Management of Patients with Atrial Fibrillation: Focus on Treatment Options
Paweł T Matusik, MD, PhD12, Jacek Lelakowski, MD, PhD13, Barbara Małecka, MD, PhD13, Jacek Bednarek, MD, PhD1, Remigiusz Noworolski, MD1
1Department of Electrocardiology, The John Paul II Hospital, Kraków, Poland.2Jagiellonian University, Medical College, Kraków, Poland.3Institute of Cardiology, Jagiellonian University, Medical College, Kraków, Poland.
Atrial fibrillation (AF) is leading cardiac arrhythmia with important clinical implications. Its diagnosis is usually made on the basis on 12-lead ECG or 24-hour Holter monitoring. More and more clinical evidence supports diagnostic use of cardiac event recorders and cardiovascular implantable electronic devices (CIED). Treatment options in patients with atrial fibrillation are extensive and are based on chosen rhythm and/or rate control strategy. The use and selected contraindications to AF related pharmacotherapy, including anticoagulants are shown. Nonpharmacological treatments, comorbidities and risk factors control remain mainstay in the treatment of patients with AF. Electrical cardioversion consists important choice in rhythm control strategy. Much progress has been made in the field of catheter ablation and cardiac surgery methods. Left atrial appendage occlusion/closure may be beneficial in patients with AF. CIED are used with clinical benefits in both, rhythm and rate control. Pacemakers, implantable cardioverter-defibrillators and cardiac resynchronization therapy devices with different pacing modes have guaranteed place in the treatment of patients with AF. On the other hand, the concepts of permanent leadless cardiac pacing, atrial dyssynchrony syndrome treatment and His-bundle or para-Hisian pacing have been proposed. This review summarizes and discusses current and novel treatment options in patients with atrial fibrillation.
Key Words : Atrial Fibrillation, Treatment, Ablation, Pacemaker, ICD, CRT.
Correspondence to: Paweł T. Matusik, Department of Electrocardiology, The John Paul II Hospital, Prądnicka 80 Street, 31-202 Kraków, Poland.
Atrial fibrillation (AF) is the most prevalent cardiac arrhythmia with important clinical implications.[1] In 2010, AF affected 33.5 million of individuals globally and was described as ‘growing epidemic’.[1] AF decreases health related quality of life[2] and substantially contributes to cardiovascular morbidity and mortality especially in women.[3] Variety of possible causative risk factors and diseases, comorbidities, as well as possible complications resulting from AF require comprehensive assessment and management of patients with atrial fibrillation (Fig 1). It refers also to screening of general population and especially subjects at risk of atrial fibrillation.[4,5] Screening of patients ranges from simple pulse assessment, through various forms of electrocardiography monitoring (including symptom event monitors and looping memory monitors), to active search of atrial high rate episodes (AHRE) in patients with cardiovascular implantable electronic devices (CIED).[6] Especially after cryptogenic stroke insertable cardiac monitors represent reasonable AF diagnostic approach.[7] CIED as well as AF ablation techniques are more and more accessible in current clinical practice and possess great potential in the treatment of patients with AF. Their application will be the focus of current review.
Figure 1. Overview of clinical management of patients with atrial fibrillation
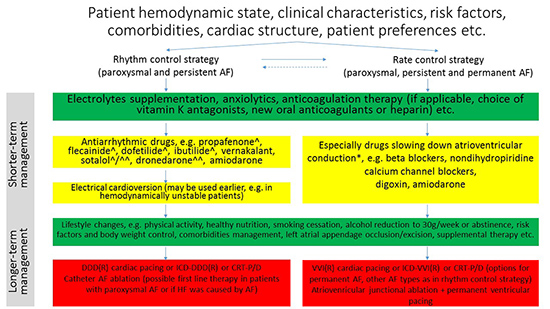
AF, atrial fibrillation; HF, heart failure; DDD, dual chamber pacemaker; ICD, implantable cardioverter-defibrillator; CRT-P/D, cardiac resynchronization therapy-pacemaker/defibrillator. ^ not recommended in left ventricular hypertrophy >15mm or ≥14mm (ibutilide) ^^ not for cardioversion. * some of these drugs should not be used in decompensated heart failure and/or in patients with pre-excitation
Overview of Clinical Management of Patients with Atrial Fibrillation
In non-emergency clinical situations before choice of clinical strategy patient clinical characteristics, risk factors, comorbidities, cardiac structure and patient preferences should be assessed and each patient should be managed individually (Fig. 1). It should be accompanied with knowledge of specific contraindications, proarrhythmic effects and noncardiovascular toxicities of antiarrhythmic drugs.[8] Especially reversible AF causes should be targeted. In the assessment of the risk of AF progression HATCH (Hypertension, Age ≥75 years, previous Transient ischemic attack/stroke [2 points], Chronic obstructive pulmonary disease and Heart failure [2 points]) scale may be utilized.[9,10]
Adequate rhythm and ventricular rate control prevent hemodynamic disturbances. Based on AF symptoms frequency „pill-in-the-pocket” (propafenone or flecainide added to beta blocker or nondihydropyridine calcium channel antagonist) may be the choice of treatment especially in the early phase of AF, in patients without advanced structural heart disease, once revealed to be safe in a monitored setting.[11,12] Patients with severe heart failure should be treated with amiodarone. Using amiodarone the pharmacological cardioversion to sinus rhythm is achieved later than in the case of class Ic drugs.[13] Electrical cardioversion, when compared to pharmacological cardioversion is more effective, particularly in persistent AF.[13] On the other hand AF symptoms duration ≥ 48 hours (or of unknown duration), patients requiring anticoagulation therapy, remain contraindications (not in hemodynamically unstable patients) to both pharmacological and electrical cardioversion if anticoagulation was not introduced at least 3 weeks earlier or left atrial thrombus was not excluded.[12,14] In patients assessment echocardiography has an important role which it not only helps to guide management strategy, but also the choice of drugs.
