Symptoms In Atrial Fibrillation: A Contemporary Review And Future Directions
Steven T. Heidt, BS1, Anna Kratz, PhD2, Kayvan Najarian, PhD3, Afton L. Hassett, PsyD4, Hakan Oral, MD1, Richard Gonzalez, PhD5, Brahmajee K. Nallamothu, MD, MPH1, Daniel Clauw, MD4, Hamid Ghanbari, MD, MPH1
1University of Michigan– Department of Cardiovascular Medicine.2University of Michigan – Department of Physical Medicine and Rehabilitation.3University of Michigan – Department of Computational Medicine and Bioinformatics.4University of Michigan – Department of Anesthesiology.5University of Michigan – Department of Psychology.
Atrial fibrillation (AF) is the most prevalent arrhythmia leading to hospital admissions in the United States. The majority of patients with AF report symptoms associated with this condition that can lead to a decrease in health related quality of life (HRQOL) and functional status. Therefore, along with reducing the risk of stroke and mortality, improvements in such symptoms are important therapeutic goals in the management of patients with AF. Our current understanding of how AF and symptoms are linked is hampered by the dominant assessment paradigm, where symptoms thought to be associated with AF are measured at a single point in time (frequently at a clinic visit). Unfortunately, this “static” snapshot does not capture the variability of symptoms and heart rhythm within a person over time and does not shed light on how symptoms are related to heart rhythm. This focused review summarizes current methods for assessing symptoms including generic and AF-specific HRQOL and functional status tools. It also describes gaps in the current assessment paradigm and where future research using mobile applications and digital technology might be able to assist with patient care.
Key Words : Atrial Fibrillation, Health Related Quality Of Life, Affect, Functional Status.
Correspondence to: Steven T. Heidt, University of Michigan - Department of Cardiovascular Medicine 24 Frank Lloyd Wright Drive Lobby A, Suite 3700, Room 3201 Ann Arbor, MI 48106
Atrial fibrillation (AF) is the most prevalent arrhythmia leading to hospital admissions in the United States.1 Its incidence is associated with an increase in the risk of stroke, congestive heart failure, and overall mortality.2-4 The national incremental cost of AF to the health care system has been estimated from $6.0 to $26.0 billion.5 Moreover, the number of patients diagnosed with AF is expected to increase to more than 15 million by 2050.6
The onset of AF may or may not be signaled by the onset of symptoms. The majority of patients with AF report symptoms associated with the condition sometime throughout the disease process; however, a sizable proportion of patients (12-42.5%) remain completely asymptomatic during each presentation of AF.7-9 The most common symptoms reported are dyspnea, chest pain, dizziness, fatigue, and palpitations. Paradoxically, recent studies using implantable cardiac monitors and arrhythmia-detecting pacemakers have revealed that patients in sinus rhythm also report symptoms of AF. These symptoms, whether reported during a period of AF or not, are related to lower functional status and health related quality of life (HRQOL) in the majority of patients with AF.10-12 In turn, low functional status and HRQOL are strong predictors of all-cause and cardiovascular hospitalizations in patients with AF.13 Furthermore, symptoms contribute to the increase in invasive cardiovascular procedures, medication use, and health care resources utilization. Therefore, improvement of symptoms is an important therapeutic goal in itself and is also related to lower risk of stroke and mortality in patients with AF.14
There are several treatment strategies that target improvement of AF symptoms. The goals of these therapies are to either restore normal sinus rhythm (NSR) or achieve heart rate control with medications and invasive cardiac procedures. Several studies have evaluated the effect of restoring NSR or achieving adequate heart rate control on symptoms and generally have shown that improving rhythm does not improve symptoms.11,15-19 Paradoxically, even without evidence for improvement of symptoms when rhythm is restored in patients with AF, a significant number of patients undergo pharmacological and interventional therapies to restore sinus rhythm in an effort to improve symptoms.20 Further, there is little empirical data to guide clinicians in regard to which symptoms are directly related to AF and should be a focus of the management of AF, versus other symptoms that might be generally unrelated to AF. Our understanding of how AF and symptoms are linked is hampered by the dominant assessment paradigm, where symptoms thought to be associated with AF – dyspnea, chest pain, palpitations, dizziness, fatigue – are measured at a single point in time (frequently at a clinic visit). Unfortunately, this “static snapshot” does not capture the daily variability of symptoms and heart rhythm and does not shed light on how symptoms are related to heart rhythm. AF can be a highly dynamic disease and a resting heart rhythm and rate during a clinical visit does not provide information about the patient’s heart rate, AF burden, and symptoms during activities of daily living. Also, this static snapshot ignores significant features within the ECG recording (especially those that serve as surrogates for autonomic function) that may better predict symptoms in AF.
