Effects of Computerized Decision Support Systems on management of Atrial Fibrillation: A Scoping Review
Reza Sheibani1, Ehsan Nabovati2, Mehdi Sheibani3, Ameen Abu-Hanna4, Alireza Heidari-Bakavoli5, Saeid Eslami1,4
1Department of Medical Informatics, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.2Health Information Management Research Center, Kashan University of Medical Sciences, Kashan, Iran.3Clinical Research Development Center of Loghman Hakim Hospital, Shahid Beheshti University of Medical Science, Tehran, Iran.4Department of Medical Informatics, Academic Medical Center, University of Amsterdam, Amsterdam, The Netherlands.5Cardiovascular Research Center, Mashhad University of Medical Science (MUMS), Mashhad, Iran.
Potential role of computerized decision support system on management of atrial fibrillation is not well understood.
To systematically review studies that evaluate the effects of computerized decision support systems and decision aids on aspects pertaining to atrial fibrillation.
We searched Medline, Scopus and Cochrane database. Last date of search was 2016, January 10.
Computerized decision support systems that help manage atrial fibrillation and decision aids that provide useful knowledge for patients with atrial fibrillation and help them to self-care.
Data collection and analysis:
Two reviewers extracted data and summarized findings. Due to heterogeneity, meta-analysis was not feasible; mean differences of outcomes and confidence intervals for a difference between two Means were reported.
Seven eligible studies were included in the final review. There were one observational study without controls, three observational studies with controls, one Non-Randomized Controlled Trial and two Randomized Controlled Trials. The interventions were three decision aids that were used by patients and four computerized decision support systems. Main outcomes of studies were: stroke events and major bleeding (one article), Changing doctor-nurse behavior (three articles), Time in therapeutic International Normalized Ratio range (one article), decision conflict scale (two articles), patient knowledge and anxiety about stroke and bleeding (two articles).
A computerized decision support system may decrease decision conflict and increase knowledge of patients with atrial fibrillation (AF) about risks of AF and AF treatments. Effect of computerized decision support system on outcomes such as changing doctor-nurse behavior, anxiety about stroke and bleeding and stroke events could not be shown.We need more studies to evaluate the role of computerized decision support system in patients with atrial fibrillation.
Key Words : Computerized decision support system, Atrial fibrillation, Medical informatics, Decision aid, Scoping review.
Correspondence to: Saeid Eslami, Pharmaceutical Research Center, School of Pharmacy, Mashhad University of Medical Sciences, Mashhad, Iran. Tel/Fax: 0098-5138827048, E-mail: EslamiS@mums.ac.ir
Atrial fibrillation (AF) is the most common cardiac arrhythmia and its prevalence increases with age[1]. One in five strokes are associated with AF and stroke severity is increased compared to patients with other causes of stroke. Furthermore, AF is associated with increased rates of death, heart failure and hospitalizations[2].
AF is almost a chronic disease and Lifelong treatment is needed. To avoid thromboembolic complications, Patients with AF need anticoagulation therapy and the most used drug is Vitamin K antagonists (like warfarin)[3]. Treatment with anticoagulant warfarin has to be monitored by prothrombin Ratio (PR) and the International Normalized Ratio ( INR )test[4]. Range 2 to 3 (therapeutic range) of INR minimize thromboembolic events for patients with AF.
Numerous guidelines exist for the management of AF. CHA2DS2-VASc [5] and HAS-BLED [6] scores can help to inform stroke risk and risk of bleeding [7]. However, physicians’ adherence to these guidelines has been low [8]. Computerized Decision Support Systems (CDSS) have been postulated as promising tools to improve the quality of decisions [9] in terms of physician adherence [10], [11]. Hence, decision support systems have been designed to implement guidelines also for the management of AF [12].
To investigate the advantages of CDSSs for the management of AF, several studies have been conducted which reported a positive effect [13] or no effect but according to our knowledge no review has been done to integrate these results.
Many reviews have shown effects of CDSS on practitioner performance [14]-[16] by providing patient-specific information and evidence-based recommendations. We therefore aim to systematically review studies that evaluate the effects of CDSS on any aspect that we will encounter in the studies. The specific aims of this scoping review are: 1) To review what outcome types that evaluate effect of CDSS on AF have been studied. 2) To summarize the effect of CDSS on management of AF.
For the current review CDSS is defined as any intervention that presents clinical knowledge and patient specific information for providers to enhance health and health care [17]. All aspects of AF (prevention, detection, diagnosis and treatment) were considered. Information sources were: Medline, Scopus and Cochrane database and last date searched was 2016, January 10.
