Esophageal Temperature Monitoring During Radiofrequency Ablation of Atrial Fibrillation: A Meta-Analysis
Ketan Koranne1, Indranill Basu-Ray1, Valay Parikh2, Mark Pollet1, Suwei Wang1, Nilesh Mathuria1, Dhanunjaya Lakkireddy2, Jie Cheng1
1Cardiac Arrhythmia Service, Texas Heart Institute and Baylor CHI St Luke’s Medical Center, Baylor College of Medicine, Houston, Texas;.2Division of Cardiovascular Diseases, Cardiovascular Research Institute, University of Kansas Hospital and Medical Center, Kansas City, Kansas.
Objective: Atrio-esophageal fistula is an infrequent but devastating complication of catheter-based ablation of atrial fibrillation (AF). Thermal esophageal injury may be the precursor of atrio-esophageal fistula. Here, we evaluated the role of esophageal temperature monitoring in preventing thermal esophageal injury during pulmonary vein isolation for AF with radiofrequency energy.
Methods: In this meta-analysis, we searched the PubMed, Cochrane, Scopus, Embase, and Refworks databases for all published studies from January 2004 to June 2016 to evaluate the role of esophageal temperature monitoring. We searched for terms esophageal temperature monitoring, AF, radiofrequency ablation, atrio-esophageal fistula, and thermal esophageal injury. We included studies comparing luminal esophageal temperature (LET) monitoring with no LET monitoring during radiofrequency ablation of AF. We excluded studies in which post-ablation esophagogastroduodenoscopy (EGD) was not performed to identify esophageal thermal injuries. To perform the meta-analysis, we used Review Manager statistical software and a fixed-effects modeling to derive the outcomes. Given significant heterogeneity between the studies, we used meta-regression analysis to adjust for age and sex.
Results: We identified 4 non-randomized controlled trials that met our search criteria and included a total of 411 patients (n=235 in the LET monitoring group; n=176 in the no LET monitoring group) in the analysis. There were 21 (8.9%) patients with thermal esophageal injury in the LET monitoring group and 12 (6.8%) in the no LET monitoring group. The pooled odds ratio was 0.66 (0.23-1.89), indicating no statistically significant differences between the 2 groups with regard to esophageal injury. Because of the small sample size and the non-randomized nature of the trials, we observed significant heterogeneity in outcomes among the trials.
Conclusion: The role of esophageal temperature monitoring in reducing the risk of esophageal thermal lesions during pulmonary vein isolation for AF has not been established, and more studies including randomized controlled trials are needed to assess its true impact.
Correspondence to: Jie Cheng, MD, PhD; Texas Heart Institute, Electrophysiology Research Lab, 6770 Bertner Avenue, Houston, TX 77030;
Atrial fibrillation (AF) is the most common cardiac arrhythmia, affecting millions of people around the world. In addition, AF has a significant health, economic, and social impact. Because of technological advances and improved operator experience, radiofrequency ablation for rhythm control of AF has become increasingly common. The efficacy of pulmonary vein isolation using radiofrequency ablation has been well established, but major complications have been reported in 4.5% of patients.[1] Although its incidence is low (0.03-0.1%), atrio-esophageal (AE) fistula is a devastating complication with a high mortality.[2]-[4] The precursor for AE fistula formation is thought to be thermal esophageal injury during radiofrequency ablation, given the proximity of the anterior esophageal wall to the posterior left atrial wall. Most AE fistulas manifest 2-6 weeks after an ablation procedure, suggesting that direct mechanical trauma during the procedure is not likely the sole mechanism underlying this complication.[5],[6]
The incidence of esophageal lesions during radiofrequency ablation has been reported as 2-47%.[7]-[11] Various techniques have been examined to reduce the risk of esophageal injury during radiofrequency ablation. These include imaging the esophagus during ablation, limiting energy delivery on the posterior left atrial wall, using mechanical deflection of the esophagus during catheter ablation, insulating the esophagus from thermal injury, and monitoring luminal esophageal temperature (LET) during the procedure.[6],[9],[12]-[17] All reports on esophageal temperature monitoring during AF ablation are from single-center studies with small sample sizes. The aim of this meta-analysis is therefore to evaluate the role of luminal esophageal temperature monitoring in preventing thermal esophageal injury on the basis of pooled data available in the literature.
