Combined Diagnostic Yield of Tilt Table Test And Implantable Loop Recorder to Identify Patients Affected by Severe Clinical Presentation of Neurally-Mediated Reflex Syncope who Could Respond to Cardiac Pacing
Tomaino M1, Unterhuber M1, Sgobino P2, Pescoller F1, Manfrin M1, Rauhe W1
1Department of Cardiology,Central Hospital of Bolzano, Italy.2Emergency Room, Central Hospital of Bolzano, Italy.
In this study we wanted to verify the diagnostic value of tilt table test (TTT) to predict the efficacy of cardiac pacing (PM) for preventing recurrences of neurally mediated reflex syncope (NMS) in patients with cardioinhibitory activity (CI) documented by implantable loop recorder (ILR).
Among patients selected by ILR in the context of severe clinical presentation of NMS, we analysed those who underwent PM implantation. In this observational and retrospective study we wanted to verify the results of TTT in the groups of treated patients with and without recurrences.
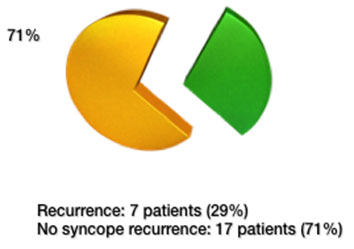
We analysed 24 patients treated using a PM (10 male and 14 female, mean age 70 years). During an average follow-up period of 35 months the recurrence of syncope occurred in 7 patients (29%). 17 patients (71%) had not recurrences. TTT was negative in 15 patients out of 17 without recurrences (88%). Among the 7 patients with recurrences TTT was positive in 4 patients (57%).
In conclusion, in this selected group of patients, a positive response to TTT is more likely correlated with a higher frequency of recurrences of syncope, while a negative response seems to predict the success of the pacing therapy. Consequently, PM could be insufficient to prevent the recurrences in the group of patients with positive TTT.
Key Words : Syncope, Tilt Test, Loop Recorder, Pacemaker.
Correspondence to: M. Tomaino,
Department of Cardiology,
Central Hospital of Bolzano, 39100 Bolzano, Italy.
The efficacy of cardiac pacing for prevention of syncopal recurrences in patients with neurally mediated syncope was considerable controversial. It was questioned approximately 15 years ago: two important randomized, multicenter, open label studies ( SYDIT1 and VASIS2 ) showed results in favour of pacing; but in the same period other two randomized, multicenter, double-blind studies ( VPS-2,3 SYNPACE4) failed to demonstrate the superiority of cardiac pacing to over placebo.
ISSUE-2 Trial5 changed the medical history in the context of severe clinical presentation of reflex syncope. ISSUE-2 Trial showed the capacity of ILR to guide the specific therapy and confirmed that there is not always a clear correlation between the results of TTT and the mechanism documented by ILR at the time of the syncope.
Three years ago, the ISSUE-3 Trial6 (a multicenter, double blind Trial) showed that pacing is effective in reducing recurrence of syncope in patients >40 years with severe asystolic NMS documented by ILR. There was 32% absolute risk reduction and 57% relative risk reduction, with evidence of a clear, statistical difference between the two groups: Pm on and Pm off arm.
At the moment we can affirm that, according to the ESC guide-lines,7 the pacemaker plays a role in the group of patients with frequent and invalidating recurrences of reflex syncope, selected by Implantable Loop Recorder after evidence of a documented cardioinhibitory activity, in class 2a.
Despite the efficacy of PM the ISSUE-3 Trial showed that in patients selected according to the ESC guide-lines, there is a good number of patients (25%) with recurrences during the follow-up period of 2 years.
Current knowledge about efficacy of pacing in reflex syncope is still characterized by needing further study; first of all whether in selecting patients Tilt Test-specific orthostatic stress is sufficient in identifying ideal candidates to cardiac pacing. This probably explains why the ESC Task Force for cardiac pacing is considering further research extremely important and very likely to impact future recommendations.
Among our patients who underwent a PM implantation, after a careful clinical evaluation and a diagnostic iter guided by ILR, we wanted to verify as to whether Tilt Table Test (performed in all patients during the initial evaluation) could help us to identify better responder PM patients.
