Pulmonary vein isolation (PVI) by a single-tip radiofrequency (RF) ablation catheter, the cornerstone of catheter ablation for atrial fibrillation (AF), remains a complex and time-consuming procedure. This point-by-point ablation technique requires extensive operator experience for efficiency and safety, and is usually associated with long procedure times, especially in centers with limited experience.
Novel AF ablation techniques (‘single shot devices’) have emerged in recent years with the intention to simplify PVI procedures, to shorten them, to reduce exposure to radiation and to reduce complication rates, with at least equally efficiency to conventional ablation approaches. The common concept of these ”single-shot” AF ablation technologies is the creation of circular lesions for PVI by placing the ablation device at the antrum/ostium of the pulmonary veins (PVs) without the need for continuous repositioning.
Non-balloon alternatives for PVI are two circular multi-electrode catheters: the pulmonary vein ablation catheter (PVAC®; Medtronic Ablation Frontiers, Carlsbad, CA), which is based on the phased RF, duty-cycled ablation technology [1]-[4]; and the irrigated multi-electrode electroanatomically guided nMARQTM catheter (Biosense Webster, Inc., Diamond Bar, CA, USA)[5]-[6]. The two non-balloon multielectrode technologies, PVAC® and nMARQTM catheters, are different in their cooling technology, the integration with electro-anatomical mapping (EAM) system, the ability of recording PV signals during ablation, the diameter of the spiral array at the distal end (25 vs. 35 mm), and the flexibility and structure of the catheter over the wire.
This review is not intended to compare the efficacy of the circular ablation catheters to conventional PVI with single tip catheters, neither to elaborate on the complication rates and the safety concerns of the circular ablation techniques; The aim of the review is to evaluate efficacy of PVAC® and nMARQ™ catheters and suggest an optional patient selection algorithm.
Technical differences and ablation strategyPVAC® - Phased RF ablation technique
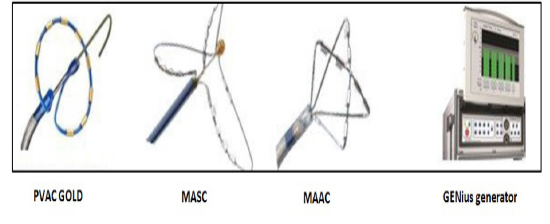
The PVAC® is one member of the phased RF AF ablation catheters family. The phased RF system utilizes anatomically designed, multi-electrode catheters with tissue temperature monitoring and a closed-loop power control generator to create contiguous, transmural lesions [Figure 1]. All three catheters monitor electrode-tissue temperature through thermocouples bonded directly to each electrode on the side of the electrode in contact with the tissue.
Figure 1. The phased RF catheter family (The circular multipolar pulmomary vein ablation catheter - PVAC GOLD; The multiarray septal catheter – MASC™; The multiarray ablation catheter - MACC™; and the The GENius™ Multi-Channel RF Ablation Generator). Image courtesy of Medtronic Inc.
Power regulation is achieved through duty-cycling of the RF energy, rather than voltage control: in contrast to conventional RF ablation that delivers continuous RF energy, “on” and “off” periods alternate during duty-cycled ablation. The length of the “on” time is regulated to reach and maintain the target temperature. The time period with no RF delivery allows accurate temperature monitoring and provides time for the electrode to cool between RF applications.
The concept of unipolar and bipolar energy delivery (phasing) means, that the multi-electrode catheter design and the generator enable simultaneous bipolar (between electrodes) as well as unipolar (from electrode to ground pad) delivery of RF energy. There is no voltage difference, thus no current flow, between neighboring electrodes while “in phase”, so only unipolar energy is delivered between each electrode and the ground pad. When the voltages for the two adjacent electrodes are “out of phase”, inter-electrode voltage difference results in bipolar RF delivery. The depth of the lesions was found to be proportional to the energy mode selected, with unipolar delivery causing the deepest lesions[7].The generator is able to deliver a mixture of unipolar and bipolar ablations. This feature is used to titrate lesion depth during PVI: in circumstances where 4:1 RF energy delivered cannot isolate the PVs (as on the ridge of the left-sided veins) – then a ratio with a higher unipolar component should be considered (e.g. 2:1). In contrast, when ablating at the posterior wall of LA and in areas with close proximity to the esophagus and other critical structures, a higher ratio of bipolar component is preferred (e.g.4:1).
