PACEMAKER IMPLANTATION IN ELDERLY PATIENTS: SAFETY OF VARIOUS REGIMENS OF ANTICOAGULANT THERAPY
Denis Terekhov1, Valeriy Agapov1, Kirill Kulikov1, Svetlana Zadorozhnaya1, Vasiliy Samitin1, Vladimir Maslyakov2
1Saratov Regional Cardiac Centre; Krymskaya ulitsa, 15, Saratov, 410039, Russian Federation.2Saratov Medical Institute “REAVIZ”; ulitsa Verkhny Rynok, 10, Saratov, 410004, Russian Federation.
To study incidence of hemorrhagic complications after pacemaker implantation in elderly patients receiving antithrombotic therapy with warfarin or uninterrupted dabigatran.
126 patients aged 83 [82; 85] years who receive continuous antithrombotic therapy after pacemaker implantation, were enrolled in the study. Adverse event data were collected during hospitalization and further 12 weeks.
95 subjects (75.4%) from general number of enrolled patients received elective anticoagulant warfarin therapy and 31 subjects (24.6%) were treated with dabigatran. All patients of dabigatran group received 220 mg/day skipping the last dose before a surgery and resumed the drug intake in 36-48 hours after it. Patients of warfarin group underwent surgery if INR was NMT 3; they didn't stop taking the drug for the duration of operation.
No statistically significant differences of hematoma incidence were detected in dabigatran (incidence is 0.065, 95%CI (-0.02–0.15)) and warfarin (incidence is 0.05, 95%CI (0.006–0.01)) groups, p(Fisher)= 0.55. Three cases of nonfatal gastrointestinal bleeding (warfarin group) and 1 similar event in dabigatran group were detected during a follow-up (12 [6; 20] weeks): RR= 0.98 (warfarin group), p(Fisher)=0.68. No statistically significant difference of age, sex composition, history of IHD and diabetes was detected between groups by comparison of individual characteristics of patients whose surgeries were complicated/non-complicated by hematoma formation. Upon that, hematoma formation rate was significantly higher in patients with adjunctive pacemaker muscular fixation: 71.4% vs 31.9% (patients without hematomas), p(Fisher)= 0.045.
Incidence of hematoma formation after pacemaker implantation in patients > 75 years receiving warfarin or dabigatran, is the same as in general population of patients treated with anticoagulants. Adjunctive pacemaker muscular fixation is a significant risk factor of hematoma formation.
Key Words : pacemaker, complications, hematomas, dabigatran, warfarin.
Correspondence to: Corresponding author: Denis Terekhov, Krymskaya ulitsa, 15, Saratov, 410039, Russian Federation, tel. +79276209757, e-mail: den_ter@list.ru
Permanent pacemaker implantation is the most common procedure of cardiovascular surgery. In the setting of increase in life expectancy and implementation of ambitious medical care programs, there is a growth of both total number of pacemaker implantations (for example, according to Mond et al. [2], 590 procedures per 1 million of population are performed in Australia and results of other studies are the same – [3]) and number of procedures in elderly patients: 70-80% of pacemaker implantations in patients > 65 years [4] and to 32% in patients > 80 years in several populations - [5], [6], [7]. In spite of reports about relative safety of such interventions in elderly patients [8], many specialists consider this group as one with increased risk of periprocedural complications in routine clinical practice. The latter is particularly true concerning patients receiving continuous antithrombotic therapy. This number increases during last few years because elderly age is not only a risk factor of atrial fibrillation but an independent predictor of thromboembolic events [9].
Pacemaker pocket hematoma is one of the most common postsurgical complications whose incidence is 0.6-2.0% according to most of sources [10], [11], [12], [13], [14]. At the same time, according to the one of recent reports related to pacemaker implantation in New South Wales [14], total incidence of complications is 11.9%. Lead dislodgement and postsurgical hematomas are the bulk of it. At that, there are only several available studies particularly evaluating clinical factors causing pacemaker pocket hematomas in elderly patients [9], [15], [16].
Due to this fact, the objective of this study is to investigate incidence and possible predictors of pocket hematoma formation after pacemaker implantation in elderly patients receiving antithrombotic therapy with warfarin or uninterrupted dabigatran.
Patients > 75 years receiving continuous antithrombotic therapy (CHA2DS2-VASc score >2) were enrolled in the concentriс prospective non-randomized study. They have undergone primary pacemaker implantation in Saratov Regional Cardiology Health Center since January, 2013 till February, 2015. Patients, who had undergone immediate pacemaker implantations, and ones with prior elective interventions were included in this study. Indications for pacemaker implantation: II and III grades of AV-block associated with symptoms, sick sinus syndrome (SSS), atrial fibrillation associated with bradycardia (average heart rate < 40 beats in minute according to 24-hour monitoring). Exclusion criteria: previously implanted device required reimplantation without lead replacement, cardioverter defibrillator causing major intervention, as well as high risk of bleeding (HAS-BLED score >3) resulting in contraindications for elective antithrombotic therapy of atrial fibrillation. Adverse event data were collected during hospitalization and further follow-up period (12 weeks).