Figure 1. Conceptual Model of Relationship between Heart Rhythm, Symptoms, Affect, and Functional Status
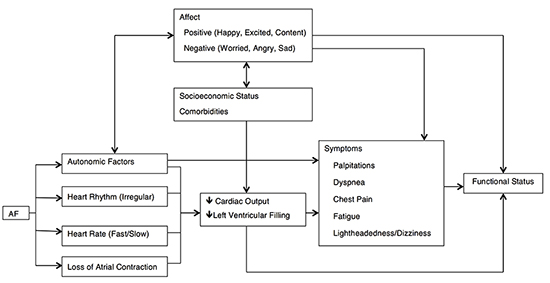
Functional status of AF patients is influenced by a variety of factors including disease processes, symptom severity and frequency, and psychological affect. These elements may contribute to functional status individually or in combination with other factors
This focused review will summarize our current knowledge of symptoms, symptom measurement, HRQOL, and functional status in AF and guide future research efforts aimed at improving the assessment, understanding, and treatment of symptoms in patients with AF.
Articles selected for this review were chosen based on the authors’ knowledge of the AF literature and a structured search using the Medline®/PubMed® database (http://www.ncbi.nlm.nih.gov/pubmed) and Google Scholar (https://scholar.google.com). Our review was deemed complete in May 2016, and encompassed literature regarding AF published between 1964 and 2016. Search terms used alone or in combination included “atrial fibrillation,” “quality of life,” “assessment,” “arrhythmia,” “ECG,” “demographics,” “psychological,” “perception,” “somatization,” “monitor,” “Holter,” “event,” “implantable loop,” “ambulatory cardiac telemetry,” “pacemaker,” and “implantable defibrillator.” All abstracts were considered, and articles of interest were reviewed in full. Reference sections were explored to identify cited articles of interest. Google Scholar’s “cited by” tool was beneficial in identifying follow-up articles to novel investigations. No preference was given to a specific study type: clinical trials, observational studies, cross-sectional investigations, and other reports of other research efforts were equally considered. This report is intended to be informative rather than exhaustive, and presents major findings related to HRQOL assessment in AF and factors that may influence perception of AF related symptoms.
Conceptual Model Of Symptoms In Patients With AF
Symptoms related to AF are likely to be multifactorial as a result of both direct and indirect effects of the arrhythmia, as well as interactive effects with affect (aspects of which are independent from arrhythmia). We have adopted a recent conceptual model of symptoms in AF that reflects this complex relationship and addresses the interaction between physiological factors, affect, symptoms, and functional status (Figure 1).21 The model identifies physiological manifestations of AF and affect as separate but related entities, combining to influence symptom perception and ultimately functional status. This reciprocal relationship has led to increased investigation of both psychological and physiological factors contributing to the AF experience in recent years.
There is a paucity of data on the physiological mechanisms by which AF causes some symptoms.22 The postulated mechanisms for the common symptoms associated with AF include impaired myocardial perfusion, alterations in sympathetic nervous system function, impaired ventricular diastolic filling, and decreased cardiac output.23-26 Remarkably, despite the lack of evidence for improvement of symptoms after treatment of patients with AF, 11,15-19 a significant number of patients undergo pharmacological and interventional therapies to restore sinus rhythm in an effort to improve symptoms.20 One potential reason for the lack of concordance between clinical practice and research findings is that clinical trials have been limited by the static assessments of heart rhythm and symptoms obtained during a clinical encounter.
Asymptomatic AF: Accounting For Symptom Dissociation
Historically, investigations measuring the success rates of AF-targeting operations such as ablation, cardioversion, and the Cox-Maze procedure were based on freedom from symptoms of AF during the follow-up period. Others used brief clinic electrocardiograms or limited Holter monitor recordings to get a clearer picture of post-procedural heart rhythm. Unfortunately, many of these studies failed to properly account for asymptomatic recurrences of AF, which still create the opportunity for deep vein thrombosis, pulmonary embolism, and stroke.27 Studies using implantable cardiac monitoring systems have shed light on the true prevalence of AF, and have found that AF recurs far more often than symptom presentation may suggest. In one of the first studies to measure asymptomatic disease, Page et al discovered that in patients with symptomatic paroxysmal AF followed for 12 months, asymptomatic atrial tachyarrhythmia occurred 12 times more often that symptomatic tachyarrhythmia.28 Later studies expanded upon this finding, estimating that even in patients with some symptomatic disease, asymptomatic AF was far more prevalent, accounting for 54-94% of all AF arrhythmias.8,29-31 Asymptomatic AF is especially prevalent in patients who have undergone some form of interventional procedure to treat AF. Verma and colleagues found that the ratio of asymptomatic to symptomatic events increased from 1.1 to 3.7 following catheter ablation.7
The use of implantable cardiac monitoring devices has done more than reveal the prevalence of asymptomatic AF: it has allowed us to search for correlations between heart rhythm and AF symptoms. Two separate studies attempting to determine the predictive value of AF symptoms to heart rhythm offered disappointing results, estimating the positive predictive value at only 17-21%.8,31 On the other hand, these studies have allowed us to learn that a large proportion of patients report AF symptoms when not in a device-confirmed episode of AF. Results from varied paroxysmal AF populations found that of all symptom reports, 45-79% were actually these “false positives.”8,29,31 Precipitating factors of non-AF arrhythmic symptoms have yet to be elucidated. Regardless of actual heart rhythm during symptom presentation, symptom measurement and management remain key in the treatment of AF.