PVAC® consists of a 9F, 10-platinum electrode, over-the-wire deflectable catheter, 25 mm diameter spiral array at the distal end, with the capability of straightening the circular end over the wire into the vein. The over-the-wire design provides stability of the catheter in various anatomies. It is a non-irrigated duty-cycled phased RF catheter that is able to deliver RF energy with varying mixtures of unipolar and bipolar ablations not integrated into an EAM system. PVAC® is used to isolate and then validate the electrical isolation of all PVs. PV angiography through the guiding sheath can be used to assess the catheter position in relation to the ostium so as to avoid any RF application inside the PVs. Electrograms cannot be assessed during the delivery of phased RF current because of the electrical noise; however, electrical conduction of the PVs can be assessed between the applications. Duytschaever reported a 93% diagnostic accuracy for the verification of PVI when a conventional mapping catheter was used as a gold standard[8]. Pacing maneuvers or a conventional mapping catheter can be considered whenever doubt remains regarding gaps in PV isolation[9], particularly during the learning curve.
The GENius™ Multi-Channel RF Ablation Generator (Medtronic, Minneapolis MN, USA) contains 12 independently controlled RF generators for each electrode in the catheter. It monitors the temperature on each electrode and adapts the power to achieve and maintain the target temperature (nominally 60 °C). The GENius™ monitors the power and the temperature on each electrode and displays to the operator when the power and temperature are sufficient to create a good lesion (Contact IQ) [10].
Most of the data in the literature refer to this type of catheter. Recently, PVAC Gold catheter was introduced to the market. It contains 9 gold electrodes. Gold has more than 4 times better thermal conductivity than that of platinum. Thus it allows more uniform heating and faster cooling than platinum, providing the potential for precise temperature control across the electrode[11]. Because of gold's ability to deliver energy more efficiently and consistently, it provides the potential for generating equivalently deep lesions to platinum [12]. The number of electrodes was reduced from 10 to 9 in order to eliminate the potential bipolar short circuit between electrodes 1 and 10 and to reduce microembolism[13]-[15]. In addition, a 20-degree forward tilt was added to the distal circular segment of PVAC Gold catheter for a more uniform tissue contact with the PV antrum.
Other members of the phased RF family used for substrate modification are the multiarray septal catheter (MASC™), a three-arm pull-back electrode which is designed to map and ablate the interatrial septal wall. This catheter is introduced through the transseptal puncture site, and the electrodes are positioned against the septum by pulling back on the catheter. The four-arm multiarray ablation catheter (MAAC™) is designed to map and ablate arrhythmogenic drivers in the left atrial (LA) body, such as complex fractionated atrial electrograms (CFAEs) [Figure 1].
nMARQTM - Multielectrode irrigated RF ablation technique
nMARQTM is an irrigated circular RF catheter visible and intended for integration into the CARTO system (Biosense Webster, Inc. Diamond Bar, CA, USA), which allows 3D anatomical mapping of the left atrium (LA) and PVs [Figure 2]. It consists of ten separate, openly irrigated electrodes arranged on an 8.4F decapolar catheter with an adjustable circular array of 20–35 mm diameter. An irrigation line is connected to the catheter’s central hub and perfused using a commercially available pump (during energy application 60 mL/min 0.9% saline via CoolFlow, Biosense Webster).
Figure 2. The nMARQ catheter – first generation
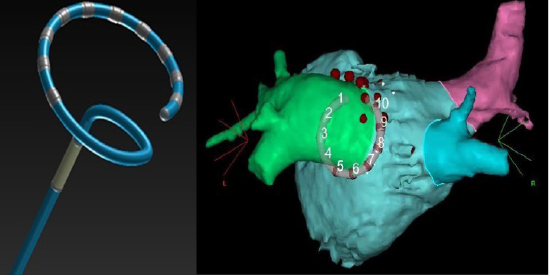
The corresponding generator (nMARQ™ Generator, BiosenseWebster)is capable of delivering RF energy over 10 separate channels independently. Up to 25 watts (W) of RF energy per electrode are delivered in unipolar mode with the temperature limited to 45 °C; (The RF energy is delivered in either unipolar or bipolar mode, but only unipolar RF is usually used for up to 60 s per application). Power delivery during ablation of the posterior wall varies between 20 and 25W in unipolar mode. In our practice and according to reports from other groups[16]-[19], unipolar RF energy is delivered with power settings of 20 W for the non-posterior zones and 15 W for the posterior areas with maximum impulse duration of 40 s. In bipolar mode, the maximum power delivery is 15W per electrode, also with temperature limited to 45°C. Each application lasts until the PV signals disappear, between 15 and 60 s each. In case of lack of atrial signals on some of the multi-electrodes, those displaying no signal are shut off during subsequent application.
With nMARQ™, atrial and PV signals can be recorded during ablation. During RF delivery, ablation-related parameters (temperature, impedance and power delivered) are monitored continuously for each active channel.Intermittent fluoroscopy is also used to assess movement of the diaphragm to avoid injury to the right phrenic nerve. Pacing for phrenic nerve capture and esophageal temperature monitoring are not routinely performed in all centers.
