to 1.78). Anemia was also associated with a
higher risk of major bleeding complications (adjusted HR 2.14, 95%
CI 1.87 to 2.46) and discontinuation of the anticoagulant therapy
(adjusted HR 1.40, 95% CI 1.28 to1.79). The association between
anemia or hemoglobin and the different cardiovascular endpoints
did not differ according to gender, major comorbidities, treatment
allocation, eGFR, aspirin use or prior use of warfarin. The incidence
of events was lower in patients with transient anemia than in patients
with chronic anemia (adjusted HR 0.66, 95% CI 0.49 to 0.91).
Anemia remained a predictor of bleeding complications, even after
adjustment for the HAS-BLED score. During the course of the
study, patients with anemia spent more time below the therapeutic
range than those without anemia (26% vs. 22%, P < 0.0001), whereas the times above the therapeutic range were comparable.20 In the
AFCAS study of 861 patients, anemia was common affecting
30% of AF patients and was associated with major adverse cardiac
and cerebrovascular thrombotic events (29.1% vs 19.4%, p=0.002)
and minor bleeding events (7.0% vs 3.3%, p=0.028) compared to
those without anemia. The incidence of stent thrombosis was also
significantly higher in anemic versus non-anaemic patients (3.9%
vs 0.7%, p=0.002).29 The thromboembolic events associated with
anemia seem to also affect the functional outcome. In the Acute
STroke Registry and Analysis of Lausanne (ASTRAL) study, AF
was more common in patients with compared to those without
anemia (33.5% vs 25.2%, p<0.001) and the presence of anemia was
a predictor of worse stroke functional outcomes as well as short and
long term mortality.24 In the ARISTOTLE trial anemia predicted
major bleeding (adjusted HR 1.92, 95% CI 1.62 to 2.28, p<0.0001).
Patients with anemia were older (median 73 vs. 69 years), had
higher mean CHADS2 score (2.4 vs. 2.1), and were more likely to
have experienced previous bleeding events (mean 20.1% vs. 16.2%)
compared to those without anemia.21 Pre-existing anemia was
associated with major bleeding ((β=0.457, p=0.02) in a retrospective
Japanese study of 184 patients with AF on dabigatran treatment after
a mean (SD) follow up of 383 (190) days. The baseline hemoglobin
concentration also correlated negatively (r=-0.160, p=0.03) with the
development of major bleeding.25 In the Rivaroxaban Once-daily Oral
Direct Factor Xa Inhibition Compared with Vitamin K Antagonism
for Prevention of Stroke and Embolism Trial (ROCKET) in Atrial
Fibrillation, anemia at baseline was independently associated with
major bleeding risk in both rivaroxaban and warfarin arms (HR
1.88, 95% CI 1.59 to 2.22, p<0.0001).26 In 90,490 patients of the
Swedish AF cohort study without anticoagulant treatment, anaemia
was also a significant predictor of major bleeding (HR 1.40, 95%
CI 1.28 to 1.53).27 Anemia is also highly scored as an independent
risk factor for bleeding in several commonly used risk stratification
schemes validated to assess the risk of bleeding in patients with
AF before initiating oral anticoagulation therapy.23,28-30 (Figure 1)
Anemia appears to be an independent risk for bleeding regardless of
the duration of oral anticoagulation. In a prospective cohort study to
investigate the significance of anemia as a risk factor for bleeding in
patients with AF newly started compared to those on long term oral
anticoagulation, anemia remained a significant risk factor (HR 2.21,
95% CI 1.53 to 3.18, p<0.001) irrespective of the timing of initiation
of anticoagulation therapy.31 (Table 2)
Figure 1 Weighting of anemia versus other risk factors for bleeding in 4 commonly used bleeding risk scores[23,28-30
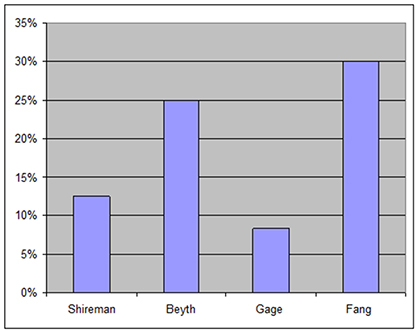
Table 2. Studies on anemia as a predictor of mortality or hospitalization in patients with AF
| Study |
Population |
Aim To |
Main findings |
| Puurunen, 2014 14 |
861 patients with AF undergoing PCI |
Analyse impact of anemia on outcome of patients with AF undergoing PCI |
Anemic patients had more thromboembolic events (29.1% vs 19.4%, p=0.002), stent thrombosis (3.9% vs 0.7%, p=0.002), minor (7.0% vs 3.3%, p=0.028) and total bleeding (25.2% vs 21.7%,
p=0.059) events |
| Westenbrink, 2015 20 |
18,113 patients with AF in RE-LY study |
Determine if anemia predicts thromboembolic or
bleeding events |
Anemia predicted stroke or systemic embolism (HR 1.41, 95% CI 1.12 to 1.78) and major bleeding (2.14, 1.87 to 2.46) |
| Westenbrink, 2014 21 |
18,201 patients with AF in ARISTOTLE study |
Test whether anemia predicts major bleeding |
Anemia predicted major bleeding (HR 1.92, 95% CI 1.62 to 2.28, p<0.0001) |
| Shireman, 2006 23 |
26,345 patients with AF on warfarin |
Develop a bleeding risk model
|
Anemia predicted major bleeding (HR 2.36, 95% CI 1.76 to 3.17) |
| Katoh H, 2014 25 |
184 patients with AF on dabigatran |
Determine risks of bleeding |
Anemia was a predictor of major bleeding (β=0.457, p=0.02) |
| Goodman 2014 26 |
14,264 patients with AF on warfarin or rivaroxaban |
Identify predictors of bleeding |
Anemia predicted major bleeding (HR 1.88, 95% CI 1.59 to 2.22, p<0.0001) |
| Friberg, 2012 27 |
90,490 patients with AF |
Investigate risks for bleeding
|
Anemia predicted major bleeding (HR 1.40, 95% CI 1.28 to 1.53) |
| Beyth, 1998 28 |
264 patients with AF on warfarin |
Evaluate outpatient bleeding risk index |
Anemia or other morbidity increased annual probabilty of bleeding from 11% to 44% |
| Gage, 2006 29 |
3791 patients with AF |
Find a bleeding risk scheme |
Anemia was validated as a part of the bleeding risk scheme |
| Fang, 2011 30 |
9,186 patients with AF |
Develop a bleeding risk stratification score |
anemia was validated as part of the bleeding risk scheme (HR 3.27) |
PCI= Percutaneous coronary intervention, HR=Hazard ratio.