Measuring Functional Status And HRQOL In AF Patients
Of all AF patients, about 15% to 20% report a decreased exercise tolerance associated with their condition.32 It is therefore of clinical interest to measure functional status in patients with AF both as a means of measuring symptom burden and as an outcome measure for therapeutic interventions.21 The most commonly used subjective measures of functional status in AF are the New York Heart Association (NYHA) classification, the Canadian Cardiovascular Society classification, the Duke Activity Scale Index, and the Goldman Specific Activity Scale. More objective measures include the 6-minute walk test or an exercise stress test.33 However, these published measures have not been specifically designed or validated in patients with AF. Further, they are collected at a single point in time without considering the variability in heart rhythm, symptoms, affect and functional status.
There are several different global measures used for evaluation of HRQOL in patients with AF, although the EuroQol 5-Dimension (EQ-5D) Assessment and the Short-Form Health Survey (SF-36) are the most frequently administered.34,35 An in-depth analysis of these generic HRQOL instruments is presented in Table 1. The EQ-5D assesses five specific domains regarding health status: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.34 In total, the assessment contains six questions; one for each health domain and the Visual Analogue Scale, which asks the patient to rate their perceived level of health from “worst imaginable” to “best imaginable” on a scale of zero to one hundred.34 Responders select from one of three values on the health-domain specific questions: “no problem,” “some or moderate problems,” or “extreme problems.” Based on these answers, one of 245 disease states can be assigned, which include “unconscious,” “dead,” and “worse than dead.”34 Using these disease state classifications, patients can be assigned “Quality-Adjusted Life Years” for cost and health utility analyses.36 Later interpretations of the EQ-5D (EQ-5D-5L) have increased the number of responses on the health-domain questions to five, thereby improving granularity.
Figure 2. miAfib Mobile Application
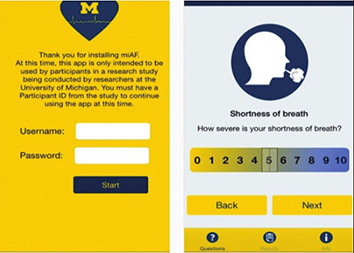
Representation of the miAfib mobile application interface used by study participants in a small institutional trial. The mobile application allows study participants to record symptoms and emotional affect at any time; when paired with ambulatory ECG readings, investigators may begin to associate alterations in heart rhythm with symptoms and changes in affect.
The SF-36 questionnaire is likely the most widely used tool to assess HRQOL in the general population. It was found to be valid, reliable, and acceptable for public use in 1992, and has since been used in general patient practice and numerous clinical trials, including those for AF.35 The SF-36 assesses eight specific disease domains, including physical functioning, social functioning, role limitations (both physical and emotional), mental health, vitality, pain, and general health perception. The questionnaire also queries health change, which is not scored and serves to quantify changes in health status over the course of a particular treatment. Disease domains are stratified into physical or mental component scores (PCS/MCS), which can be used to assess overall physical or mental health. On average, the SF-36 takes patients about five minutes to complete, and the non-monotonous make-up of the questions may decrease participant fatigue and improve completion rates. In the years since its validation, three shorter interpretations of the SF-36 have been developed and validated, the SF-12, the SF-8, and the SF-6.37,38 These briefer forms take less time to complete, and like the SF-36, they can be completed as part of a routine clinic visit. Additional versions of the SF-36 and the SF-12 have been validated in recent years, showing improvements in general wording and precision in the role-functioning scales (both emotional and physical).39,40 These new forms are now recommended for general use in most situations.
Figure 3. Relationship between Heart Rhythm, Affect, and Palpitations
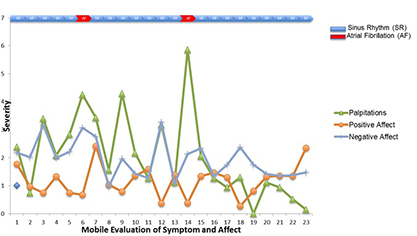
Representation of results obtained from the miAfib mobile application, documenting rhythm status, presence of palpitations, and emotional affect. Palpitations were not always associated with presence of AF, and emotional state varied throughout the observation period.
Generic HRQOL assessments like the SF-36 and the EQ-5D are extremely effective in determining general levels of HRQOL in a variety of patient populations. Although brief and suited for use in clinical situations, they lack the specificity needed to distinguish between different disease states. Because patients with AF are likely to have a variety of other cardiovascular conditions, such as coronary artery disease or heart failure, determining the true effect of AF on HRQOL is challenging when using generic measures. In addition, these instruments have been shown to improperly account for HRQOL in women, the elderly, and the unemployed, among other groups.35 For optimal determination of HRQOL in the AF population, it is recommended that generic measures be used alongside AF-specific measures.