Prior to ablation, the individual LA anatomy is reconstructed with the CARTO system. Circular ablation can be guided by CT image integrated into fast anatomical map and by intra cardiac echo as well[20]. There is a visual display of the nMARQTM System electrodes that are in close proximity to tissue, using the TissueConnectTM technology that measures constantly and collects phase differences between current and voltage. The position of the nMARQ™ catheter at the PV ostium is optimized using a combination of fluoroscopic imaging and the EAM. Our group has shown that addition of contrast injections to standard nMARQ™ procedure is feasible and safe. It has no benefit in routine use but may have a potential added value to EAM in catheter localization by newly trained operators and in selective cases of large/common PV anatomy [21].
For evaluating isolation of PVs using nMARQTM the entrance and exit block technique can be used for very large PVs, through which the whole catheter can be entered. In smaller veins, RF delivery is continued until no PV signals are observed at the antrum (along the inner aspect of the circumferential ablation line) and atrial loss of capture can be proved (the pace-and-ablate technique) [22] or dissociated PV activity can be shown. Administration of adenosine or pacing of the ablation line is performed at the operator's discretion. Some centers use a different method[16]-[17], where the entire ablation is conducted while the recording circular lasso mapping catheter is positioned distal to the nMARQ™ catheter inside the corresponding PV.Repeated RF applications are delivered through the nMARQ™ poles facing the precise lasso electrodes showing persistent PV potentials until all the local PV electrograms recorded by the lasso catheter are disappeared. Isolation of the left-sided PVs is conducted during atrial pacing from the distal CS catheter whereas isolation of the right PVs are conducted during sinus rhythm or coronary sinus pacing. The endpoint of the procedure is the isolation of all PVs, attested by disappearance of all PV potentials in the lasso catheter within the vein and confirmed by pacing maneuvers.
The nMARQ™ catheter was first used in humans in May 2013, and the first series of patients were reported in 2014. The nMARQ™ catheter was recalled from clinical use in June 2015 due to issues with the thermocouple and reporting of three deaths,of which two were confirmed to be due to esophageal-atrial fistula[23]. The catheter was re-designed and the next prototype is under current evaluation.
Comparison of the efficacy of PVAC® and nMARQTM for paroxysmal atrial fibrillation (PAF)PVAC®Acute Success and Procedural Parameters
Procedural parameters and acute outcomes from single- and multi- center studies are presented in [Table 1]. Acute procedural success by patient is defined as complete isolation of all targeted PVs. Acute success by vein is defined as the successful electrical disconnection of a targeted PV in which PV potentials are previously demonstrated.
Table 1. Acute and longer-term results of multi-electrode circular duty-cycled RF ablation (PVAC®)
| Study |
No.patients |
Age |
Paroxysml AF(%) |
Mean LA diameter(mm) |
Procedure time(min) |
Fluoro time(min) |
Efficacy-acute success(%) |
Efficacy-long term success(%) |
F/U duration(mo) |
Major complications(%) |
Year |
| Boersma et al. [1] |
98 |
59±9 |
100 |
NA |
84±29 |
18±8 |
100 |
83 |
6 |
0 |
2008 |
| Fredesrdorf et al. [38] |
21 |
59±12 |
81 |
NA |
81±13 |
30±11 |
99 |
86 |
6 |
0 |
2009 |
| Beukema et al. [39] |
102 |
57.9±9.6 |
90 |
41.2±6.5 |
139.3±37.72 |
32.1±11.3 |
100 |
60.8 |
12.2±3.9 |
0 |
2010 |
| Duytschaever et al. [8] |
27 |
60±8 |
100 |
41±4 |
176±25 |
NA |
93 |
74 |
3 |
0 |
2010 |
| Wieczorek et al. [3] |
73 |
56±12 |
100 |
44±3 |
122±27 |
20±11 |
99 |
85 |
6 |
0 |
2010 |
| Bulava et al. [40] |
51 |
56.5±9.9 |
100 |
41.2±5.4 |
107±31 |
16±5 |
98 |
77 |
6.6±0.4 |
0 |
2010 |