The rate control strategy focuses on slowing down atrioventricular conduction. The drugs used in this strategy include beta-blockers, nondihydropyridine calcium channel blockers, digoxin and especially in resistant to treatment subjects amiodarone. The resting heart rate target of <80 beats per minute (bpm) or <110 bpm during moderate exercise (or resting if lenient rate-control strategy is applicable) should be achieved.[12,15] However, we should take into account that ventricular rates <70 bpm may be associated with a worse outcome and current European Society of Cardiology guidelines for patients with heart failure (HF) and AF recommend resting heart rate of 60-100 bpm as optimal target value.[16]
Thromboembolic and bleeding complications prevention is one of the most important goals in treatment of patients with AF. Scales important in their risk assessment include CHA2DS2-VASc (Congestive heart failure/ left ventricular dysfunction, Hypertension, Age ≥75 years [2 points], Diabetes mellitus, Stroke/ transient ischemic attack/thromboembolism [2 points], Vascular disease (prior myocardial infarction, aortic plaque or peripheral artery disease), Age 65-74 years, Sex category [female gender])[17] and HAS-BLED (uncontrolled Hypertension, Abnormal renal/liver function [1 or 2 points], Stroke previous history, Bleeding history or predisposition [anemia], Labile international normalized ratio [INR], Elderly [> 65 years], Drugs/alcohol use [1 or 2 points])[18] scores. These scales calculate risk of stroke/peripheral embolism/pulmonary embolism or risk of major bleeding, respectively. Moreover, inclusion of persistent form of AF and renal impairment, beside CHA2DS2-VASc score, may be considered and may lead to achievement of greatest area under the curve.[19,20] Based on risk stratification of thromboembolic complications anticoagulation therapy use must be considered. One should take into account, that new, promising players appear and become more and more common on the stage of anticoagulation therapy and currently in eligible patients non-vitamin-K oral anticoagulants are recommended as the first-line anticoagulants.[21,22,80] Bleeding risk management should especially focus on modifiable bleeding risk factors correction and if high bleeding risk is present it should generally not be a contraindication to anticoagulation.[80] On the other hand in AF patients with clear contraindications for long-term oral anticoagulation therapy left atrial appendage (LAA) occlusion may be considered for stroke prevention.[14,80] LAA occlusion may be performed using endocardial percutaneous intracardiac occluder (WATCHMANTM, Amplatzer Cardiac Plug) and epicardial left atrial appendage ligation via pericardiac sack (LARIAT, AtriClip®).[23,24] According to recently published data, LAA occlusion may eliminate significantly the risk of thromboembolic complications.[24,25] LAA surgical occlusion or exclusion may be considered in AF patients undergoing cardiac surgery as well as thoracoscopic AF surgery.[14,24,80] Extracardiac LAA ligation may be performed via thoracoscopy or percutaneously.