AF-Specific HRQOL Instruments
In order to meet the need for AF-specific instruments to assess HRQOL, AF-specific measurements have come into widespread use in the past few years. Although AF-specific instruments are not as generalizable to the general population or as extensively validated, they offer a clearer picture of what AF patients experience on a regular basis. AF-specific measurements generally assess symptom severity, AF burden, and impact of treatments, among other characteristics. Most of these instruments have been validated against general HRQOL assessments, and are often used alongside general measures in clinical trials to obtain a full picture of HRQOL. The most commonly used instruments are presented in Table 2.41-45
The Atrial Fibrillation Effect on QualiTy-of-Life (AFEQT) Questionnaire has become the most commonly used AF-specific HRQOL measure in recent years.42 It has been developed and validated for measurement of symptoms, daily activities, treatment concern, and treatment satisfaction. Patients are categorized by symptom severity: asymptomatic, mild, moderate, or severe. It is accurate in discriminating between AF patient groups (i.e. those with paroxysmal or persistent AF) and is sensitive to changes in AF-related HRQOL over time. In the validation study, patients who were treated with radiofrequency ablation showed significant HRQOL improvements over those treated with pharmacological treatment and those who received no AF treatment.42 This finding indicates that AFEQT is beneficial in assessing treatment-specific changes to HRQOL, which is of particular importance for investigators selecting an AF-specific instrument for clinical trial use.
AF-Specific Classification Tools and Symptom Scales
As opposed to generic or disease specific HRQOL measures, classification tools and symptom scales offer a chance to quantify the impact of AF on a patient’s health condition without considering overall HRQOL. These instruments are often used in clinical practice, when there is not enough time in a regular patient interaction to complete longer HRQOL assessments. The classification tools described in this section include the European Heart Rhythm Association (EHRA) Classification and the Canadian Cardiovascular Society Severity in Atrial Fibrillation (CCS-SAF) Scale.46-48 Similar to the NYHA scale in patients with congestive heart failure, these classification systems allow a provider to quickly designate AF patients into specific classes, which can then be used as a guide for future treatment options.49 Patient-completed symptom scales such as the University of Toronto Atrial Fibrillation Symptom Severity (AFSS) tool and the Symptom Checklist (SCL) have been used for decades to immediately assess the frequency, duration, and severity of AF-related symptoms.50,51 They are often paired with generic HRQOL tools to create a broader picture of the overall effects of AF. These classification systems and scales, along with pertinent characteristics and advantages, are presented in Table 3.46-48,50-52
The EHRA classification is a clinician-completed tool and assigns patients with AF into one of four symptom distinct categories: 1-no symptoms; 2-mild symptoms which do not affect daily activities; 3-moderate symptoms which affect daily activities; and 4-severe symptoms which cause a discontinuation of daily activities.47 The classification was validated in 2014, though a poor discriminatory ability between groups two and three prompted a reclassification of patients in group two: those whose symptoms were not considered “troublesome” are assigned to group 2A; those with troublesome symptoms are assigned to group 2B.46 This new classification system is known as the modified EHRA (mEHRA). Both tools are valid and reliable for differentiating between AF patients of varying symptom severity, but the mEHRA offers more granularity. The Canadian Cardiovascular Society Severity of Atrial Fibrillation (CCS-SAF) scale was created as a concise, symptom-based severity scale intended for routine clinical use in patients with AF.53 The CCS-SAF scale provides a potentially clinically useful scale for practitioners to assess patient status and to communicate the severity of the functional consequences of the patient’s symptoms from AF. It closely approximates patient-reported subjective measures of quality of life in AF and may be practical for clinical use.48 The SAF class, derived from CCS-SAF, is imperfectly correlated to generic QOL measures in the SF-36 and AFSS. This presumably occurs because the SAF class captures, by design, all components of the AF syndrome (including, for example, symptom severity during AF, adverse effects of treatment administered, and the physical and psychological consequences of the disease state), whereas the generic QOL measures capture only components of the AF “illness burden.”48 Though not as regularly utilized as the NYHA classifications, we anticipate that the EHRA, mEHRA, and CCS-SAF scales will become commonplace in clinical practice.
Patient completed symptom scales have been extensively used in clinical trials and in the validation of AF-specific HRQOL instruments. Although they are not descriptive enough to encompass all facets of HRQOL, these tools are helpful in determining the effect of pharmacological or interventional treatments on the symptoms of AF. The SCL encompasses frequency and severity of AF symptoms and has been shown to be beneficial in evaluating patients with atrial fibrillation and other types of tachyarrhythmia.51 The AFSS is a 14-item assessment that also investigates symptom frequency, duration, and severity, but is limited to atrial fibrillation patients only.50 The AFS/B is a relatively new symptom scale that assesses both AF severity and burden; as compared to other tools, both the patient and provider assess symptoms.52 Not surprisingly, the correlation of patient-reported symptoms to HRQOL was stronger than that of the physician’s, underscoring the need for patient-completed outcome measures.
While the breadth of available classification systems and symptom scales allows the use of specific tools for distinct patient populations, the lack of consensus on one specific tool is apparent. It is imperative that we continue to further validate the available tools in different populations and develop new measures for assessment of patients with AF should the need arise.