The selection of patients was made according to the ISSUE-3 criteria: certain or suspected reflex syncope (except of “Carotid Sinus Syndrom” because this is an already axcepted indication for cardiac pacing), age more than 40 years, all patients had to have a severe clinical presentation to warrant a specific therapy and justify an invasive treatement like a PM implantation. The severity of the clinical presentation was based on the definition of high frequency or risk provided by guide lines: invalidated quality of life, unpredictable syncope, syncope exposing patients to risk of trauma, occurence of syncope during “high risk activity”.
The exclusion of patients involved cardiac abnormalities which suggested cardiac syncope, symptomatic orthostatic hypotension, non-syncopal loss of consciousness.
During the initial evaluation in all patient a TTT was performed according to the Italian protocol.8 It consisted in a 60-70 grades passive tilt for a duration of 20 minutes or until the occurrence of syncope; if the passive tilt phase did not induce syncope, 0,4 mg oral nitroglycerine spray was administered to the patients while the table was maintained in the same position; the test was continued for 15 minutes after pharmacological challenge. TTT positive responses were classified according to the New Vasis classification9 in asystolic or vasis 2B form (those with an asystole > 3 s) or mixed or vasodepressor forms (all the other forms without asystole).
After a careful initial evaluation and execution of TTT, all these patients followed a diagnostic iter guided by ILR and were followed till the first documented syncopal recurrence or an occurrence of a diagnostic arrhythmic event. Events were classified according to the ISSUE classification10 as: type 1 (asystole < 3 s), type 2 (bradycardia), type 3 (slight o no rhythm variations) and type 4 (tachycardia).
According to the ISSUE-3 Trial we implanted a dual chamber pacemaker with a specific algorithm for reflex syncope, the rate drop response (RDR), in patients with a documented asystole > 3 seconds and concomitant syncope or asystole > 6 seconds irrespective of the recurrence of syncope.
In this observational and retrospective study we wanted to observe the results of TTT in the two groups of treated patients: the group with recurrences and the one without recurrences.
We treated 24 patients (10 male and 14 female, age of 70+12 years) implanting a dual chamber PM with RDR algorithm in the period between 2008 and 2012.
All patients had not a significant structural heart disease, had a presentation of likely reflex syncope, with a burden of 4+2 episodes in the index year. 10 patients had no previous medical treatment. Because of hypertension 6 patients used 1 treatment (Ca-antagonist), 8 patients received two treatments (5 patients Ca-antagonist and Ace-Inhibitor, 3 patients furosemide and Ace-Inhibitor).
During an average follow-up period of 35 months the recurrence of syncope occurred in 7 patients (29%). 17 patients (71%) had not recurrences during the follow-up (Figure 1).
Figure 1. Recurrences in patients treated with PM
The mean time to first syncope recurrence was 7 months ±7 (95% CI).
TTT was positive in 4 patients out of seven with recurrences (in two cases documented CI): 57%.
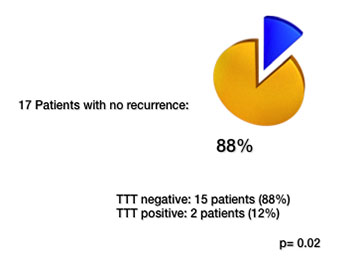
Among the 17 patients without recurrences TTT was positive only in 2 patients (12%), 15 patients had a negative TTT (88%), p= 0.02 (Figure 2).
Figure 2. TTT results in patients with recurrences
Considering that we are talking about well selected patients through a careful clinical evaluation, without structural heart disease and no rhythm disturbances, the common diagnostic pathway is overthrown by a small group of patients which presents with likely atypical reflex syncope.
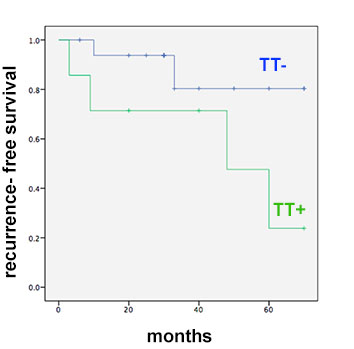
Figure 3. Recurrence-free survival of patients treated with PM and negative TTT
The ours is only a small experience, which is confirmed by an important subanalysis of the ISSUE-3 Trial.11 This substudy demonstrated that the benefit of pacemaker therapy in patients with presumed neurally-mediated syncope and documented asystole is greater when tilt test is negative. 52 Patients (26 TTT+, 26 TTT-) with asystolic ILR were treated with a PM: the recurrence of syncope occurred in 8 (31%) with TT+ and 1 (4%) with TT- patients. The unexpected and important conclusions of this subanalysis were that pacing is effective in NMS with asystole by ILR and negative TTT; there is no evidence of efficacy in positive TTT; although a positive asystolic TTT response predicts a clinical asystolic NMS, the pacing benefit is similar to that of positive non-aystolic TTT response.