In both AF treatment strategies upstream therapies should be considered. Intensive risk factors management, including hyperlipidaemia, hypertension, diabetes, smoking and obstructive sleep apnoea may increase clinical success rates.[26] Moreover exercise and alcohol abstinence (or reduction to 30g per week) should also be taken into consideration.[26] As mean body mass index (BMI) among patients with AF is elevated,[27,28] importance of weight management needs to be emphasized. In a study by abed and colleagues, in patients with obesity and symptomatic AF, with a median follow up of 15 months duration it was found that weight management with intensive management of cardiometabolic risk factors (intervention group) was superior to intensive management of cardiometabolic risk factors and general lifestyle advice in achieving weight reduction and reduction of AF symptom burden and severity scores, number of episodes and cumulative duration.[29] Interestingly in both studied groups reduction of interventricular septal thickness and left atrial area were observed and were more pronounced in the intervention group.[29] Long-Term Effect of Goal directed weight management on Atrial Fibrillation Cohort: A 5 Year follow-up (LEGACY) study revealed that in patients with AF and BMI ≥27kg/m2 sustained (particularly with evasion of weight fluctuation), long-term weight loss associates (in a dose dependent manner) with AF burden reduction and maintenance of sinus rhythm.[30] Furthermore, these changes associate with beneficial alterations in risk factors and cardiac remodeling.[30]
Ablation in The Treatment of Atrial Fibrillation
Atrial fibrillation ablation eliminates the arrhythmogenic triggers, substrate and/or improper impulses propagation. Promising effects of new ablation devices influence increase in number of candidates for AF ablation and lead to decrease in complications rate. Taking into account patients preferences as well as outcomes associated with catheter AF ablation, it should be considered in selected patients with symptomatic paroxysmal AF (as first-line therapy) and in cases of ineffective pharmacological treatment of persistent AF (Fig. 2).[14,80] It is generally indicated in symptomatic recurrences of paroxysmal AF during antiarrhythmic drug therapy. Moreover in management of AF patients AF Heart Teams have been proposed.[12,80] Tachycardiomyopathy is another clinical situation in which AF ablation may be performed before use of antiarrhythmic pharmacotherapy.[14] This recommendation seems to be in line with results of recent clinical trial, which has shown, that catheter ablation of persistent AF in patients with HF was found to be superior to amiodarone in achieving no AF recurrence at long-term follow-up and reduction in unplanned hospitalizations and mortality.[31] Catheter or surgical ablation of AF should be considered in symptomatic patients with persistent AF or long-standing, persistent AF refractory to antiarrhythmic medication (Fig. 2).[80] Healthier, younger individuals may benefit more from ablation than elderly patients with multiple comorbidities. However, benefits of AF ablation in patients ≥ 75 years old were shown to be effective in reducing mortality and stroke risk.[32] AF arrhythmogenic substrate location is often poorly defined so its targeting has probalilistic nature. The most common AF origins are, atrial muscle sleeves extending to pulmonary veins (ca. 80%), left atrial posterior wall, superior caval vein, oblique vein/ligament of Marshal, terminal crest, coronary sinus and interatrial septum.[33] AF ablation may be performed from the endocardial side using catheters introduced via femoral vein and transseptal puncture. Alternatively, epicardial ablation by open heart surgery (often performed in conjunction with other cardiac surgery) or via a thoracoscopic or mediastinal approach. Moreover the hybrid procedures are also performed. The most common techniques in AF ablation is pulmonary veins isolation (PVI) without or with lines and/or complex fractionated atrial electrogram (CFAE) ablation.[34] Regarding to freedom from total tachyarrhythmia during long-term follow-up, it was shown, that wide antral circumferential ablation (WACA) approach (ablation ≥1.5 cm away from PV ostium) in PVI is more effective than ostial PVI.[35] Some of the most frequent lines in catheter AF ablation are the “roof line”, the “mitral isthmus line” and anterior linear lesion.[36,37] In patients with history of cavotricuspid isthmus dependent atrial flutter or if it was induced during EP testing additional linear lesion at the cavotricuspid isthmus is also placed.[37]
Figure 2. Overview of atrial fibrillation ablation indications
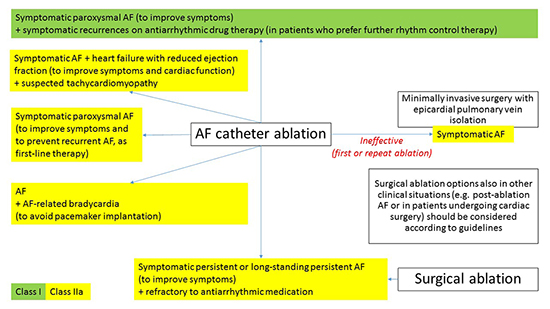
AF, atrial fibrillation