Demographics Influencing Symptom Assessment In AF
Large population-based assessments of HRQOL outside of the AF population tell us that older patients often report lower levels of HRQOL when compared with their younger counterparts.54,55 This finding can be explained by the fact that older patients are more likely to have additional underlying chronic diseases, which hinder them more than younger patients with fewer diagnoses. Along these lines, many studies have found that older age negatively affected HRQOL in those with permanent AF.19,50,56 Some other assessments of HRQOL show an interesting discordance with this trend: although older AF patients reported lower levels of physical functioning, both younger and older patients recorded similar mental functioning levels and overall HRQOL scores. Reynolds et al found that elderly AF patients reported decreased levels of physical functioning, but ranked higher on mental HRQOL scores than their younger counterparts.57 This finding is consistent with well-established findings in the general population that levels of negative affect tend to decrease, while levels of positive affect tend to increase with age. This could also stem from younger patients perceiving the diagnosis of AF to be more intrusive to their execution of daily activities.58-60 In addition, younger patients reported higher levels of symptom severity, possibly stemming from anxiety over having a new diagnosis.61 Data from the ORBIT-AF trial regarding demographic differences in AF presentation and HRQOL showed that patients with a new AF diagnosis recorded lower HRQOL scores on the AFEQT.9 Older patients may place less emphasis on their symptoms of AF, or attribute non-specific symptoms of chest pain or dyspnea to separate cardiac diagnoses, such as coronary artery disease or congestive heart failure, or even attribute such symptoms to growing older. One study of exercise tolerance in the elderly found that elderly AF patients had no depreciation of quality of life when compared with a separate control group of older patients, but this finding has been heavily refuted and can be attributed to a low participant number.17 Studies measuring the relationship between age and AF must take into account that while their participants may report lower levels of physical functioning, they may not perceive AF to have a great impact on overall HRQOL.
When validating the SF-36 instrument, the investigators found that females in the general population scored significantly lower than men in all aspects of the assessment, including physical, mental, and overall HRQOL.35 Numerous AF clinical trials, cross-sectional investigations, and prospective studies have found that women score lower than men on at least one aspect of a generic HRQOL assessment.9,19,50,57,62-64 It should be noted that even in some clinical trial control groups, healthy men report greater HRQOL than healthy women.62 Although there is debate over the exact cause of decreased scores on HRQOL assessments, increased symptom reporting among females may offer some clarification.65,66 Women often report greater AF severity, frequency, and burden than men on questionnaire measures.50,52,56,57 When evaluated with continuous ambulatory monitors or an event/loop recorder, women report more undocumented episodes of AF, meaning symptom reports do not correlate with time-stamped ECG recordings.67 A 2016 study of HRQOL in female AF patients showcased all of these findings, as women recorded fewer asymptomatic AF events, recorded an increased number of AF symptoms (even when not correlated with ECG-documented AF), and lower overall HRQOL as measured by the AFEQT.9
Table 1. Analysis of Generic HRQOL Instruments
| Generic HRQOL Instrument |
Number of Questions and Scoring Method |
HRQOL Domains Assessed |
Length of Recall Period |
Specific Advantages |
| EQ-5D34 |
- 6 total questions
- Patients are assigned one of 245 disease states based on responses |
- Mobility
- Self-care
- Usual Activities
- Pain/Discomfort
-Anxiety/Depression |
Present day |
- Extensive validation
- Widespread use in clinical situations
- Extremely brief
- Stratification by QALY |
| SF-3635 |
- 36 total questions
- Questions within each domain are scored on a 0-100 scale (Health Change is unscored)
-Physical (PCS) and Mental (MCS) Component subscores (0-100) may be calculated |
- Physical Functioning
- Social Functioning
- Role limitations (physical problems)
- Role limitations (emotional problems)
- Mental health
- Vitality
- Pain
- General Health Perception
- Health Change |
Up to four weeks |
- Extensive validation
- Widespread use in clinical situations
- Relatively brief
- PCS/MCS subscores |
*EQ-5D: EuroQol Five Dimension. SF-36: Medical Outcomes Survey Short Form 36. QALY: Quality-Adjusted Life Year
Increased symptom reports in women have been linked with depression, anxiety, and somatization tendencies, which may also explain decreases in mental well-being and overall HRQOL.63,68 Regardless of the underlying physiological or psychological mechanism, increases in AF symptom severity, frequency, or duration drive more women than men to seek medical treatment.13,63,67 Suttorp et al found that women had a higher rate of AF recurrence after pharmacological or interventional treatment; however, the investigators defined AF recurrence as any report of symptomatic AF, failing to account for asymptomatic AF.69 Knowing that women report symptoms more commonly than men, and that both groups report symptoms in normal sinus rhythm, it is unlikely that a significant difference in AF recurrence rate exists between these groups. Although most investigators are aware of the tendency for females to score lower on HRQOL measures and report more AF-related symptoms than men, some studies still fail to adjust for female sex in multivariate models, leading to potentially confounded results.