Considering all that we are talking about results which could change the previous knowledge related to the historical role of TTT; in the past we implanted a PM after evidence of a significant asystolic event during the TTT, at the moment the discussion concerns the fact that just patients with positive TTT (irrespective of cardioinhibitory or vasodepressor form) are those who respond less to a PM therapy.
In perspective the somewhat surprising results of these evidences can be interpreted differently. Results are of help in selecting the best candidates to cardiac pacing. From one hand, cardiac pacing is very effective in NMS patients who have the documentation of an asystolic event and a negative TTT. In the ISSUE-3 substudy the observed 5% recurrence rate with pacing at 21 months is similar to that observed in the DANPACE Trial, in patients paced for cardiac intrinsic bradycardia.12 thus, pacemaker therapy could be offered to these patients with the same confidence than that used for indications in patients with sick sinus syndrome or AV block. These patients could be reassured that, after pacemaker implantation, they will likely be free of recurrence of syncope. On the other hand, caution should be exercised before offering such therapy to patients with a positive TTT even if they have had an asystolic response during TTT and the documentation of an asystole during spontaneous event by ILR. Even if some benefit could be still possible in terms of reduced burden of syncope, the patients should be informed that they will likely have some recurrence of syncope despite cardiac pacing. This is the reason why this group of patients could take advantage from a supplementary therapy like the “isometric counterpressure manouvres” (ICM), in a sort of hybrid therapy: PM plus ICM.13
Recently the SUP-2 Study14,15 has been completed; it is a multicenter, prospective, observational study which wanted to verify the utility of a standardized algorithm for cardiac pacing in older patients affected by severe unpredictable reflex syncope. The Syncope Unit Project 2 (SUP 2) showed the benefit of cardiac pacing at 3 years in patients selected according to the ESC-guide lines: carotid sinus massage (CSM) , followed by Tilting Table Test (TTT) if CSM was negative, followed by implantation of an Implantable Loop Recorder (ILR), if TTT was negative; those who had an asystolic response to one of these tests received a dual-chamber pacemaker. The 3-years recurrence of syncope was 20% and was significantly lower than the group of patients who did not receive the pacemaker and were observed by ILR. The 3-year recurrence was not different among the subgroups (CSM, TTT and ILR) used to select patients to undergo pacemaker implantation, whereas it was lower in patients with negative TTT than patients with positive TTT.
Considering the recent scientific literature concerning the use of a pacemaker as first line treatment in the context of neurally mediated syncope we can affirm that:
1. the most important point is the accuracy in the selection of patients after a careful initial evaluation
2. ISSUE-3 (double blind study) demonstrated the efficacy of pacemaker in this group of patients selected by ILR, but first of all in patients who had a negative TTT (subanalysis)
3. SUP-2 (observational study) showed that TTT is also efficient to identify patients who could respond to the cardiac pacing but, once more, PM seems to be mostly effective in patients with negative TTT
4. in these studies we have used in most cases a dual chamber pacemaker with a specific algorithm, the rate drop response (RDR). It is necessary to remember that we do not have studies of comparison between a pacemaker with and without the RDR, as there are no studies of comparison involving devices with different algorithms.
At the moment there are two points to investigate further: the capacity of TTT to identify patients to undergo a pacemaker and the opportunity to verify other pacing algorithms in the context of a selected group of patients affected by NMS. Further important information will be given from the BIOsync Trial: an international, randomized, double-blind parallel trial, which aims to verify the benefit of dual-chamber pacing with closed loop stimulation (CLS) in tilt-induced (tilt positive) cardioinhibitory reflex syncope.16,17,18,19
These results show that a positive TTT seems to be more likely
correlated with a higher frequency of recurrences of syncope in
patients treated using a PM, while a negative response seems to
predict the success of the pacing therapy.
The rationale could be that TTT is able to highlight the importance
of a concomitant hypotensive reflex response or that the orthostatic
stress (for example during prolonged standing) as trigger of reflex
syncope (investigated by TTT) produces an important reduction
in the central venous volume, as consequence the compensative
chronotropic pacing in an empty heart is not able to prevent the
syncope.
Anyhow PM could be insufficient in a group of patients with
positive TT response.