Atrial fibrillation ablation may be performed using radiofrequency energy, cryothermy, laser, ultrasound or microwave energy, some of them remain still at the initial stage.[38] Recent clinical trial (The FIRE AND ICE Trial) revealed that cryoballoon ablation was noninferior to radiofrequency ablation (the most common method, with the use of electroanatomical mapping system) in patients with drug-refractory paroxysmal atrial fibrillation.[39] The recommendations regarding atrial fibrillation ablation by PVI technique point that electrical PV isolation should be the goal and entrance block into PV should be demonstrated. Moreover reconduction assessment 20 minutes following initial procedure should be considered.[37]
Cardiovascular Implantable Electronic Devices in Management of Atrial Fibrillation
Many clinically interesting cardiovascular implantable electronic devices functions were shown to have significant impact on the course of AF and clinical management of patients with AF. CIED play important role both in the diagnosis and treatment of atrial fibrillation. Incidence of pacemaker-detected AF may reach 50% and its burden is associated with increased stroke risk.[40,41] However, it was found that patients with subclinical pacemaker-detected AF are significantly less frequently treated by anticoagulants than patients with clinical AF.[40] On the other hand remote control of CIED enables early detection of AF and/or optimization of treatment.[42]
Cardiac implantable electronic devices in treatment of AF are generally reserved for clinical situations in which lifestyle changes and pharmacological and/or ablation treatments are ineffective. Choice of pacing mode in patients with AF is very important. In patients with paroxysmal or persistent AF and concomitant sinus node disease and/or atrioventricular (AV) conduction disturbances atrioventricular rate – responsive pacing (DDDR) is indicated (rhythm and rate control). Ventricular rate responsive cardiac pacing (VVIR) is used in patients with advanced AV conduction disturbances in the course of permanent AF (heart rate control), Fig. 3.[12,14] Importantly permanent leadless cardiac pacing may possess valuable treatment option especially in this group of patients.[43]
Figure 3. Overview of current options and/or guidelines recommendations for cardiovascular implantable electronic devices use in patients with AF. Based on,[57,58] other references are cited throughout the text
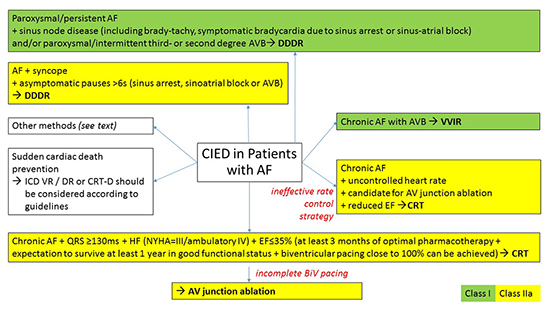
AV, atrioventricular; AVB, atrioventricular block; CIED, cardiovascular implantable electronic devices; EF, ejection fraction; NYHA, New York Heart Association; BiV, biventricular; other abbreviations as in Fig. 1
Atrial fibrillation is frequent in patients with heart failure (HF).[44,45] There are two groups of indications for CIED implantation in patients with AF and HF. The first group includes patients with AF and HF, who are often characterized by prolonged ventricular depolarization (especially QRS ≥ 130ms) and decreased left ventricular ejection fraction (EF≤35%)[81] and the second, in which left ventricular dysfunction results from long standing fast heart rate. Patients in both clinical categories may benefit from improved heart rhythm and/or heart rate control. MUltisite STimulation In Cardiomyopathies (MUSTIC) study evaluated the effects of biventricular pacing in HF patients in New York Heart Association (NYHA) class III and intraventricular conduction delay. It revealed clinical benefits according to improved 6-min walked distance, quality of life and NYHA class, also in patients with AF.[46] In the Ablate and Pace in Atrial Fibrillation (APAF) trial ‘Ablate and Pace’ therapy for severely symptomatic chronic AF was tested.[47] In this study cardiac resynchronization therapy (CRT) was superior to apical right ventricular pacing in reducing clinical manifestations of HF in patients undergoing AV junction ablation.[47] On the other hand subgroup analysis of the Resynchronization–Defibrillation for Ambulatory Heart Failure Trial (RAFT) revealed, that in patients with permanent AF or atrial flutter, HF (NYHA class II-III), a LVEF ≤30% and an intrinsic QRS ≥120ms or a paced QRS ≥200ms, who received an CRT-D device did not differ from those who received implantable cardioverter-defibrillator (ICD) alone, when death or HF hospitalization were taken into account (composite primary outcome).[48] Therefore indications to implant CRT in patients with permanent AF and without significant bradyarrhythmias is discussed, especially because large registry data have shown, that atrial tachycardia/AF was the most prevalent reason for CRT pacing loss.[49]
However, systematic review revealed that patients with AF undergoing CRT for symptomatic heart failure and left ventricular dyssynchrony, after AV nodal ablation compared with medical therapy aimed at rate control, had significantly reduced all-cause and cardiovascular mortality as well as had improved NYHA class.[50] On the other hand, we have to keep in mind, that patients after AV nodal ablation are pacing device dependent.
