Management of Atrial Fibrillation Post Bypass Surgery with Intravenous Sotalol: A Case Study
Sergio F. Cossú
The Arrhythmia Center at Charlotte Heart and Vascular Institute.
Intravenous sotalol has been available for many years outside of the United States, but has only recently become available in the US. The safety and feasibility of intravenous sotalol for the prevention of recurrent atrial fibrillation following bypass surgery has not been described. The present case study is of a patient with several other co-morbidities undergoing coronary artery bypass graft surgery, who post-operatively developed atrial fibrillation. The patient received intravenous sotalol and was then transitioned to oral sotalol. The patient remained hemodynamically stable, with normal QTc and without further atrial fibrillation or tachyarrhythmias in the post-operative period until discharge. Intravenous sotalol is a reasonable alternative to intravenous amiodarone in the post bypass surgery patient with better tolerability and safety profile.
Correspondence to: 3340 Tamiami Trail Port Charlotte, FL 33952
Atrial fibrillation is commonly encountered following open heart surgery, with an incidence of approximately 20 – 40% in this patient population [1], [2]. Although many of these episodes are short lived and self-terminating, at times it may result in significant hemodynamic compromise as well as further complications. Studies have shown that patients developing atrial fibrillation following cardiac surgery have a significant increased risk of thromboembolic phenomenon, stroke, congestive heart failure, myocardial infarction and mortality compared to patients who maintained sinus rhythm [1], [3]. In addition, the cost of managing atrial fibrillation following open heart surgery is also significantly higher due to the prolonged ICU stay as well as use of other resources. The choice of anti-arrhythmic drug therapy is quite limited. Until recently the only intravenous antiarrhythmic medication available in the United States was amiodarone. The acute hemodynamic effects as well as the long-term side effect profile of the oral form of this medication makes this a less than desirable option for the management of these post open heart surgical patients. We present a case in which intravenous sotalol was utilized in this scenario with a positive patient outcome.
The patient is a 73-year-old male with a history of coronary artery disease (CAD) status post anteroseptal myocardial infarction in 1993, for which he underwent TPA administration. In August, 2000, the patient also underwent stent placement to the left anterior descending artery and the right coronary artery. The patient recently presented with complaints of unstable angina and underwent stress testing which demonstrated a large reversible defect involving the anteroseptal wall. Coronary angiography demonstrated an 80% left main stenosis as well as restenosis involving the right coronary artery. His left ventricular systolic function was approximately 40%.
His past medical history is notable for CAD, as mentioned above, as well as a history of chronic obstructive pulmonary disease (COPD), hypertension, hyperlipidemia, and hypothyroidism. The patient also has a history of an underlying chronic left bundle branch block.
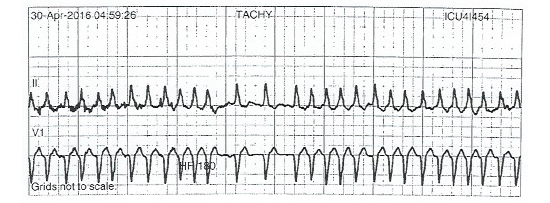
The patient subsequently underwent coronary artery bypass graft surgery with a left internal mammary artery to the left anterior descending artery and the obtuse marginal as well as a saphenous vein graft to the right coronary artery. On his third post-operative day, the patient developed a sustained episode of atrial fibrillation with ventricular rates of 180 – 200 bpm [Figure 1]. The patient was symptomatic with these episodes of atrial fibrillation associated with chest pain, palpitations and dyspnea, as well as becoming somewhat hypotensive with a systolic blood pressure of 90 – 100 mm Hg. These episodes of atrial fibrillation would self-terminate and then re-initiate abruptly. Per ICU protocol the patient was initially started on amiodarone at a rate of 1 mg/min without a bolus.
Figure 1. Figure illustrates an episode of atrial fibrillation with a rapid ventricular response rate (180 – 200 bpm) in this patient. Underlying intraventricular conduction defect consistent with a left bundle branch block is noted.
At the time of our assessment the patient had received approximately 2 hours of amiodarone therapy. It was decided that, due to the patient’s history of CAD as well as underlying COPD, that he would be better suited with sotalol rather than amiodarone therapy. We were quite concerned about the long-term effects on his lung function as well as the potential hypotension associated with IV amiodarone. His creatinine clearance measured 129.41 mL/min. Potassium and magnesium levels were within normal range. Amiodarone was discontinued, and after approximately 6 hours, the patient received sotalol 75 mg IV infusion over 5 hours. The patient was monitored in the ICU. His QTc remained stable throughout the entire infusion. On the following day, he was switched to oral sotalol 80 mg twice daily. He remained in sinus rhythm throughout the remainder of his hospital stay without any further arrhythmias. QTc remained within normal range corrected for his left bundle branch block.