| Choo et al. [41] |
38 |
56.9±10.2 |
79 |
42±7.5 |
168±41 |
39±14 |
97(100 PAF) |
68(73 PAF) |
6 |
3.9 |
2011 |
| Bittner et al. [42] |
40 |
57±11 |
53 |
43±5 |
171±40 |
26±8 |
99 |
72 |
8.5±3.3 |
0 |
2011 |
| Khaykin et al. [43] |
31 |
63±10 |
100 |
39±6 |
125±25 |
36±14 |
100 |
67 |
6 |
0 |
2012 |
| Tivig et al. [44] |
143 |
61±10 |
100 |
40±6 |
128±38 |
29±13 |
100 |
76*
74* |
7.1±5
15.9±2.8 |
2.6 |
2012 |
| Beukema et al. [45] |
89 |
56±10.4 |
100 |
42.5±3.4 |
138±35 |
31±13 |
100 |
84 |
12 |
0 |
2012 |
| Mulder et al. [46] |
120 |
59 (34-76) |
100 |
40±5 |
86±26 |
NA |
100 |
55
49 |
12
24 |
3 |
2012 |
| Nardi et al. [47] |
429 |
60±12 |
68 |
43±4 |
62±15 |
21±4 |
NA |
75.1 PAF
54.7 CAF |
22±5 |
1.8 |
2013 |
| Malmborg et al. [48] |
56 |
62±7 |
66 |
42±5 |
167±40 |
47±17 |
93 |
34 |
12 |
1.8 |
2013 |
| Looi et al. [49] |
75 |
60±10.1 |
100 |
48±4.2 |
135±54 |
46±29 |
NA |
65.3 |
25.6±5.9 |
2.6 |
2013 |
| Spitzer et al. [50] |
388 |
61.7±9.7 |
80 |
42±6 |
67±18 |
15.6±5.7 |
>99 |
64.2 |
24 |
0.5 |
2014 |
| De Greef et al. [51] |
79 |
60±10 |
66 |
41±7 |
121±41 |
33±11 |
100 |
65 |
36 |
1.26 |
2014 |
| Gal et al. [52] |
230 |
56.6±10.3 |
83.9 |
41.7±4.7 |
133.9±38.8 |
31.9±12.3 |
99.8 |
47.7 |
43 |
1.3 |
2014 |
| McReady et al. [4] |
94 |
58±12 |
100 |
38±7 |
140±43 |
35±16 |
98 |
60 |
12 |
2 |
2014 |
| Laish-Farkash et al. [19] |
93 |
61.4±9.8 |
87 |
38.8±5.4 |
94±27 |
33±13 |
97 |
79 |
12 |
0 |
2015 |
A systematic review by Andrade et al.[24] has summarized 42 publications. Overall, 1162 patients had PVAC® based ablation for PAF and 347 for persistent AF. The average age was 58.5 ± 2.6 years, and 71.7% of patients were male. Average left ventricular ejection fraction was 60.5% ± 4.0%, and the left atrial dimension was 41.4 ± 1.9 mm. For PAF, the average procedure time was 116.9 ± 33.4 minutes, fluoroscopy time was 26.5 ± 9.6 minutes, and the number of PVAC® applications per patient was 25.1 ± 3.4. For persistent AF, the average procedure time was 137.1 ± 29.3 minutes with a fluoroscopy time of 31.6 ±12.4 minutes. Significantly more PVAC® applications were required to isolate common ostia when compared with individual PVs. The data on 1147 patients from 20 studies showed that acute PVI was achieved with the PVAC® alone, without concomitant use of a focal RF ablation catheter "touch-ups", in 98.57% of the patients and in 99.38% of the targeted PVs. Six studies reported the concomitant use of irrigated RF catheter ablation to complete PVI in a median of 5.7% of patients. There was no difference in acute procedural success between patients treated for PAF vs persistent AF. Predictors of failed acute PVI with PVAC® included larger PV size (>25 mm) and increased LA size (>58 mm). Compared to early procedures, centers with extensive experience reported a progressive decrease in procedural time (95 ± 26 vs 74 ± 21 minutes for PAF; 151 ± 50 vs 100 ± 17 minutes for persistent AF), fluoroscopy time (19 ± 9 vs 15 ± 7 minutes for PAF; 30 ± 15 vs 19 ± 6 minutes for persistent AF), and mean number of PVAC® applications per patient (29 ± 7 vs 25 ± 7 applications for PAF; 29 ± 8 vs 23 ± 5 for persistent AF). It should be noted that mean procedure times below 85 min have been reported from several experienced centers for cohorts of mainly PAF patients [Table 1].
The European survey on the efficacy and safety of PVAC®[25] included twenty centers from seven European countries, 2748 patients (77% with PAF). The mean procedure time was 122 min for paroxysmal and 145 min for persistent AF (P = 0.08). Fluoroscopy times (29.4 vs. 38.6 min, P = 0.13) and RF duration (28.3 vs.42.6 min, P <0.001) were shorter in paroxysmal AF. In patients with paroxysmal AF, the pulmonary veins were isolated using the PVAC® in all centers.
Long-term success rates for different follow-up times from single- and multi- center studies are presented in [Table 1]. Long-term procedural success was defined as freedom from recurrent AF.
