Comparison of the efficancy and complication rates of the hybrid maze, complete Cox-maze and catheter ablation in the treatment of atrial fibrillation
Usama Boles1, Enes E Gul1, Andres Enriquez1, Howard Lee1, Dave Riegert2, Adrian Andres1, Adrian Baranchuk1, Damian Redfearn1, Benedict Glover1, Chris Simpson1, Hoshiar Abdollah1, Kevin Michael1
1Division of Cardiology, Heart Rhythm Service, Kingston General Hospital, Queen‟s University, Kingston, Ontario, Canada..2Department of Mathematics and Statistics , Queen's University, Kingston, Ontario, Canada..
Atrial fibrillation is the most common cardiac arrhythmia in the United States. It has been associated with a reduction in patient quality of life and more serious complications such as stroke and heart failure. The aim of this study was to compare the efficacy of commonly performed invasive procedures in keeping patients in normal sinus rhythm.
A retrospective chart review was performed on all patients who underwent primary radiofrequency catheter ablation, the complete Cox-maze, or the hybrid maze at OSF Saint Anthony Medical Center between January 2010 and December 2013 (n=140). Immediately post-procedure, arrhythmia recurrence rates did not differ between the groups (p = 0.28). At all follow-up points thereafter, however, differences in procedural efficacy between surgical and catheter therapy remained highly significant (p < 0.001). At 2 years, 20.3% of the catheter ablation patients were in normal sinus rhythm, when compared to 57.9% of hybrid maze and 72.7% the complete Cox-maze groups. A difference in major complication rates was noted (p = 0.04), with the complete Cox-maze having a 17.4%, the hybrid having 22.7%, and the catheter ablation group having 5.6%.
This study was unable to detect differences in the efficacy rates of the surgical procedures, however they were both superior to catheter ablation. Although the hybrid approach is considered minimally invasive, complication rates were similar to those of the complete Cox-maze. Catheter ablation was the safest procedure, and since evidence of reduced mortality after the use of aggressive rhythm therapy is currently lacking, the results suggest that hybrid surgery for atrial fibrillation should be used after the failure of more conservative measures.
Key Words : Atrial Fibrillation, Hybrid Maze, Cox Maze, PVI Catheter Ablation.
Correspondence to: Ivo K. Genev, B.S. University of Illinois College of Medicine at Rockford 1601 Parkview Avenue Rockford, Illinois 61107 Email: igenev2@uic.edu
As the most commonly encountered cardiac arrhythmia in the United States, atrial fibrillation is currently estimated to affect between 2 and 2.5 million people and the number suffering might rise to approximately 5.6 million by the year 2050 [1]. Atrial fibrillation patients are at an increased risk of having a stroke, developing heart failure or other cardiovascular complications associated with marked reductions in quality of life. An analysis of patients in the original Framingham Study who suffered from atrial fibrillation noted that the condition is likely associated with a significant increase in patient mortality even after adjusting for other cardiac disease [2]. The condition is generally considered to be progressive in nature and involves four stages: paroxysmal, occurring in separate episodes; persistent, when it becomes constant; long standing persistent; and permanent, when the decision has been made to no longer pursue conversion to normal sinus rhythm (NSR). Currently, there are no curative options for patients with atrial fibrillation. In fact, the annual cost of treating patients in the United States is approximately $6.65 billion, which does not take into account additional costs incurred for stroke prevention, inpatient medications, comorbid conditions, or other inpatient expenditures [3].
Despite the profound impact on our society, the exact cause of this arrhythmia is still unknown. The pathophysiology of the disease however, depends on two major components: abnormal electrical triggers, thought to be cardiac ganglionic plexuses located at the pulmonary veins and left atrial junction, and an enlarged and often fibrotic left atrium, acting as a substrate for propagation of the abnormal signals [4]. Current invasive treatment strategies are based on these two notions and focus on the prevention of thromboembolism, which may lead to stroke or other cardio-embolic complications [5]. The condition can be asymptomatic, in which case, physicians may simply focus on anticoagulation and rate control. If symptoms are severe enough to warrant therapy, it is possible to utilize a number of antiarrhythmic medications in order to try and gain control of the abnormal rhythm. In addition to pharmacologic therapy, electrical cardioversion can be utilized to convert the patient back is also utilized with the aim of converting the patient back to normal sinus rhythm. If that fails, patients may undergo more invasive ablation therapies [6]. It is of note that the AFFIRM trial, which is a large study that compared rate versus rhythm control in the management of atrial fibrillation patients, detected no decreases in overall mortality associated with either method compared to the other [7]. Therefore, utilization of invasive approaches for rhythm management is purely for symptomatic relief with an aim of improving quality of life. Consequently, the risks of complications should carefully be weighed against the benefits of these procedures.