We searched the PubMed, Scopus, Cochrane, Embase, and Refworks databases for studies published from January 2004 to June 2016 that compared radiofrequency ablation for AF with and without LET monitoring. We searched the title field for terms esophageal temperature monitoring, AF, radiofrequency ablation, AE fistula, and thermal esophageal injury. We included only studies in which esophagogastroduodenoscopy (EGD) was performed within 72 hours after the ablation procedures with thermal esophageal injury as the primary endpoint. Meta-analysis was performed by using Review Manager (RevMan) [Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014]. Fixed-effects modeling was primarily used to conduct the outcomes meta-analysis from the included studies. The pooled incidence rates of thermal esophageal injury for patients in the esophageal temperature monitoring arm and in the no esophageal temperature monitoring arm were derived from the studies that we identified as meeting our criteria. The pooled odds ratios were then calculated for the comparisons. Because of the significant heterogeneity among the studies, we conducted a meta-regression analysis to determine the differences in the incidence of esophageal lesions using 2 different strategies after adjusting for age and sex. The meta-analysis has been reported in accordance with the Observational Studies in Epidemiology Guidelines.[18]
Our search resulted in the identification of 4 non-randomized controlled trials that met our search criteria [Table 1].[10],[19]-[21] In the first study published in 2008, Singh et al[21] retrospectively analyzed 81 consecutive patients who had undergone AF ablation followed by EGD and compared the LET vs no LET groups. They noted a significantly higher frequency of esophageal injury in patients who had not undergone LET monitoring during ablation.
Table 1. Esophageal thermal injury during radiofrequency ablation of AF with and without LET monitoring
|
Study
|
LET monitoring
|
No LET monitoring
|
Weight
|
Odds ratio
|
95% CI
|
|
Injury
|
Total
|
Injury
|
Total
|
|
Singh 2008(21)
|
n=4
|
67
|
n=5
|
14
|
36.60%
|
0.11
|
(0.03, 0.51)
|
|
Deneke 2011(19)
|
n=5
|
48
|
n=0
|
42
|
9.50%
|
10.75
|
(0.58, 200.42)
|
|
Muller 2015(20)
|
n=12
|
40
|
n=1
|
40
|
18.40%
|
16.71
|
(2.05,136.08)
|
|
Kiuchi 2016(10)
|
n=0
|
80
|
n=6
|
80
|
13.1%
|
0.07
|
(0.00,1.29)
|
|
|
|
|
|
|
|
|
|
|
Total events
|
21
|
12
|
|
|
|
|
Total (95% CI)
|
235
|
176
|
100%
|
0.66
|
(0.23, 1.89)
|
LET: Luminal esophageal temperature. CI: confidence interval.Test for overall effect: Z=0.77 (P=0.44).Heterogeneity: Chi2 = 20.22, df = 3 (P<0.0002), I2=85%.
Subsequently in 2011, Deneke et al[19] reported a higher incidence of esophageal injury in patients who underwent LET monitoring than in those who did not undergo LET monitoring during AF ablation. This study included 90 patients. These results were consistent with those reported by Muller et al[20] in 2015 who evaluated 80 patients who underwent AF ablation. They noted a significantly higher incidence of esophageal injury in the LET monitoring group. In 2016, Kiuchi et al[10] retrospectively analyzed 160 patients who underwent AF ablation with or without LET monitoring. They reported a significantly lower incidence of esophageal injury in the LET monitoring group. We have reported the ablation parameters and the esophageal temperature probes used in these four studies in [Table 2].