In the meta-analysis by Andrade et al.[24] summary analyses were limited to six studies (283 patients) for 6-month outcomes and 5 studies (272 Patients) for 12-month outcomes. For PAF, six-month freedom from recurrent AF ranged from 77.8% to 84.4%, yielding a pooled estimate of 81.36%. At one year, the pooled estimate for freedom from recurrent AF was limited by significant heterogeneity. For persistent AF, six-month freedom from recurrent AF ranged from 39.1% to 64.0%, yielding a pooled estimate of 54.1%.
In the European survey on the efficacy and safety of PVAC® [25] (2128 patients with PAF, 620 persistent AF) 81% had a structured follow-up defined as routine Holter-ECG after a mean of 11.2 months. The survey found in PAF patients an overall success rate of 82% [median 80%, interquartile range (IQR) 74–90%], with a first procedure success rate of 72% [median 74% (IQR 59–83%)]. In persistent AF, overall success rates were significantly lower with 70% [median 74% (IQR 60–92%)]; P = 0.05) as well as the first procedure success rate of 58% [median 55% (IQR 47–81%)]; (P = 0.001). The overall and first procedure success rates were similar among higher (79.1% and 68.8%) and lower volume centers (79.4% and 72.3%). However, a poorer success rate was reported off antiarrhythmic drugs (AAD) in the lower- volume centers (49.7%) than in the higher-volume centers (60.8%) centers. Further, the success rates were neither dependent on the duration of experience with duty-cycled RFA, which ranged from 1 to 4.7 years, nor with the number of procedures with duty-cycled RFA. There was a correlation between average LA diameter and success rate.
Mulder et al. [26] found that PV anatomy did not have a significant effect on the long-term results; only a tendency to a poorer outcome was seen for PVs with diameters>24 mm.
In patients with recurrent AF who underwent a second procedure after PVI by PVAC®, the reconnection rate was 73 % of all previously isolated PVs[40]. Balt et al. [56] reported that in almost all patients (98 %) with recurrent AF after previous PVAC® ablation at least one PV was reconnected, and all PVs were equally likely to show reconnection. Few studies demonstrated that superior veins were more often affected as compared with the inferior ones[57]. In other studies[58],[59], the highest rate of reconnection was observed for the inferior quadrant of the right lower PV (as opposed to the superior quadrant of the right upper PV with single tip catheters), most likely due to difficulties in appropriately engaging this vein with the PVAC® and early branching of this vein. As suggested by Rademakers et al.[59], optimal electrode-tissue contact with all electrode pairs may be more difficult to achieve due to the circular design of the PVAC® catheter.
Evaluation of the new PVAC Gold catheter is currently in progress. The post-market GOLD AF registry (ClinicalTrials.gov ID: NCT02433613) is a prospective, multi-center, single-arm, non-interventional and open-label registry, designed to evaluate the performance and describe the day-to-day clinical use of PVAC Gold phased RF PV ablation catheter. This study is intended to track minimum of 1000 patients in approximately 50 sites in Western, Central Europe, Israel and South Korea between April 2015 and February 2019. The primary endpoint is to estimate phased RF ablation mid-term success rates at 12 month follow-up. Success rates will be estimated as time to first AF recurrence and/or left atrial flutter.
nMARQ™Acute Success and Procedural Parameters
Procedural parameters and acute outcomes from single- and multi- center studies are presented in [Table 2].
Table 2. Acute and longer-term results of nMARQ circular irrigated multielectrode ablation catheter
| Study |
No.patients |
Age |
Paroxysmal AF(%) |
Mean LA diameter(mm) |
Procedure time(min) |
Fluoro time(min) |
Efficacy-acute success(%) |
Efficacy-long term success(%) |
F/U duration(mo) |
Major complications(%) |
Year |
| Scaglione et al. [28] |
25 |
57±13 |
100 |
44±8 |
131±49 |
1.8±2 |
96 |
68 |
6 |
0 |
2014 |
| Zellerhoff et al. [6] |
39 |
60±10 |
100 |
NA(area 19±5 cm2) |
86±29 |
22.2±6.5 |
98 |
66 |
140±75 |
2.5 |
2014 |
| Laish-Farkash et al. [19] |
82 |
63±10.6 |
76 |
39.4±6 |
81±18 |
30±8.5 |
95 |
80.7 |
12 |
1.2 |
2015 |
| Deneke et al. [53] |
145 |
64±10 |
53 |
NA |
115±36 |
17±7 |
99 |
66 |
12 |
2.1 |
2015 |
| Mahida et al. [27] |
374 |
60±10 |
70.3 |
NA |
114±42 |
24±14 |
99.6** |
65 |
12 |
0.5 |
2015 |
| Stabile et al. [54] |
180 |