Association Between Affect and Symptoms
There is growing evidence that affect is associated with cardiovascular health.70 Negative emotional states have been associated with acute cardiac dysfunction, myocardial ischemia, and increased long term cardiovascular mortality.71 These negative emotional states and specifically anxiety and depression have also been linked to more severe symptoms in patients with AF.70,72-74 Anxiety in the AF population is fairly widespread, and may affect all types of patients. Studies examining the prevalence of anxiety in the AF population have found that while women report higher rates compared to men, the prevalence of anxiety is consistent across age groups.64,75,76 Increased symptom prevalence in women may cause greater feelings of anxiety, perhaps because of a belief that their disease is more serious as compared to the male population. Increased levels of anxiety often manifest as lower rankings of HRQOL and increased reports of symptom frequency and severity.64,77,78In a landmark study assessing the relationship between personality traits and lower levels of HRQOL, Ong et al. discussed the role of anxiety sensitivity, or the tendency to associate anxiety-related sensations as signifying immediate harm or catastrophe. The authors found that anxiety sensitivity was related to symptom preoccupation; furthermore, both anxiety sensitivity and symptom preoccupation led to decreased mental and physical HRQOL and increased symptom severity.79 Patients who are more sensitive to anxiety provoking events (such as symptoms of atrial fibrillation) may be more likely to worry about these symptoms, which manifests as decreased perception of HRQOL. Other investigators have shown that illness perception can fuel negative thoughts about AF and its symptoms, and attempts to educate patients about the true nature of AF may remedy erroneous and anxiety-provoking beliefs.80,81
The prevalence of depression among the AF population is similar to that of anxiety, with similar detrimental effects on HRQOL. Women are more likely to be affected than men, and rank lower on HRQOL scales as a result.64,82 Ong et al. cited depression as a mediating factor for decreased HRQOL in women, suggesting that because women are more commonly affected by depression, this tendency influences HRQOL scores.82 While depression may contribute to AF-related HRQOL in some women, additional underlying factors are likely to be present in others. Regardless of sex, patients with depression are more likely to be affected by symptoms.83 The presence of depression may perpetuate with an AF diagnosis: Dabrowski et al showed that AF patients with depression also had lower levels of activity and overall energy, negatively impacting HRQOL.84 AF patients who were unemployed also reported lower levels of HRQOL, which may be explained by the prevalence of depression among those without full-time jobs.64,85 Investigations measuring anxiety and depression at baseline and follow-up have found that AF treatments are generally ineffective at improving these psychological conditions, and recurrence rates of AF after cardioversion are higher in those with depression.61,64,86
Table 2. Analysis of AF-Specific HRQOL Instruments
| AF-Specific HRQOL Instrument |
Number of Questions/Scoring Method |
HRQOL Domains Assessed |
Length of Recall Period |
Validation Strategy |
Specific Advantages |
| AF-QoL41 |
-18 total questions
-0 to 100 scoring scale, 100 indicating best HRQOL
-Domain scores may be calculated |
-Physical Functioning
-Psychological Functioning
-Sexual Activity |
-One month |
-Validated against SF-36 |
-Good discriminatory power
-Sensitive to change for follow-up assessment
-Domain scoring for specific assessment |
| AFEQT42 |
-20 total questions
-0 to 100 scoring scale, 100 indicating no limitation or disability from AF.
-Domain scores may be calculated |
-Symptoms
-Daily Activities
-Treatment Concern
-Treatment Satisfaction |
-4 weeks |
-Validated against SF-36, EQ-5D, AFSS, and SCL |
-Good discriminatory power
-Sensitive to change for follow-up assessment
-Patient input via treatment concern and satisfaction domains
-Domain scoring for specific assessment |
| ASTA43 |
-9 total questions
-Patient scores are not coded to specific 0-100 scales.
-Higher scores indicate greater symptom burden or arrhythmia impact |
-Symptom Burden
-Arrhythmia Impact |
-3 month episode recall |
-Validated against SF-36 and SCL |
-Brief assessment
-May be used in patients with non-AF tachyarrhythmias |
| AFSympTM 44 |
-11 total questions
-Domain scores may be calculated |
-Heart Symptoms
-Tiredness
-Chest Discomfort |
-1 week |
-Validated against SF-36, AFSS, AFImpact |
-Developed for use across cultural contexts
-Valid for use in all AF patient groups (paroxysmal, persistent, and permanent)
-Electronic tool |
| AFQLQ45 |
-26 total questions
-Domain scores may be calculated |
-Variety and frequency of symptoms
-Severity of symptoms
-Limitations of daily and special activities and mental anxiety related to AF |
-Not available (written in Japanese) |
-Not available (written in Japanese) |
-Sensitive to change for follow-up assessment
-Previous clinical trial use
-Domain scoring for specific assessment |
*AF-QoL: Quality of Life Questionnaire for Patients with Atrial Fibrillation. AFEQT: Atrial Fibrillation Effect on QualiTy of Life Questionnaire. AFSS: Atrial Fibrillation Symptom Severity Scale. SCL: Symptom Checklist. ASTA: Arrhythmia-Specific Questionnaire in Tachycardia and Arrhythmia. AFQLQ: Atrial Fibrillation Quality of Life Questionnaire.