The present case demonstrates a situation in which we were able to administer intravenous sotalol for the management of post-operative atrial fibrillation following coronary artery bypass graft surgery. The patient had initially received amiodarone as part of the hospital protocol. Although the side effects of amiodarone are usually experienced when given in high doses for a prolonged period of time, we were concerned about the long-term use of amiodarone in this patient with underlying lung disease. Obviously the administration of sotalol could potentially have had increased effects on the patient’s QTc interval after having received amiodarone. By administering sotalol as an infusion over 5 hours we were able to monitor the QTc carefully during the entire infusion, and if necessary, modify or discontinue its infusion if a QTc prolongation was observed or if Torsades de Pointes were to occur. The QTc was able to be corrected despite his underlying chronic left bundle branch block. The patient was already in the intensive care unit following his bypass surgery and thus provided the best environment for the use and monitoring of this medication. Since we were able to quickly transition the patient to its oral counterpart, the use of IV sotalol did not prolong the patient’s ICU stay.
The management of atrial fibrillation in the post open heart patient can be somewhat difficult. Class I-C antiarrhythmic agents are contraindicated in the setting of coronary artery disease, thus Class III agents, including amiodarone, sotalol or dofetilide are the medications currently utilized in this scenario. Until the introduction of intravenous sotalol, the only one of these agents available in an intravenous formulation was amiodarone. Intravenous amiodarone has been shown to cause hypotension, thus making it difficult to control the hemodynamics in these very tenuous patients. Further, upon transitioning to oral form, the side effect profile of long-term amiodarone use can have serious long-term consequences. The SAFE-T trial compared the use of sotalol and amiodarone for the acute conversion as well as maintenance of sinus rhythm. The investigators found similar rates of efficacy between the two agents, especially with respect to the median time in recurrence of atrial fibrillation in patients with ischemic heart disease [4]. Two further studies evaluated amiodarone vs. oral sotalol in the post bypass population and found similar efficacy and discontinuation rates [5],[6]. Piccini and colleagues recently reported the safety in the long term use of sotalol vs. amiodarone in patients with ischemic heart disease.
Although sotalol was associated with an increased mortality compared to no antiarrhythmic drug therapy, the mortality rate was less compared to the use of amiodarone [7]. A recent meta-analysis by Somberg et al comparing amiodarone vs. sotalol for the management of atrial fibrillation demonstrated similar rates of acute conversion (risk ratio = 0.947, 95% CI: 0.837 – 1.071, p = 0.387) [8]. Similarly, the maintenance of sinus rhythm was not statistically different between amiodarone or sotalol (RR = 1.05, 95% CI: 0.625 – 1.774, p = 0.847) [8]. In another recent meta-analysis, the use of sotalol, both IV as well as oral, was found to be similar to Class I-A and Class I-C antiarrhythmic agents in the acute conversion of atrial fibrillation [9]. These studies demonstrated the efficacy of long-term oral sotalol in comparison to amiodarone, however it is important to also evaluate their safety. Intravenous amiodarone has been described to cause hypotension, bradycardia, heart block as well as Adult Respiratory Distress Syndrome (ARDS). Acute hepatic injury has been described in 2.8-4.2% of patients receiving IV amiodarone. The long term side effect profile of oral amiodarone can include pulmonary fibrosis, hypothyroidism, hyperthyroidism, optic neuritis, hepatitis and peripheral neuropathy. Other less concerning side effects include corneal deposits and skin discoloration [10]. Somberg et al described in their meta-analysis the adverse events related to both acute and chronic amiodarone or sotalol therapy [8]. Compared to amiodarone, sotalol had significantly lower incidence of the aforementioned adverse events with the exception of bradycardia and AV block (12-13% vs. 4.9% for amiodarone) and fatigue (10–11% vs. 4 -9% for amiodarone). The incidence of Torsades de Pointes with both the acute intravenous form as well as the chronic oral route of amiodarone is quite rare (<2%). Torsades de Pointes, on the other hand, has been demonstrated to be quite common in patients receiving chronic oral sotalol (2-4%) [11]-[13]. This is primarily due to its effect on QTc prolongation. Conversely, in a meta-analysis studying 962 patients receiving IV sotalol, the risk of Torsades de Pointes with IV sotalol was 0.1%, significantly lower than with oral sotalol [14]. Piccini et al did discuss that although the all-cause mortality of patients receiving sotalol was greater compared to patients receiving no antiarrhythmic drug therapy, there was a significantly decreased mortality compared to amiodarone (hazard ratio 0.72, 95% CI: 0.55 – 0.91, p = 0.0141) [7]. Although dofetilide is also a potential option in this patient population as well, it is only available in oral form and one also has to weigh the potential risks of QTc prolongation as well as the risk of Torsades de Pointes [15].
In conclusion, intravenous sotalol provides a much safer and efficacious option in the management of post-operative atrial fibrillation in comparison to intravenous amiodarone. The ability to then transition these patients to oral sotalol provides a better long-term side effect profile compared to oral amiodarone. The infusion of sotalol over a period of five hours also gives the flexibility of halting the drip if any ventricular arrhythmias are observed. This would obviously not be possible after a patient consumed an oral dose of sotalol. The success in the ability for IV sotalol to convert post-operative atrial fibrillation provides another tool for the manegement of these patients compared to the standard amiodarone therapy. The clinician prescribing these antiarrhythmic agents should be aware of all potential effects of these drugs and be familiar with their dosing.