There are three main methods of rhythm control: medical management, catheter ablation and surgical therapy. Medical management, usually being the first-line approach, involves the use of antiarrhythmics. One of the more established invasive procedures for the treatment of recurrent symptomatic patients is radiofrequency endocardial catheter ablation, in which the pulmonary veins are electrically decoupled from the left atrium with the help of a catheter that is advanced into the left atrium usually through a vein in the groin. Epicardial ablation with left atrial appendage clipping, also known as the complete Cox-maze procedure, is the most invasive surgical approach. It is an open-heart surgery which is typically performed in conjunction with surgery to correct another heart condition like coronary artery disease or valvular disease. Studies have shown outstanding efficacy rates, but due to the invasiveness of the procedure and the potential for complications, it is not recommended for all patients[8]–[10]. Developed by Dr. James Cox in 1987 [11]–[13], the complete Cox-maze provided a basis for other currently utilized surgical procedures. The hybrid maze combines minimally invasive surgical epicardial ablation relying on a mini-thoracotomy approach and endocardial catheter ablation. The procedure can be completed in a stepwise fashion, where the patient undergoes the minimally invasive maze and then several months later, undergoes catheter ablation. Completing both stages of the procedure at one time is also possible. This therapy combines the benefit of left atrial debulking with a minimally invasive approach, which in theory would make it a preferred choice. Current data suggests that this newer hybrid procedure may be far superior in efficacy to standard endocardial catheter ablation, with studies reporting success rates greater than 90% [14].
With the utilization of newer procedures and the improvement of more established techniques, patient treatment options are expanding. Yet to our knowledge, there are currently only two studies that have compared the hybrid maze to other invasive treatment modalities, and neither has examined it in the context of primary treatment, before the failure of other invasive treatments [15],[16]. In one trial, the control was catheter ablation, however the study included only 15 patients who underwent the maze, of which less than half followed up for more than 20 months [16]. The other examined the differences in outcomes when adding a sequential catheter ‘touch up’ to a minimally invasive surgical ablation, essentially dicussing the plausability and potential benefits of utilizing the hybrid approach [15]. At this time, neither the 2016 European Society of Cardiology (ESC) nor the 2014 American Heart Association (AHA) guidelines provide any recommendation as to the proper utilization of this surgical technique, despite both of them mentioning that surgical ablation may still play a role in some more highly symptomatic patients [6],[17]. Because of ethical concerns regarding patient safety, a randomized controlled trial examining the hybrid maze as stand-alone treatment for atrial fibrillation is currently not feasible. Therefore, the aim of this retrospective study is to compare long-term efficacy and complication rates of the hybrid maze procedure to other more commonly utilized invasive procedures—radiofrequency endocardial catheter ablation and the complete Cox-maze.
All patients with atrial fibrillation who have undergone radiofrequency endocardial catheter ablation, the complete Cox-maze, or the hybrid maze at OSF Saint Anthony Medical Center, Rockford, IL between January 2010 and December 2013 were identified through the use of the respective CPT billing codes for each procedure – comprising 163 cases. The subjects were stratified into three groups based on the first invasive procedure they received for the treatment of their illness. In order to provide a fair comparison between the procedures, any patient who had received prior invasive therapy to treat their condition was excluded. This included 2 patients from the hybrid maze group, 13 patients from the PVI catheter ablation group, and 8 patients from the complete maze group. The final sample size for analysis was 140 patients.
Data were extracted by two independent researchers, cross-referenced and any inconsistencies or missing values were rechecked in the electronic medical record (EMR). The patients were followed up for two years post-procedure. Data on the CHADS2 score, atrial fibrillation status, anticoagulation use (including warfarin, rivaroxaban, apixaban, dabigatran, aspirin, clopidogrel, prasugrel), antiarrhythmic use (including amiodarone, flecainide, dronedarone, propafenone, sotalol, dofetilide, digoxin, procainamide, quinidine), major life-threatening complications and additional procedures were collected at four time points—immediately post-procedure prior to discharge from the hospital, 6 months, 12 months and 24 months post-procedure. A CHADS2 score, which ranges from 0 to 6, where a higher number is correlated with a higher estimated risk of cerebrovascular accidents, was used as a surrogate for disease severity. CHADS2 is a risk stratification schema that includes: congestive heart failure, hypertension, age (>/= 75), diabetes, and cerebrovascular accidents, including transient ischemic attacks [18].