58±10 |
78 |
46±10 |
113±53 |
13.1±8.4 |
98 |
PAF 73% Persistent 70% |
13.9±8.2 |
0.5 |
2015 |
| Vurma et al. [23] |
327 |
PAF 63±10 Pers 64.8±8.2 |
69.7 |
39±5 44±5 |
69±22 75±23 |
14.8±6.6 16.8±6.3 |
NA |
75(PAF)* 52(Persistent)* |
6±5 |
0.6 |
2016 |
| Rodriguez-Entem et al. [55] |
35 |
57.3±8.6 |
100 |
41.2±3.1 |
79.5±39.3 |
31.6±8.2 |
98.6 |
77.2 |
16.8±2.8 |
2.8 |
2016 |
| Burri et al. [18] |
50 |
58±10 |
100 |
23±5 |
100±25 |
22±8 |
100 |
46(low power settings) |
15±4 |
6 |
2016 |
| Marai et al. [20] |
31 |
55±13 |
87 |
45% nornal 42% mild 13% mod |
130±21 |
22±3 |
97*** |
87 |
15.9±3.6 |
3.2 |
2016 |
| Wakili et al. [16] |
29 |
67.1±8.6 |
100 |
40.5±6.1 |
132±37(86.5±24.6 nMARQ only) |
31±12 |
83 |
72 |
12.4±9.3 |
0* |
2016 |
| Rosso et al. [17] |
36 |
58.7±10 |
64 |
NA |
101±26.4 |
25.9±9.5 |
100## |
78(PAF 82 Persistent 69) |
19±2.6 |
0 |
2016 |
* One procedure off AAD**non-PV additional ablation: 13%PAF;27%persistent***13% touch-up ablations# one case of phrenic nerve palsy despite prophylactic stimulation and immediate abortion of ablation, one patient with esophageal lesion in the post-procedure endoscopic examination.## 2.7% touch-ups
For PAF, the average procedure time range from 69±22 to 114±42 minutes in large series of nMARQ™ patients[23], [27]; Fluoroscopy time range from 14.8±6.6 to 24±14 minutes.
Acute success rates in isolating the PVs using nMARQ™ catheter alone range from 83 to 100%. Some centers report the need for additional ablations using a single tip ablation catheter in order to achieve complete PV isolation[16]-[17], [20], [28], especially after confirmatory mapping with an additional diagnostic mapping catheter reveals persistent PV conduction.
Wakili et al.[16] described this problem in 19 out of 29 nMARQTM patients. These patients underwent further ablation, which still failed to achieve PVI in 5 of the 29 (17%) nMARQTM patients, mainly due to significant temperature rise in the esophagus (mainly in the posterior wall in the area of the left inferior PV) and technical limitations in reaching the right inferior PV. This need of an additional mapping catheter for confirmation caused a significant prolongation of the procedure duration compared with a conventional point-by-point PVI.
Similarly, Rosso et al.[17] showed that procedure times were shorter for patients with paroxysmal AF ablated with circular catheters but 11% of patients assigned to nMARQ™ ablation procedure required point-by-point ablation to close gaps left within the antral circular ablation lines done with the circular ablation catheter. This group[29] and the group of Scaglione et al.[28] have shown that a lack of correlation between a diagnosis of PVI based on the local nMARQ™ electrograms and those recorded from a more distal Lasso catheter may be seen in up to one-third of PVs, a finding that could conceivably influence the long term results.
Mahida et al.[27] reported in a large multicenter study that RF times were longer for the superior veins as compared to the inferior veins. Ablation at non-PV sites was performed at the operating physician’s discretion. Among patients with paroxysmal AF, 87% had PV isolation only while 13% had ablation at non-PV sites. Among persistent AF patients, 73% patients had PV isolation only while 27% had ablation at non-PV sites. Of these patients who had ablation at non-PV sites, 74% patients had ablation with nMARQ™ only. Of the 17% patients who had ablation with nMARQ™ and conventional catheters, 82% required ablation in the coronary sinus.
Long-term success rates for different follow-up times from single- and multi- center studies are presented in [Table 2]. Long-term procedural success was defined as freedom from recurrent AF.
In PAF patients 66-87% of patients are free of recurrent AF after a follow-up duration of at least 1 year with single procedure and no AADs [Table 2]. Longer follow-up of 19±2.6 months in a recent study that included 36 patients after nMARQ™ ablation showed 82% success rate for PAF and 69% success rate for persistent AF ablation using nMARQ™ catheter with 2.7% touch-ups[17].
Reports of esophageal injury in up to 50% of the patients [30]-[31]and cases of esophago-pericardial fistula[27],[32], have recently prompted caution to titrate energy from 20–25 W unipolar RF down to a maximum of 15 W unipolar RF[33]. Burri et al. [18] evaluated long-term outcomes of 50 AF patients after PVI using nMARQ™ with these low power settings. Follow-up was 15 ± 4 months (range 7–23 months).