All pacemakers were implanted by cardiac surgeons who carried out not less than 100 similar procedures in angiographic operating rooms last year. The type of pacemaker to be implanted was selected according to bradyarrhythmia type, patient's age, physical status and comorbidity. Local or general anesthesia was selected in virtue of operating surgeon's preference. All patients received preventive antibiotic therapy before a surgery and in 2 days after it. V. cephalica was commonly used for venous access. In case of technical difficulties, subclavian vein puncture was carried out. Correct positioning of implanted leads after implantation was confirmed by intracardial cardiograms (endograms), pacing threshold analysis and radiographs of thoracic organs. Cardiac pacing conditions were reported in dismissal and a follow-up was prescribed in 4-6 weeks after it. Besides, additive phone contacts were performed.
Incidence of pocket hematoma formation within 6 weeks after pacemaker implantation was evaluated as a primary endpoint. Hematoma was diagnosed due to opinion of the surgeon (who had implanted a device) confirmed by ultrasonographic data. During further analysis hematomas were divided depending on need for drainage. Type of received anticoagulant and antithrombotic therapy, as well as their potential interaction with hematoma development were considered. According to international practice [13], [14], other postsurgical complications were evaluated as secondary endpoints, such as: cardiac stimulant system infections, lead dislodgement, pneumothorax, myocardial rupture, life-threatening arrhythmias (resuscitation is required) and death.
Data are presented as frequency (categorical variables), medians and interquartile interval (quantitative variables). Differences of proportions were analyzed with chi-square method or Fisher exact test. Continuous quantitative variables were analyzed with Mann-Whitney test. Statistic analysis was carried out in Statistica 10 (StatSoft, Inc, 2011) application software package. In order to review statistical hypotheses, critical significance level was set to 0.05%. Diagram was formed using MedCalc 12.5.0.0 (MedCalc Software bvba, 2013).
During the specified period pacemaker implantations were performed in 126 patients (48 men and 78 women) > 75 years receiving elective antithrombotic therapy due to permanent or persistent atrial fibrillation. Data of follow-up or phone contacts with patients (or their relatives) were received for all enrolled subjects. At the time of surgery average age of patients was 83 [82; 85] years; the maximum age in observed cohort was 93 years. The most common indication for pacemaker implantation was high grade AV-block (68 cases, 54.0%), atrial fibrillation with slow ventricular rate (29 cases, 23.0%) and SSS (29 cases, 23.0%) were rather rare ones. Cardiac pacing was performed in DDD(R) and VVI(R) modes in 21 (16.7%) and 105 (83.3%) cases, respectively. Forty six percent of surgeries were immediate or urgent (in case of syncopal conditions).
Ninety five (75.4%) of total number of enrolled subjects received elective anticoagulant warfarin therapy and 31 patients (24.6%) used dabigatran. Subgroup data had no significant differences of basic characteristics ([Table 1]). Duration of antithrombotic therapy course was 14 days at least before a surgery in all patients.
Table 1. Antithrombotic therapy type-based characteristics of patient subgroups
|
Characteristic
|
Warfarin group, n= 95
|
Dabigatran group, n= 31
|
p
|
|
Age (years)
|
83 [82; 85]
|
83 [81; 85]
|
0.063 (U)
|
|
Men
|
40
|
8
|
0.55 (c2)
|
|
CHA2DS2-VASc
|
4 [3; 5]
|
4 [4; 4]
|
0.57 (U)
|
|
HAS-BLED
|
2 [2; 3]
|
2 [2; 3]
|
0.3 (U)
|
|
INR before implantation
|
2.7 [2.2; 3.2]
|
2.8 [2.0; 3.6]
|
0.8 (U)
|
|
Implantation duration (min)
|
77 [65; 85]
|
84 [70; 90]
|
0.057 (U)
|
|
Access via v. subclavia
|
76 (80%)
|
26 (84%)
|
0.6 (z)
|
|
Average number of leads per patient
|
1.2
|
1.1
|
0.8 (U)
|
|
Antiplatelet therapy
|
19
|
5
|
0.63 (c2 Pearson)
|
All patients of dabigatran group received 220 mg/day skipping the last dose before a surgery (withdrawal interval was 12 hours). After a surgery interval before the first dabigatran intake was defined at operating surgeon's discretion (36-48 hours). In order to confirm INR value < 3, morning presurgical and postsurgical INR monitoring was performed in patients received antithrombotic warfarin therapy. In case of greater values, surgery may be delayed in the setting of short-term warfarin withdrawal until target INR value is obtained. Wafrarin intake wasn't stopped for the duration of surgery. Patients took usual drug dose of the drug after the implantation.