The coexistence of anemia and chronic conditions not only further
adds to the comorbidity burden but it appears to be a detrimental
factor in worsening the outcomes.7,8 AF is not an exemption to
this observation. In AF population anemia clearly predicts adverse
outcomes including increased mortality, bleeding, thromboembolic
events and hospitalization. (Figure 2)
Figure 2
Mechanism of adverse outcomes
Anemia may increase mortality through increasing the risk of
coronary ischemic events. This may be due to the fact that anemia
may predispose to left ventricular hypertrophy and subsequently to
heart failure. Anemia is associated with cardiovascular compensatory
changes including high cardiac output, low systemic vascular resistance
and sodium and water retention increasing the cardiac workload.32
In patients with established atherosclerosis, anemia appears to be a
direct risk factor for myocardial ischemia and increased mortality.33 In a meta-analysis of 27 studies, anemia was associated with increased
mortality risk in patients with acute coronary syndrome.34 The
increased risk of bleeding induced by anemia may be explained by the
fact that in the normal conditions, with normal red blood cell count,
the flow and number of erythrocytes force the platelets centrifugally
towards the endothelial lining. This facilitates the contact of
the platelets to the vessel wall. Therefore, platelet adhesion and
aggregation occurs to reduce any bleeding when the vascular integrity
is disrupted by injury. In patients with anemia and reduced red blood
cell count this relationship is compromised with more luminally
rather than marginally placed platelets impairing the process of
platelet aggregation and adhesion increasing the risk of bleeding.35
Anemia also decreases the amount of adenosine diphosphate that
is available to contribute to collagen induced platelet aggregation
at the site of injury.36 The thromboembolic events precipitated by
anemia may be due to the fact that anemia may aggravate myocardial
ischaemia and unveil significant coronary obstruction in patients with
established atherosclerosis. The hemodynamic changes associated
with anemia such as increased heart rate and cardiac output lead
to myocardial hypertrophy increasing myocardial oxygen demands
and exaggerating the imbalance between myocardial oxygen demand
and supply.37 The duality of anemia to predict both bleeding and
thromboembolic events is not unusual as it is shared by the other risk
factors for ischemic stroke such as age or hypertension. Increased
hospitalization risk is likely to be due to the increased adverse
outcomes induced by anemia as stated above.
Implications for clinical practice
The relationship of anemia with adverse outcomes could be due
to the possibility that anemia acts as a mediator of adverse outcomes
and therefore correction of anemia may improve outcomes. The
other possibility is that anemia may merely act as a marker for
persons with worse prognosis related to their underlying complex
condition and comorbidity burden. However, in the Randomized
Etanercept North American Strategy to Study Antagonism of
Cytokines (RENAISSANCE) trial, correction of anemia improved
the outcome. For each one g/dL increase in the hemoglobin
concentration there was an improvement in the left ventricular
hypertrophy with a 4.1 g/m2 decrease in left ventricular muscle mass
and a 15.8% reduction in mortality risk after 24 weeks of follow up.38
Anemia appears to identify patients with AF who are at increased
risk for thromboembolic events who could benefit most from
oral anticoagulation therapy and who are also at risk for bleeding
complications. These findings suggest that close monitoring of oral
anticoagulation is important in patients with combined AF and
anemia. Anemia enhances the performance of the bleeding risk
scales and is already included as an independent predictor in four
of them. However, anemia may not enhance the performance of
the thromboembolic risk scales such as CHA2DS2-VASc as older
people (≥75 years) are likely to benefit from oral anticoagulation
therapy regardless of their risk stratification.39
Physicians may under estimate the magnitude of the bleeding risk
of anemia in patients with AF. In a study to describe physicians’
assessment of patient’s risk of bleeding using data from national
clinical registry of AF, anemia was the most significantly associated
with physician-assigned bleeding risk being lower than empirically
calculated bleeding risk (adjusted estimate, 1.36, 95% CI, 1.30
to 1.42).40 The bleeding risk predicted by anemia, especially
gastrointestinal bleeding, could be limited by the inability to account for the effects of antiplatelets or nonsteroidal anti-inflammatory
drugs used over the counter. Another factor is whether the use of
oral anticoagulation may have a confounding effect on calculating
the bleeding risk. However, in the Loire valley AF project, anemia
was an independent risk factor for bleeding in 7156 patients with
AF whether on vitamin K antagonist or not (HR 2.49, 95% CI 1.27
to 4.88).41 Anemia therefore appears to be a modifiable risk factor,
which suggests that prevention or treatment of anemia could improve
the prognosis in patients with AF.