This project was approved by the Institutional Review Boards at the University of Illinois College of Medicine at Rockford (protocol number 20150077) and OSF Saint Anthony Medical Center (protocol number #201509).
The primary outcome of the study was procedural efficacy, which was defined as absence of atrial fibrillation at four time points during the 24-month follow-up. At baseline, a one-way ANOVA was used to test for differences in mean age between the different groups and a chi-square test was used for the categorical data. Due to the small sample size within the hybrid maze procedure group, a Fisher’s exact test was used where appropriate. Both a chi-square analysis and a multivariate logistic regression were used to determine if there were an association between procedure used and recurrence of atrial fibrillation at different time points. All baseline variables that were significant (p-value < 0.05) were included in the final logistic regression analysis that examined procedural efficacy. When conducting the final regression analysis, the only dependent variable was procedural efficacy in keeping patients in normal sinus rhythm. The independent variables included were: age, obesity, antiarrhythmic usage, mitral valve disease, diabetes mellitus type II, and procedure utilized.
Baseline demographic characteristics and co-morbid conditions stratified by procedure utilized are presented in [Table 1]. The mean age of subjects within the PVI catheter ablation group was 61.4±8.5 years, 68.1±10.9 for the hybrid maze group, and 69.3±9.0 in the complete Cox-maze group. The majority of participants in the study were males, with 68.1% in the catheter ablation group and 72.7% and 69.6% in the hybrid and complete maze groups respectively.
Table 1. Baseline Patient Characteristics
|
|
PVI Catheter Ablation (n=72)
|
Hybrid Maze (n=22)
|
Complete Cox-maze (n=46)
|
|
Demographics:
|
|
|
|
|
§ Age, mean (SD)
|
61.4 (8.5)*
|
68.1 (10.9)
|
69.3 (9.0)
|
|
§ Male
|
68.1%
|
72.7%
|
69.6%
|
|
§ Female
|
31.9%
|
27.3%
|
30.4%
|
|
Comorbid Conditions:
|
|
|
|
|
§ Obesity (BMI > 30)+
|
42 (58.3%)
|
18 (81.8%)
|
22 (47.8%)
|
|
§ Mitral Valve Disease+
|
12 (16.7%)
|
8 (36.4%)
|
16 (34.8%)
|
|
§ Coronary Artery Disease
|
24 (33.3%)
|
7 (31.8%)
|
23 (50.0%)
|
|
§ Cardiomyopathy
|
4 (5.6%)
|
1 (4.5%)
|
1 (2.2%)
|
|
§ Hypertension
|
57 (79.8%)
|
19 (86.4%)
|
40 (87.0%)
|
|
§ Diabetes Mellitus Type II
|
25 (34.7%)
|
4 (18.2%)
|
22 (47.8%)
|
|
§ COPD
|
9 (12.5%)
|
1 (4.5%)
|
9 (19.6%)
|
|
§ Sleep Apnea
|
25 (34.7%)
|
8 (36.4%)
|
13 (28.3%)
|
*One-way ANOVA: age of the Catheter Ablation group differs significantly from the other two, which are similar.+Chi-squared test: there was a significant difference in the rates of obesity and mitral valve disease between procedure groups.
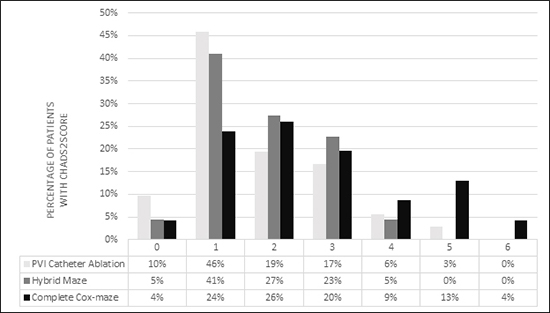
The distribution of patient CHADS2 scores can be seen in [Figure 1]. A higher percentage of patients within the complete Cox-maze were observed to have a score of 4 or above than the other two procedures, in which a greater majority of patients had a score lower than 4.