Table 2. Ablation parameters used in the four studies included in our meta-analysis
| Study |
Ablation catheter |
Ablation parameters
(power and temperature) |
Esophageal probe |
Maximal LET |
| Singh et al21 |
3.5 mm external or 4 mm internal irrigated catheter |
35W and 40°C |
n/a |
38.5°C |
| Muller et al20 |
Irrigated catheter (Size not specified) |
35W (25W at posterior wall), 43°C |
Sensitherm, 5 electrodes |
39.5°C |
| Deneke et al19 |
Multi-channel RF system |
10W, 60°C |
Esotherm, 3 electrodes |
40°C |
| Kiuchi et al10 |
Irrigated catheter |
30W (20W for post), 43°C |
Sensitherm, 5 electrodes |
39°C |
LET: Luminal esophageal temperature. RF: radiofrequency. W: watts.
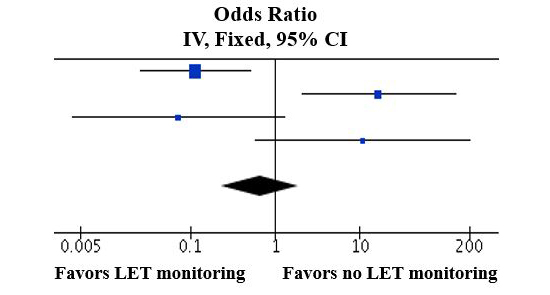
The total number of patients included in our analysis was 411. Of these, 235 patients underwent LET monitoring and 176 did not undergo LET monitoring during radiofrequency ablation of AF. All patients underwent EGD to determine the presence of post-ablation esophageal thermal injury, which was defined as the primary endpoint. Thermal esophageal injury was seen in a total of 21 (9%) patients in the LET monitoring group and 12 (7%) patients in the no LET monitoring group. In a meta-analysis of these 4 studies, a fixed-effects model showed that the pooled odds ratio was 0.66(confidence interval, 0.23-1.89) [Figure 1]. The Z score was 0.77 (P value = 0.44) that failed to reach statistically significant difference between the two groups with regard to thermal esophageal injury. We observed significant heterogeneity because of the small sample size and non-randomized nature of the studies. In the meta-regression analysis in which the data were adjusted for age and sex, there was no significant difference in outcomes of esophageal thermal injury between the two groups.
Figure 1. Pooled odds ratio after meta-analysis using a fixed-effects model. There is no significant difference between the incidence of esophageal injury between LET monitoring and no LET monitoring groups. Odds Ratio – 0.66, 95% CI (0.23, 1.89).
LET monitoring during left atrial radiofrequency ablation for AF is frequently used to try to minimize excessive esophageal thermal injury, thereby reducing the risk of developing AE fistula. Here, we present the first meta-analysis of studies evaluating LET monitoring during AF ablation. Our findings indicate that there is no conclusive evidence at this point supporting the use of esophageal temperature monitoring in prevention of esophageal mucosal injury during radiofrequency ablation of AF.
The close proximity of the esophagus to the posterior left atrial wall is one of the most important factors contributing to esophageal mucosal injury during AF ablation.[22]-[24] Thermal injury is thought to affect the microvasculature of esophageal tissue leading to ischemic necrosis of the mucosal layers.[6] Multiple studies have reported esophageal thermal injury after AF ablation. Redfearn et al[25] and Perzanowski et al[26] reported that real-time monitoring of esophageal luminal temperature during AF ablation was feasible and could be used to detect esophageal heating. They also suggested luminal esophageal temperature monitoring as a means of reducing esophageal injury. Maximal LET of 40°C-41°C has been shown to be directly associated with an increase in the incidence of esophageal lesions.[8],[16] Halm et al[8] have demonstrated significantly increased odds of esophageal injury for every 1°C rise in LET. Singh et al[21] were the first to report a reduction in the incidence of esophageal injury with the use of esophageal temperature monitoring during AF ablation.
However, various limitations of LET monitoring have been recognized. Deneke et al[19] and Muller et al[20] have suggested that esophageal temperature monitoring may increase the risk of esophageal mucosal injury. The proposed underlying mechanism is that the esophageal temperature probe itself may act as a conductor for the transfer of heat energy to the esophagus, thereby increasing the thermal injury risk. However, in a simulation study, Perez et al[27] showed that the temperature increase in the esophagus is due primarily to thermal conduction only and that electrical conduction between the ablation catheter and the esophageal probe does not play a significant role.