No serious hemorrhagic (such as profuse bleeding, hemothorax, hemopericardium, gastrointestinal bleeding) or thromboembolic (ishemic stroke, deep venous thrombosis of lower limbs, pulmonary artery thromboembolia) complications were detected during initial hospitalization.
Subcutaneous hematomas developed in 2 patients of dabigatran group (incidence is 0.065, 95%CI (-0.02–0.15)) and 5 patients treated with warfarin (incidence is 0.05, 95%CI (0.006–0.01)). Differences of incidence between two groups were not statistically significant – p(Fisher)= 0.55. Moreover, the only one patient (warfarin group) had a hematoma with a need for drainage. Hematoma formation was associated with target INR level defined before a surgery in all patients received warfarin. In all cases of hematoma formation this complication developed within 12-24 hours after a surgery. It was primary, i.e. it was not a result of lead positioning correction or local infectious process required antibiotic therapy. In case of developed hematomas, reinitiation of antithrombotic therapy was delayed for 1-3 days till confirmation of dimensional stability according to repeated ultrasonic examination. No complications caused by hematoma formation were detected in future (including contamination, lead dislocation or capture failure, pneumothorax and thrombembolia). In the single case required drainage repeated hematoma formation was not detected.
During follow-up (12 [6; 20] weeks) 3 cases of nonfatal gastrointestinal bleeding (warfarin group) and 1 similar event in dabigatran group were recorded; RR= 0.98 (warfarin group), p(Fisher)= 0.68 (see [Figure 1]).
Figure 1. Relative risk of basic events for warfarin and dabigatran groups
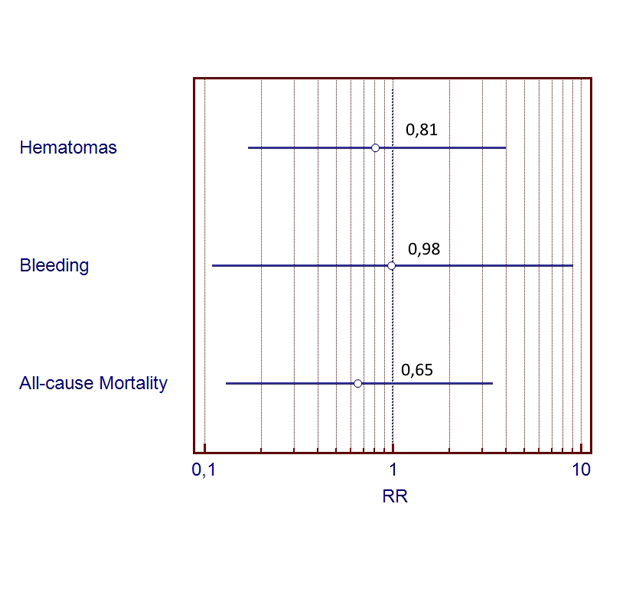
No fatal cases related to hemorrhagic or thromboembolic events were detected during follow-up period. Two (warfarin group) and 1 (dabigatran group) fatal cases occurred as a result of IHD. There were no statistically significant differences of lethality rate between two groups (р(Fisher)= 0.72).
No statistically significant difference of age, sex composition, history of IHD and diabetes was detected between groups by comparison of individual characteristics of patients whose surgeries were complicated/non-complicated by hematoma formation. Upon that, hematoma formation rate was significantly higher in patients with adjunctive pacemaker muscular fixation: 71.4% vs 31.9% (patients without hematomas), p(Fisher)= 0.045, see [Table 2].
Table 2. Possible predictors of hematoma formation
|
Characteristic
|
Patients with hematomas,
n= 7
|
Patients without hematomas,
n= 119
|
p(Fisher)
|
|
Urgent intervention
|
4 (57.1%)
|
44 (36.9%)
|
0.248
|
|
Elective intervention
|
3 (42.9%)
|
75 (63.1%)
|
|
Number of DDD(R) devices
|
3 (42.9%)
|
18 (15.1%)
|
0.09
|
|
Number of VVI(R) devices
|
4 (57.1%)
|
101 (84.9%)
|
|
Pacemaker muscular fixation
|
5 (71.4%)
|
38 (31.9%)
|
0.045
|
Pacemaker implantation is a common life-saving procedure which is, however, associated with defined risk of postsurgical complications. One of stages of the surgery is a pacemaker pocket formation, when surrounding tissues are prepared without ligation. It may cause poor hemostasis [17]. As a result, formed hematoma is uncomfortable for a patient increasing risk of contamination and lengthening postsurgical hospital period.