Figure 1. Percentage of Patients in each CHADS2 Score Category Stratified by Procedure
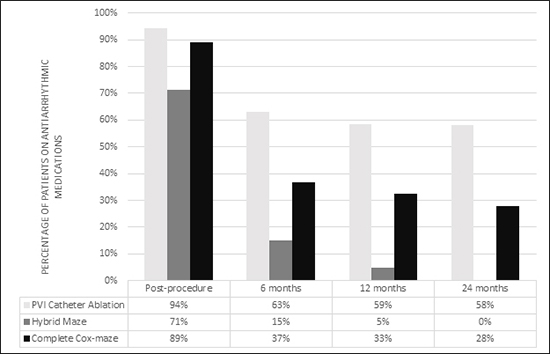
An important confounding variable is antiarrhythmic usage at different time points [Figure 2]. There was a substantial difference in medication utilization at all time points, including immediately post-procedure, with 94.4% of the catheter ablation group, 71.4% of the hybrid maze group, and 89.1% of the complete Cox-maze group taking antiarrhythmics immediately post-procedure. At 6 months, the reliance on these medications dropped to 62.9% in the PVI catheter ablation group, 15% in the hybrid maze, and 36.6% in the complete Cox-maze. By the end of the 24-month follow-up, utilization was at 58.2% in the PVI catheter ablation group, 27.8% in the complete Cox-maze, and none in the hybrid maze were utilizing rhythm control medication.
Figure 2. Usage of Antiarrhythmic Medications Stratified by Procedure Across Time Points
At that bivariate level, there was no significant relationship between any of the variables listed in [Table 1], including procedure utilized, and atrial fibrillation status immediately post-procedure. At 6 months, obesity (p-value = 0.01), diabetes (p-value = 0.01), and procedure utilized (p-value <0.01) all had a potentially significant relationship with arrhythmia recurrence. Beyond 6 months, only the procedure was associated with the patient’s atrial fibrillation status, suggesting that there was indeed statistically meaningful difference in procedural efficacy (p-values < 0.01).
Table 2. Number of Complications Associated with Each Procedure during the two-year timeline
|
Complication
|
PVI Catheter Ablation (n=72)
|
Hybrid Maze (n=22)
|
Complete Cox-maze (n=46)
|
|
Major Events:
|
|
|
|
|
· Pneumonia
|
0
|
1
|
3
|
|
· Acute Kidney Injury
|
0
|
0
|
1
|
|
· Dressler's Syndrome
|
0
|
1
|
1
|
|
· Cardioplegic Syndrome
|
0
|
0
|
1
|
|
· Pleural Effusion
|
0
|
2
|
1
|
|
· Acute Heart Failure
|
0
|
0
|
1
|
|
· Stroke/Transient Ischemic Attack (TIA)
|
0
|
0
|
0
|
|
· Pericardial Effusion/Cardiac Tamponade
|
4
|
0
|
0
|
|
· Procedure-related Death
|
0
|
1
|
0
|
|
Total number of events*
|
4 (5.6%)
|
5 (22.7%)
|
8 (17.4%)
|
|
Minor Events:
|
|
|
|
|
· Pseudoaneurysm
|
2
|
0
|
0
|
|
· Groin Hematoma/Bleed
|
2
|
0
|
0
|
*Chi-squared test: there was a significant difference in major complication rates between procedures (P-value = 0.04)
Based on the bivariate analyses, the variables age, obesity, antiarrhythmic usage, mitral valve disease, diabetes mellitus type II, and procedure utilized were all found to possess statistically significant association with presence of atrial fibrillation, therefore were all included as independent variables in the multivariate logistic regression equations. Because of well-studied differences in the rates of heart disease between men and women, the gender of the patients was also included [19],[20]. The final regression model results closely mirrored those at the bivariate level. Immediately post-procedure, there was no significant effect of any of these variables on whether or not the patient remained in normal sinus rhythm (model chi-square = 8.6, p = 0.28). The procedure utilized remained highly significant at p < 0.001 throughout all follow-up time points thereafter. At 6 months, there was also a relationship between mitral valve disease, type II diabetes, and the recurrence of arrhythmia (model chi-square = 47.0, p < 0.001), but by 24 months, only the procedure utilized was found to have a significant effect on the primary endpoint (model chi-square = 31.1, p < 0.001).