Patients with AF and increased sudden cardiac death (SCD) risk may benefit from implantable cardioverter-defibrillators as SCD preventive therapy. However, after ICD implantation for primary or secondary prevention, during median follow-up of 3 years, about 21% of patients suffer from inappropriate ICD shocks and 60% of them result from AF.[51] Moreover multiple (≥2) ICD shocks due to AF are associated with worse prognosis, while single shock resulting from AF or shocks due to lead failure are not.[51] It is crucial in ICD programming to know discrimination algorithms, including interval stability and atrioventricular association discriminator in dual-chamber ICD differentiating AF from fast ventricular rhythms.[52]
Moreover, in selected patients with AF, especially with concomitant heart failure, requiring permanent cardiac pacing, His-bundle or para-Hisian pacing may possess a therapeutic option.[53-56] However, this mode of pacing limitations include intraventricular conduction disturbances.
Overview of current options and/or guidelines recommendations for CIED implantation in patients with AF are shown on Fig. 3.[57,58]
Permanent Cardiac Pacing and Reduction of AF
Influence of pacing mode on AF was tested in Canadian Trial Of Physiologic Pacing (CTOPP).[59] Results of CTOPP have shown, that patients who underwent physiologic (atrial based) pacing (AAI or DDD) were less likely to develop chronic AF, than patients who underwent ventricular-based pacing.[59] Similar results were also found in our study, in which we have found that DDD pacing mode was associated with lower rate of AF de novo than VVI pacing mode.[60] Surprisingly, subgroup analysis of CTOPP revealed, that in patients with myocardial infarction/coronary artery disease or abnormal left ventricular function, there was no benefit regarding chronic AF development resulting from physiologic pacing.[59] The current look, takes into account the detrimental effect of high right ventricular pacing percentage and enables us to assess the results of the CTOPP study differently.[61,62]
In patients after total AV junction ablation, without antiarrhythmic therapy, DDDR cardiac pacing, compared with VDD pacing (PA3 Trial) did not prevent paroxysmal AF.[63] This data also suggest, that ventricular pacing (also in synchronous mode) promotes AF.[64] Therefore, DDD(R) pacemakers with programmed algorithms promoting spontaneous AV conduction should be prefered in most pacemaker patients without permanent AF and significant AV conduction abnormalities.[65]
Cardiac resynchronization therapy may influence atrial fibrillation and possess antiarrhythmic effects.[66-68] Gasparini and colleagues, found that end-diastolic diameter ≤65 mm, left atrium ≤50 mm, post-CRT QRS ≤150 ms and atrioventricular junction ablation appear to be predictive of spontaneous sinus rhythm resumption in heart failure patients with permanent AF after CRT introduction.[68] However, in the CArdiac REsynchronisation in Heart Failure (CARE-HF) trial, CRT did not reduce the incidence of AF.[69] It should be emphasized that in the Management of Atrial fibrillation Suppression in AF-HF COmorbidity Therapy (MASCOT) trial it was revealed that the atrial overdrive pacing did not lower the 1-year incidence of AF in a group of CRT recipients.[70]
Interestingly, the interaction between electrical impulses in the right and left atrium may be important to sustain AF.[71] Electrical activation between atria occurs by preferential conduction pathways, such as Bachmann’s bundle, fossa ovalis rim and coronary sinus.[71] Atrial conduction disturbances due to primary disease, AF recurrences and/or AF ablation may lead to atrial dyssynchrony and be a risk factor for atrial fibrillation.[72,73] It may therefore be targeted by atrial resynchronization through multisite atrial pacing (including Bachmann’s bundle area and coronary sinus ostium pacing), atrial septal pacing, coronary sinus or biatrial pacing.[72,74-79] However, concept of atrial dyssynchrony syndrome treatment needs more research evidence before it could be widely used in clinical practice.[72]
Treatment options in atrial fibrillation are extensive and are based on chosen rhythm and/or rate control strategy. Indications for anticoagulation therapy must be considered in all AF patients. Nonpharmacological treatments, comorbidities and risk factors control remain mainstay in the treatment of patients with AF. Electrical cardioversion consists important choice in rhythm control strategy. Much progress has been made in the field of catheter ablation and cardiac surgery methods. Left atrial appendage occlusion/closure may be beneficial in patients with AF. CIED are used with clinical benefits in both, rhythm and rate control. Pacemakers, implantable cardioverter-defibrillators and cardiac resynchronization therapy devices with different pacing modes have guaranteed place in the treatment of patients with AF.