Actually, about 1 million of pacemakers are annually implanted worldwide and this number even grows every year. In 2011 a total 32 317 antiarrythmic devices were implanted in the Russian Federation but number of implantations annually increases by 8-10% [1] at average. In spite of lead dislodgement, pocket hematoma formation (including ones required operative exploration) is one of the most common complications after pacemaker implantation. However, confident quantitative evaluation of this complication incidence is difficult in Russian population because individual statistic recording related to the procedure complications is required in the Russian Federation. Due to this fact, we selected information from documents (a report of Australian interventional arrhythmological center activities) including record of corresponding complications in population in order to perform a comparative study. In 2005 a total 11 850 pacemakers were implanted in Australia [2]. Reported data related to prevalence rate of pacemaker implantation complications showed 11.9% (total incidence), 2.6 % of which was hematoma formation [18]. This pattern is comparable to major international register data (total incidence of complications is 4.5 - 10.1%, 0.6-1.9% of which is hematoma rate [10], [11], [12], [13]). According to our data, incidence of pacemaker pocket hematomas is 5.0-6.5% in patient subgroups receiving various antithrombotic therapy which is significantly consistent with reported information.
Potential causes of slightly higher incidence of hematoma formation in our study cohort may be related to enrolling of elderly patients receiving anticoagulant therapy and immediate or urgent performance of essential part of implantations. Thus, according to Link et al. [19], incidence of complications after two-chamber pacemaker implantation in patients > 65 years was 6.1%, 4.4% of which required reintervention. As follows from this work [16], incidence of hematomas in elderly patients was 4.9% with any antithrombotic therapy during perisurgical period as a main risk factor of this complication. However, a material constraint of this study [16] is a fact that 41% of patients received warfarin before a surgery were transferred into temporary anticoagulant therapy (so-called ''bridging therapy''). It can be an independent risk factor of postsurgical complications related to blood-clotting disorders [20], [21], [22]. Thus, Chow et al. [16] mentioned that postsurgical hematomas formed in patients received anticoagulants only in cases of temporary anticoagulant therapy (21 vs 0); as a whole, hematomas formed in 65.6% of 32 patients who have administered excitatory amino acid. Besides that, according to Chow et al. [16], influence of anticoagulant therapy on hematoma formation depends on degree of intervention urgency; immediate procedures duplicate this risk. Although authors withheld representation of this observation, we can suggest that urgent intervention complicates adequate control in case of prescribing of temporary ''short-term'' anticoagulant during presurgical period. Such a theory is indirectly confirmed by the fact that no statistically significant influence of intervention urgency on hematoma development risk was obtained in the frame of our study (without included regimen of temporary anticoagulant therapy).
The fact of additional interest is that antiplatelet therapy (used in 19.8% subjects of our study) was not a predictor of hematoma formation. It is a promising factor for patients with coronary blood flow disorders (including ones with implanted coronary stents). In this case withdrawal of antiplatelet drugs may be associated with increased risk of corоnary thrombosis.
According to reported data [19], [23], [24], higher incidence of pneumothorax is observed due to pacemaker implantation in elderly patients vs. younger ones along with similar incidence of other complications. Additional risk factors of this complications were female sex, lower body weight, lower Karnofsky score and higher Carlson score [24], [25], [26]. Karnofsky Performance Scale displays degree of patient's activity naturally decreasing with age. Furthermore, low body weight and kyphosis (which are common in elderly patients) can cause higher incidence of this complication.
Hypertension does not significantly influence on incidence of complications after device implantation because interventions are carried out via venous access.
Armaganijan et al. [25] highlighted relatively higher incidence of early complications (such as lead dislodgement, capture failure, myocardial rupture, infection) along with similar incidence of late ones (lead integrity violation) in elderly patients. However, according to later large study [26], absolute number of complications were rather small (even in patients > 80 years). Comorbidity was a predictor but not patient's age.
Present study was not a randomized and has a relatively small sample size, which can lead to absence of difference in study endpoints due to lack of statistical power. Furthermore, the small number of events did not allowed to perform multivariate analysis to identify independent predictors of hematoma formation. However, our data is consistent with other studies which did not demonstrate the increased hematoma frequency after device implantation in senior patients receiving uninterrupted dabigatran [27].
This study demonstrated relatively small total incidence of complications and incidence of hematoma formation after pacemaker implantation in patients older than 75 years receiving elective anticoagulant therapy (continuous warfarin or dabigatran intake). Adjunctive pacemaker muscular fixation was found to be a risk factor of hematoma formation.