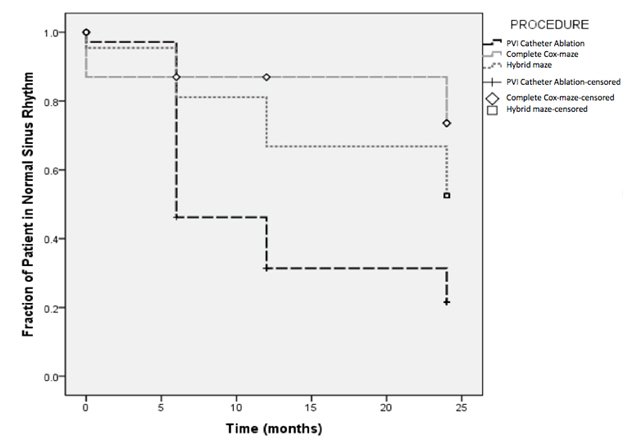
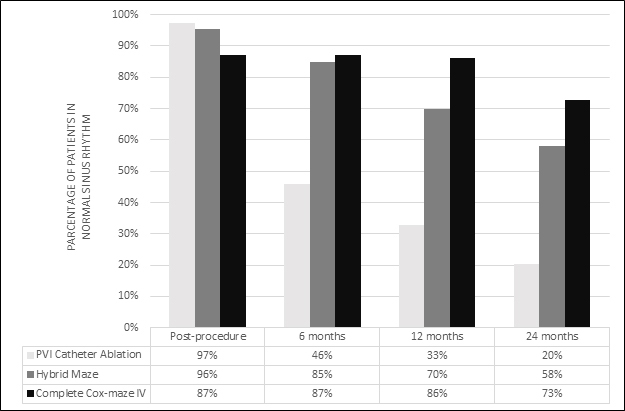
[Figure 3]and [Figure 4] illustrate differences in long-term efficacy between the three procedures. [Figure 3]depicts a Kaplan-Meier survival plot of the data, whereas [Figure 4] is a plot of the percentage of patients remaining free from atrial fibrillation at different time points, stratified based on the initial procedure utilized. At the 2-year mark, only 20.3% of the patients in the PVI catheter ablation group were in normal sinus rhythm, whereas 57.9% of patients in the hybrid maze and 72.7% within the complete Cox-maze group were atrial fibrillation free. Notably, follow-up was obtained for 105 (75%) patients at 24 months, with no significance being observed in the numbers of patients lost to follow-up between different procedures.
Figure 3. Kaplan-Meier Survival Plot for All Patients in the Study
A significant variance in major complication rates (p = 0.04) was noted between the surgical procedures and catheter ablation, with the complete Cox-maze having a 17.4% complication rate, the hybrid maze having 22.7%, and the catheter ablation group having 5.6%. Table 3 summarizes the adverse events associated with the different procedures. Within the whole cohort of subjects being followed, a single procedure-related death was observed. The patient expired during the minimally invasive thoracotomy portion of the hybrid maze procedure.
Figure 4. Percentage of Patients in Normal Sinus Rhythm at each Time Point
Indications of the complete Cox-maze have been thoroughly studied along with its excellent .long-term efficacy. However, in patients needing primary treatment solely for atrial arrhythmia, a more minimally invasive approach is preferred. Despite a clear superiority of the hybrid maze procedure when compared to pulmonary vein catheter ablation, at this time, the most appropriate indications for the procedure is yet to be identified. The current American Heart Association and European Society of Cardiology guidelines for the treatment of atrial fibrillation lack any recommendations for hybrid surgical therapy. They both do mention, however, that a standalone surgical ablation procedure can be reasonable in a symptomatic patient that is not controlled with other less invasive approaches. The ESC states that: “Although preliminary experience with hybrid simultaneous ablation shows promise, procedural time and rates of bleeding complications are higher” [17]. Therefore, the question remains whether this procedure has a role when deciding between treatment options for patients in whom medical management has failed.