There were no cases of esophageal fistula or stroke during follow-up. AF recurred in 27 (54%) of patients. Of these, 63% underwent a redo procedure. Reconnections of at least two PVs were documented in all patients (2 PVs in 2 patients, 3 PVs in 6 patients and 4 PVs in 9 patients). Reconnections were found in the left superior PV in 16 patients (94%), in the left inferior PV in 14 patients (82%), the right superior PV in 13 patients (76%) and the right inferior PV in 15 patients (88%). Isolation was achieved in all cases by point-by point RF application. There were no cases of atypical flutter or atrial tachycardia. Our group also used these low-power settings and reported the following long-term results:[19] 80.7% of nMARQ™ patients were free of AF after 1 year from index procedure, although 28% were on AADs. 4.8% patients underwent a second PVI, with an overall one-year success rate of 87.7% (26% on AADs).
Head to head comparisonAcute Success and Procedural Parameters
Our group has compared the efficacy of PVAC® vs. nMARQ™ in 175 consecutive symptomatic AF patients with a follow-up duration of at least 5 months [Table 3]. 93 patients underwent PVI using PVAC® (age 61.4±9.8 years; 60% male, 13% persistent AF) and 82 patients underwent PVI using nMARQ™ catheter (age 63.2+10.6 years; 67% male, 24% persistent AF) [19].
Table 3. Phased RF ablation outcomes in comparison with nMARQ
| Study |
No.patients |
Age |
Paroxysmal AF(%) |
Mean LA diameter(mm) |
Procedure time(min) |
Fluoro time(min) |
Additional ablation |
Efficacy-acute success(%) |
Efficacy-longterm success(%) |
F/U duration(mo) |
| Laish-Farkash et al. [19] |
PVAC:93 nMARQ:82 |
61±10 63±10.6 |
87
76 |
38.8±5.4 39.4±6 |
94±27 81±18 |
33±13 30±8.5 |
2 pts in each group were switched to the alternate technique |
97
95 |
79
80.7 |
12
12 |
Procedure and radiation times were 94±27 and 33±13 min for PVAC® and 81±18 and 30±8.5 for nMARQ™ (P = 0.0008 and P = 0.18), respectively. The number of applications and the total burning times were 20±7 and 19±6.7 minutes for PVAC® and 16+5.6 and 11+4 minutes for nMARQ™ (P <0.0001 for both), respectively. Thus, the fluoroscopy time was comparable for both procedures, but the mean procedure time was longer for PVAC®. This could be explained by several causes: (1) the learning curve of PVAC® (which entered the market before nMARQTM and required a transformation from point-by-point to circular ablation skills) was longer. We showed in our study that there were longer procedure and fluoroscopy times in the first 10 PVAC® patients but not in the first 10 nMARQTM patients; (2) PVAC® patients had longer total burning time; and (3) the lack of 3D mapping using PVAC®, as opposed to nMARQ™.
The number of applications and the total burning time were shorter for nMARQTM vs. PVAC®. This probably stems from the difference in technology: while the signals can be seen during ablation with nMARQTM and ablation can be stopped at any time after PV signals are gone, with PVAC® the signals cannot be seen during ablation and an application of one minute each is the rule. It might be as well that the need to switch off pair 1 or 5 in PVAC® patients is a potential reason for more RF lesion applications that are needed for full circumferential line of ablation.
Because of the different size of the PVAC® and nMARQTM catheters, their different flexibility, and the built-in ability of the PVAC® catheter to be straightened over the wire and enter the PVs, as opposed to nMARQTM, PV isolation was assessed by different methods for these catheters: In PVAC® patients we proved isolation by pacing and recording from inside and outside the vein and the coronary sinus, respectively, to prove entrance and exit block. The acute success rate was 97%. In nMARQTM patients, the entrance and exit block technique was used in patients with very large PVs that the whole catheter could be entered into, as in Lasso catheter (17% of nMARQ™ patients). In smaller veins, RF delivery was continued until no PV signals were observed at the antrum (along the inner aspect of the circumferential ablation line) and atrial loss of capture could be proved (the pace-and-ablate technique) [22], [34] or dissociated PV activity could be shown (83% of nMARQ™ patients). The success rate was 95%.
In two nMARQ™ patients with small atria and small PVs and in two PVAC® patients with large PVs, the procedure failed with no ability to isolate the PVs; switching to the alternative technology was successful with 100% acute success rate.