Compared to anxiety and depression, somatization has been less well examined as a potential contributor to HRQOL in the AF population. Defined as the tendency to experience non-specific, recurrent medical symptoms due to underlying psychological distress, somatization may be present in patients who report AF symptoms as especially frequent or particularly severe. AF studies assessing somatization most commonly use the Somatosensory Amplification Scale, a validated, brief tool that reliably identifies patients who amplify symptoms based on clinical or subclinical psychological conditions.87 Paquette et al determined that along with depression and anxiety, AF patients with high levels of somatization scored lower on the mental health subscale of the SF-36, reported decreased functional capacity, and experienced increased symptom frequency and severity when compared to those with low levels of somatization.63 An additional study found that even after adjusting for age, sex, and other demographic factors, somatizing patients still scored higher on the AFSS in terms of symptom severity.88 Assessment for somatization plays an important role in interventional studies that define an “AF recurrence” as the first time a subject experiences an AF symptom post-procedure. Aside from not accounting for asymptomatic AF, this definition may lead to an overestimation of AF recurrences in specific demographic groups. In order to provide a clearer characterization of the psychological makeup of patient populations under study, investigators should consider administering some form of somatosensory scale along with validated depression and anxiety measures.
Regardless of disease type, patients with higher educational levels have been shown to possess increased levels of health literacy, better equipping them to seek out, use, and understand health information.89,90 In the AF population, it is known that older patients, those with less formal education, and those with decreased health literacy all possess lower levels of disease-specific knowledge.91-93 Aside from the potential clinical implications associated with decreased AF knowledge, a lack of understanding of AF and its complications may impact symptom perception. To our knowledge, only one study has examined the impact of educational level on AF symptom perception. Goli et al. determined that in a prospective cohort of AF patients, those with low levels of educational achievement (less than a high school diploma) were more likely to report severe symptoms of AF.88 These patients may believe that their disease is more intrusive or potentially harmful than others who are more informed about the course of the non-lethal arrhythmia. Initial unadjusted analyses found that non-Caucasian race and unemployment also significantly influenced AF symptom severity though did not remain significant after adjustment for confounding variables including age and comorbid conditions.88 Investigations assessing HRQOL in the AF population must account for the influence of educational level on AF symptom perception. Clinical trials lacking a standardized educational session regarding the course and complications of AF may be introducing an additional confounding element into the analysis, allowing patients to draw their own conclusions about the prognosis of AF.
Influence Of Comorbid Conditions
The advent of disease specific tools has, to an extent, allowed investigators to analyze the effects of treatments or interventional techniques on the patient experience of AF. AF patients are often afflicted with multiple cardiovascular conditions, especially in the older population and, on general HRQOL assessments, patients with cardiovascular disease score lower than healthy controls; it follows that those with multiple diagnoses will report lower HRQOL than those with only a single diagnosis.10,94 Yet, studies assessing the impact of comorbid conditions on HRQOL in patients with AF offer mixed results. The FRACTAL investigators found that AF patients with additional cardiovascular conditions recorded lower HRQOL as compared to those with AF alone.57 An additional study found that AF patients with severe underlying cardiovascular disease reported lower HRQOL as compared to patients with more manageable conditions.19 Conversely, Dorian et al found that a range of cardiovascular parameters had no significant impact on HRQOL, including NYHA class, coronary artery disease, hypertension, left ventricular function, AF frequency, or AF duration.50 Regardless of the impact of other conditions, the classification of AF as paroxysmal, persistent, or permanent may have a greater influence on both general and disease-specific AF assessments. Numerous investigations have shown that patients with paroxysmal disease report more frequent, invasive, and severe symptoms of AF than those with persistent or permanent disease; however, increased symptom reports do not always correlate with decreased perception of HRQOL.95,96 When developing and validating the Canadian Cardiovascular Society Severity of Atrial Fibrillation Scale, investigators found that persistent or permanent AF patients had lower HRQOL than those with paroxysmal AF.48 Other studies have found that those affected by paroxysmal, persistent, or permanent AF have similar levels of HRQOL.64 These results may be influenced by the subject’s rhythm at the time of assessment: prior research has shown that AF patients in sinus rhythm while completing an HRQOL measure score higher than those in AF.97 Clinical trial investigators should strive to evaluate rhythm throughout the HRQOL instrument administration process.
Limitations Of Traditional Assessments Of Symptoms, Affect, And Functional Status
Current approaches to the assessment of symptoms during clinical visits are problematic for several reasons. These data are traditionally collected via recall that requires participants to summarize their experiences over some time period (i.e. since the last clinic visit). Therefore the events that are easily recalled are more likely to be reported during the retrospective reporting of events.98 The recall of an event can also be influenced by other events occurring after the event to be recalled (retroactive reconstruction), individual’s beliefs about the condition (effort after meaning), and affect.99 Another concern is that the assessments of symptoms, affect, and functional status are not performed objectively in patient’s natural settings, therefore limiting their generalizability and ecological validity.100 This emphasis on retrospective assessment prevents the study of dynamic changes in symptoms over time and their interaction with heart rhythm, affect, and functional status. There is a need for time sensitive study designs with repeated assessments of rhythm, symptoms, and affect to capture the daily variability in symptoms and that can increase our understanding of the dynamic interplay between physiology, psychology, patient reported symptoms, and moment-to-moment functioning in daily life.