One of the major limitations of LET monitoring is the underestimation of temperature of esophageal intramural tissue.[28] Because the direct monitoring of esophageal intramural tissue temperature is not currently feasible, luminal temperature monitoring is the best strategy available. The major drawback of LET monitoring is that it does not accurately reflect the esophageal intramural tissue temperature because of the variable and unpredictable distance between the temperature probe and the anterior wall of the esophagus. In addition, the physical composition and dimensions of the tissue between the posterior left atrium and the esophagus vary significantly among individual patients. Furthermore, the safe maximal LET and critical temperature rise from the standpoint of esophageal injury remain to be established. Another major limitation to the monitoring of esophageal temperature is the variability among different thermistor probes. Recently, investigators reported a significant difference in thermodynamics with the use of two different esophageal probes in both experimental and clinical settings.[29] All of these factors may limit the ability of LET monitoring to accurately predict esophageal damage during ablation. In addition, given the extremely low incidence of AE fistula, esophageal thermal injury has been used as a surrogate marker to predict the risk of fistula formation in all major studies. Our understanding of the evolution of AE fistula from esophageal thermal injury remains incomplete.
Our study has limitations. The non-randomized nature of the studies in our meta-analysis as well as the small number of studies/patients available limit our findings and indicate the need for a large-scale, randomized multicenter trial. Another limitation of our analysis was the significant heterogeneity noted among the studies. The ablation parameters and the esophageal temperature probes used in the four studies varied (Table 2). In addition, we examined only the use of esophageal temperature monitoring in preventing esophageal mucosal injury. Other approaches such as limiting the power and duration of the delivery of radiofrequency energy at the posterior left atrial wall, using a deflectable esophageal probe or previous esophageal imaging, and insulating the esophagus were not evaluated in this meta-analysis, which could have affected the incidence of thermal esophageal injury in these studies.
Use of esophageal temperature monitoring during cryoballoon ablation for atrial fibrillation
When approved initially by FDA, the risk of esophageal injury with cryoballoon (Medtronic, Inc.) ablation of atrial fibrillation was perceived to be minimal. However, atrio-esophageal fistulas have been reported with both first generation and second generation cryoballoons[32]-[33]. Risk of thermal esophageal injury during cryoballoon ablation has been reported to be 2% to 19% depending on the lower esophageal temperature cut-offs used [34]-[36]. While the risk of esophageal injury increases at temperatures below 30 C, an esophageal cut-off temperature of 10-120 C has been suggested, given the progressive decline in temperature after cessation of ablation[35]-[36]. Furkranz et al demonstrated a reduction in esophageal injury from 18.8% to 3.2% by use of LET guided cryoballoon ablation[34]. Based on current evidence available, it seems vital to use LET monitoring for assessing esophageal cooling than relying primarily on cryoballoon temperatures.
Accurate esophageal wall temperature monitoring probes are currently being studied and will aid in the real-time identification of early esophageal heating, which will help reduce the risk of esophageal thermal injury. Safe retraction of the esophagus away from the ablation plane by using mechanical probes such as EsoSure (Northeast Scientific Inc., Boynton Beach, Florida) is also under evaluation.
Capsule endoscopy is a reliable tool for detecting esophageal injury after AF ablation without the risk of insufflation with EGD.[7] Recent data also suggests that esophageal injury from radiofrequency ablation is not limited to mechanical damage but also involves esophageal dysmotility.[30] Incorporation of improved tools such as capsule endoscopy and assessment of both mechanical and functional esophageal injury will help design better trials, thereby lowering the overall risk of esophageal injury.
In this first meta-analysis of studies evaluating LET monitoring during AF ablation, we found that the evidence from non-randomized clinical trials supporting its role in preventing esophageal mucosal lesions is far from conclusive. Randomized controlled trials are necessary to evaluate the true impact of LET monitoring. Furthermore, advances in the technology for temperature monitoring and diverting the esophagus further away from the ablation site may improve our strategies for avoiding esophageal thermal injury.