Three observations were noticed during the ablation procedures that were different when using these two ablation techniques and comparing them head to head: 1) we observed more arrhythmogenic activity at PV ostia during ablation in sinus rhythm when using the PVAC® vs. nMARQTM system (95% of PVAC® patients vs. 36.5% of nMARQTM patients) (P = 0.0001). We used a different definition for ‘triggers’/‘arrhythmogenic veins’ than the one used in previous studies[35], and the long-term significance of this observation still needs to be resolved—perhaps with some similarity to the junctional response during slow pathway ablation in AV-node re-entrant tachycardia[36]. This difference in arrhythmogenic activity during ablation could stem from the presence of a guidewire in the PVAC® system or the different energy used: unipolar in nMARQTM vs. the addition of bipolar application in PVAC®.
2) Another observation was RF application-induced coughing, probably when the PVAC® catheter was located unintentionally a few mm inside the PV, enforcing immediate cessation of the application. Using nMARQTM, the catheter was almost always out of the vein due to its larger diameter and the ability to inspect minor catheter movements by CARTO 3D mapping system; thus, we hardly ever observed this phenomenon with nMARQTM.
3) In another study comparing these two AF ablation techniques we found that there is no influence of catheter type on pain location during ablation using either PVAC® or nMARQ™ [37]. The location of pain during PVI is not catheter dependent but rather a reflection of autonomic nerves physiology.
In our study[19] one-year freedom from AF using PVAC® vs. nMARQ™, was 79% and 80.7%, respectively, after one procedure, and 88% vs. 87.7%, respectively, after redo procedures. Thus, we found no difference in 1-year freedom from AF results between the two techniques (despite different acute endpoints). This similar outcome was shown even though the diameter of the spiral array at the distal end of nMARQ™ is larger than PVAC®, indicating ablation on a more antral area. The larger PV isolation should intuitively relate to better clinical outcome, however, this was not shown, although the reduced number of applications and shorter total burning time with nMARQTM vs. PVAC® could be the direct implication of the size difference. Notably, the similar outcome was shown even though the nMARQ™ group included more patients with persistent AF. This result may suggest a better clinical outcome with the nMARQTM since persistent AF patients usually have lower rate of freedom from AF after PVI vs. paroxysmal AF patients[2].
Optional Target Population for Each Catheter
Despite this supposed clinical effectiveness of the nMARQTM system, the issue of the occurrence of life-threatening esophageal fistulas related to this system is of major concern and requires further investigation[23], [27], [30]-[32].
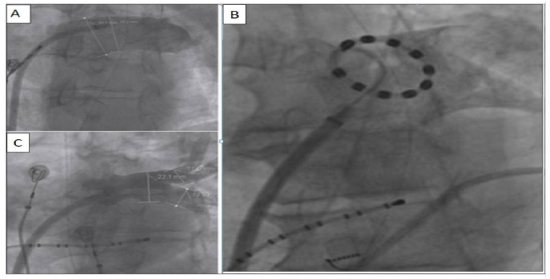
Similar to other studies [16], in our study[19] there were two nMARQTM patients with too small atria and PVs that caused inability to deploy the catheter properly, especially in the right-sided veins. The nMARQTM procedure was switched to PVAC® and the patients had successful PV isolation. In two failed PVAC® patients due to large PVs and inability to deploy the catheter properly, a redo procedure with nMARQTM was successful with a better catheter–LA contact and more efficient burnings. Thus, a patient-based pre-ablation anatomy definition is probably warranted for appropriate selection of technology type. Pre-procedure imaging of LA and PVs may guide the operators in choosing the proper circular multi-electrode system: to use PVAC® catheter for smaller LA and PVs and nMARQTM system for larger LA and larger/common-ostium PVs [Figure 3]. However, it is possible that a more anterior trans-septal puncture may solve that issue of small atria and PVs regarding the nMARQTM catheter, as well as the introduction of the new nMARQTM catheter prototype, which is more flexible and with the ability to reach a smaller minimal diameter vs. the first generation catheter. This catheter is under clinical evaluation nowadays.
Figure 3. (A) Angiogram of a large left common pulmonary vein; (B) Same vein with an nMARQ catheter in its antrum; as opposed to (C) a normal size left common pulmonary vein.
nMARQ™ should also be considered as the preferred first step approach in cases of combined AF and left atrial flutter and in cases of redo procedures, because of the integrated 3D mapping and the capability of observing the signals during ablation. An important potential benefit of nMARQTM over PVAC® is the 3D mapping option, which has an advantage in visualization of catheter location in relation to PV ostia, an advantage in voltage mapping of the atrium, an advantage in adding location points of the phrenic nerve route, a potential advantage in reducing fluoroscopy time when using CARTO-MERGE technology, and an advantage in adding lines of ablations outside PV ostium. Thus, nMARQTM system can also be considered for patients who need additional lines of ablation on top of PVI, in order to save costs by using one catheter only. This suggested approach needs to be proved in future studies.