Table 3. Analysis of AF-Specific Classification Tools/Symptom Scales
| Classification Tool/Symptom Scale |
Patient or Provider Completed? |
Classifications or Scoring Method |
Length of Recall Period |
Validation Strategy |
Specific Advantages |
| EHRA47 |
Provider |
-4 total classifications
-Patients classified based on AF’s impact on ability to complete daily activities |
-Immediate Assessment |
-Validated against AFEQT and EQ-5D |
-Simple classification system for efficient bedside use |
| mEHRA46 |
Provider |
-5 total classifications
-Patients classified based on AF’s impact on ability to complete daily activities
-Subset of patients scored based on “troublesome” nature of symptoms |
-Immediate Assessment |
-Validated against AFEQT and EQ-5D |
-Increased granularity compared to standard EHRA |
| CCS-SAF48 |
Provider |
-5 total classifications
-Patients classified based on symptom’s perceived impact on overall HRQOL |
-Immediate Assessment |
-Validated against SF-36 and AFSS |
-More detailed classifications as compared to EHRA/mEHRA
-Assesses symptom severity with respect to HRQOL |
| AFSS50 |
Patient |
-14 total questions assessing symptom severity, frequency, and duration
-Objective and subjective measure of AF symptom impact |
- |
- |
-Patient
-reported outcome measure |
| SCL51 |
Patient |
-Separate assessments of symptom severity and burden.
-Higher scores indicate more frequent/severe symptoms |
- |
- |
-Patient
-reported outcome measure |
| AFS/B52 |
Patient |
-4 classifications of symptom and burden severity
-14 total questions: Eight focus on symptoms in daily life, six focus on AF frequency, duration, and healthcare use |
-Current Status |
-Validated against SF-12 (V2) |
-Both patient and provider complete instrument. |
*Authors were unable to determine validation strategies or recall lengths for the AFSS and SCL. §EHRA: European Heart Rhythm Association Classification. mEHRA: Modified European Heart Rhythm Association Classification. CCS-SAF: Canadian Cardiovascular Society Symptoms Severity in Atrial Fibrillation. AFSS: Atrial Fibrillation Symptom Severity. SCL: Symptom Checklist. AFS/B: Atrial Fibrillation Symptom and Burden.
Mobile Application To Assess Symptoms And Affect In Patients With AF (miAfib app)
Investigating the temporal sequence of affect and cardiac dysfunction represents significant methodological challenges that are not addressed with one-time assessments of affect during clinic visits. The prospective real-time assessments regarding how a person feels over a period of time have demonstrated an association between negative affect, acute cardiac dysfunction, and poor long-term survival. Despite the evidence suggesting an association between affect and symptoms in cardiovascular disease, there have not been studies evaluating their relationship in patients with AF.
Developments in mobile technology have created opportunities for people to assess their symptoms during times (real time) and in places or situations (real world) when they are most needed. Mobile technology is ideal for the recording of symptoms because these devices are relatively small and convenient for people to carry as they go about their daily lives. We have developed a novel mobile application (miAfib) to assess symptoms (chest pain, palpitation, shortness of breath, fatigue, dizziness/lightheadedness), and positive (happy, excited, content) and negative (worried, angry, sad) affect on multiple occasions throughout the day. The application is based on the iOS platform for iPhone and is available through the app store for download by study participants (Figure 2). We designed a study website (www.miAfib.com) to assist participants with mobile application set up and study details.
We conducted a feasibility trial to examine the user adherence, acceptance, and experiences over a 21-day period. The protocol was approved by IRB and informed written consent was obtained. For initial feasibility testing, we recruited 10 patients with paroxysmal AF for 21 days. At the end of the trial, we conducted a structured interview asking the patients to complete a questionnaire consisting of five point Likert scaled questions (strongly agree to strongly disagree) designed to measure ease of use (“I found the app easy to use”), convenience and integration into daily practice (“I found the app fit into my routine”), and future intention to use the application (“I intend to use the app in the future”). Participants completed 1.70±0.84 assessments per day. All of these entries contained complete information. Descriptive statistics showed that users found the application easy to use (M=4.67±0.52), intended to use the application in the future (M=4.83±0.41), and easily integrated the application into their daily routines (M=4.50±0.55). These descriptive data suggest that the application was easy to use and users would consider its continued use. The relationship between heart rhythm, affect and palpitations during multiple evaluations is shown in Figure 3.
There is a complex and poorly understood interplay between symptoms, heart rhythm, affect and functional status in patients with AF. Our understanding of this relationship has been hampered by our current assessment paradigm that is focused on evaluations at one point in time (typically a clinical visit). Mobile and sensor technologies offer novel methods for evaluating symptoms and functional status in patients with AF and can give us a unique and never-before-seen window into this disease. Future research is needed to evaluate the role of these technologies in evaluation and treatment of patients with AF.