Based on both the bivariate analysis and multivariate logistic regression model, it is apparent that there is a difference in atrial fibrillation recurrence at 6 months and beyond, depending on which procedure was utilized. Catheter ablation patients were much more likely to suffer from a recurrence of their atrial arrhythmia, despite the highest utilization of antiarrhythmic medication across all time points. The study was unable to demonstrate any difference between the efficacies of the hybrid maze and the complete Cox-maze, providing further evidence that the combined minimally invasive maze and catheter ablation approach might indeed be associated with favorable efficacy rates. It is important to note that the failure of this study to prove inequality between the efficacies of the hybrid maze and the complete Cox-maze does not imply equality. In a subgroup analysis of 43 patients with longstanding persistent atrial fibrillation, the results mimicked the overall cohort, with the catheter ablation procedure having an even lower efficacy when compared to the other two procedures.
Despite its promising efficacy rate, the hybrid maze procedure was associated with a significant number of complications and a possible increase in mortality. Pneumonia, Dressler’s syndrome, pleural effusion, and one death were observed. In the complete Cox-maze group, acute renal failure was most common, but pleural effusion, respiratory failure, aspiration pneumonia, heart failure and Dressler’s syndrome were all recorded complications. It is important to note that most complications encountered with both of the surgical treatments happened during patient recovery, and not at the time of the procedure. As catheter ablation procedures do not require long term hospitalization, patients are not as susceptible to hospital-associated adverse events. The majority of catheter ablation complications did not require any significant intervention from a physician, when compared to the other two procedures, which tended to require the involvement of a team of treating physicians in order to prevent long-term consequences or death. The most commonly encountered complication in the catheter ablation group was a pericardial effusion.
At this time, it is precisely because of the high complication rates associated with surgical procedures that they are utilized as a third-line treatment, only after the failure of both medical management and catheter ablation [6],[17],[21],[22]. The FAST trial, which current guidelines are mainly based on, is the largest randomized control trial comparing minimally invasive surgical ablation and catheter ablation. It was performed by Boersma et al. in two centers, one being in Spain and the other in the Netherlands. Unfortunately, this study did not evaluate the hybrid maze, therefore surgical patients were not followed-up with a catheter procedure. Also, the patients being examined had either left atrial dilitation and hypertension or a failed prior catheter abltation, suggesting a population that is inherently resistant to treatment. Despite these differences, both complication rates (5.6% vs 3.2% in the catheter ablation group and 22.7% vs 23.0% in the minimally invasive surgical group) and efficacy rates (33.0% vs 36.5% in the catheter ablation group and 70.0% vs 65.6% in the minimally invasive surgical group) at 12 months in this study were found to be similar to those of the FAST trial, suggesting that the hybrid maze may be considered a viable option in highly symptomatic patients that have failed medical therapy [21].
There are several notable limitations to this study. Due to it being a single center retrospective analysis of electronic medical records, there is an inherent reliance on the accuracy of the records. As a result of the retrospective nature of the study, there is no way to accurately measure if the patients actually experienced any improvement of their atrial fibrillation symptoms following a procedure. Instead, the success of a procedure is based on the complete lack of recurrence of the arrhythmia. Also, because of the lack of randomization, there is no way to account for effects of other variables that were not measured at baseline. Lastly, like many other studies in this field, due to the limited utilization of surgical ablation procedures, there is a limited cohort size. Thus, as mentioned previously, the study was underpowered, and its inability to identify a difference in the efficacies of the Cox-maze IV and the hybrid maze does not imply their equality. Adequately powered studies in patients with symptomatic longstanding persistent atrial fibrillation are still necessary to investigate whether the superior efficacy observed with surgical procedures might in fact outweigh the risk of procedural complications and ultimately provide some benefit in mortality.
This study was unable to detect any differences in efficacies of the two surgical procedures under investigation, however they were both found to be significantly superior to a pulmonary vein isolation catheter ablation in keeping patients in normal sinus rhythm. Although the hybrid approach utilized a minimally invasive method of gaining access to the left atrium, adverse event rates were similar to those of the complete Cox-maze. Catheter ablation had a significantly lower efficacy when compared to the surgical procedures, with most arrhythmia recurrences occurring within the first 6 months post-procedure. However, it was associated with the fewest number of potentially life threatening adverse events. Since, at this time, evidence of any long-term survival advantage after the use of aggressive rhythm therapy is lacking, the results of this study suggest that stand-alone surgical treatments for atrial fibrillation should be used as a third-line approach, only after the failure of more conservative measures. It is important to note that patients with longstanding persistent atrial fibrillation may often suffer from a substantially increased burden of disease. There is a lack of data regarding the proper utilization of the hybrid maze procedure in the treatment of this population and therefore further studies with a primary focus on these patients are necessary.