Search strategy and study selection
Our full electronic search strategy for Medline was:
(clinical decision support systems[MESH] OR decision support system*[TITLE/ABSTRACT] OR decision support tool*[TITLE/ABSTRACT] OR reminder system*[TITLE/ABSTRACT] OR reminding system*[TITLE/ABSTRACT] OR alert system*[title/abstract] OR alerting system*[title/abstract] OR computer assisted decision making[MESH] OR computer assisted decision making[TITLE/ABSTRACT] OR diagnosis, computer assisted[MESH] OR computer assisted diagnosis[TITLE/ABSTRACT] OR computer assisted therapy[MESH] OR computer assisted therapy[TITLE/ABSTRACT] OR expert systems[MESH] OR expert system*[TITLE/ABSTRACT] OR *CDS*[TITLE/ABSTRACT] OR medical order entry systems[MESH] OR order entry system*[TITLE/ABSTRACT] OR computerized order entry[TITLE/ABSTRACT] OR computerized prescriber order entry[TITLE/ABSTRACT] OR computerized provider order entry[TITLE/ABSTRACT] OR computerized physician order entry[TITLE/ABSTRACT] OR electronic order entry[TITLE/ABSTRACT] OR automated order entry[TITLE/ABSTRACT] OR CPOE[TITLE/ABSTRACT]OR electronic prescribing[MESH] OR electronic prescribing[TITLE/ABSTRACT] OR electronic prescription[TITLE/ABSTRACT] OR computer assisted therapy[MESH] OR computer assisted therapy[TITLE/ABSTRACT] OR computer assisted drug therapy[TITLE/ABSTRACT]) AND (atrial fibrillation*[TITLE/ABSTRACT] OR Auricular Fibrillation*[TITLE/ABSTRACT] OR Atrial Fibrillation [MESH]).
This search strategy was modified for other databases.
Inclusion criteria were:
1. Studies evaluating effects of a CDSS on all aspects of AF.
2. CDSS provided clinical knowledge to augment clinician decisions or patient specific information to reinforce patient decisions.
3. Real world clinical studies.
Exclusion criteria were:
4. Letters, abstracts, conference proceeding, study protocols, reviews and meta-analysis.
5. Studies that only assessed accuracy and sensitivity.
Searching was complemented by reviewing bibliographies listed in identified articles. Two reviewers screened the titles and abstracts and evaluated the eligibility of studies for detailed evaluation. Disagreements were resolved through consensus or consulting a third reviewer.
Two reviewers extracted, separately, data from the selected studies. Data items were: participants (sample size, audience and characteristics), type of the interventions, primary and secondary outcomes, design of studies (cross sectional, case control, cohort, before-and-after and Randomized Control Trial (RCT)) and results of the studies.
Selected studies were evaluated using a previously published tool in prevention of cardiovascular disease [18]. It provides a maximum of 10 points for quality. The following aspects were considered: Allocation to study groups, data analysis and presentation of results, presence of baseline differences, objective outcomes and percentage of follow-up [Table 1].
Table 1. The tool used to rate the quality of the studies
| Quality assessment aspects |
score |
| Allocation to study groups |
|
| Random |
2 |
| Quasi-random |
1 |
| Selected concurrent control |
0 |
| Data analysis and presentation of results |
|
| Appropriate & clear |
2 |
| Inappropriate or unclear |
1 |
| Inappropriate & unclear |
0 |
| Presence of baseline differences between the groups |
|
| No baseline differences present or appropriate statistical adjustment made |
2 |
| Baseline differences present & no statistical adjustment made |
1 |
| Baseline characteristics not reported |
0 |
| Objectivity of the outcomes |
|
| Objective outcomes or subjective outcomes with blinded assessment |
2 |
| Subjective outcomes with no blinding but clear criteria |
1 |
| Subjective outcomes with no blinding & poorly defined |
0 |
| Completeness of follow-up for the appropriate unit of analysis |
|
| 90% |
2 |
| From 80% to 90% |
1 |
| < 80% or not described |
0 |
Each item has a score between 0 to 2.
Studies were classified according to type of outcomes. Effects of CDSS on each outcome were extracted and classified as statistically significant positive effects and no effect. Mean differences of outcomes and confidence intervals for a difference between two means are reported. The included studies were heterogeneous and were classified as being one of: Randomized Controlled Trial (RCT), Non-Randomized Controlled Trial (before-after studies), Observational study with controls (cross-sectional studies and cohort studies with controls ), Observational study without controls (cohort studies without controls or case series)[19].
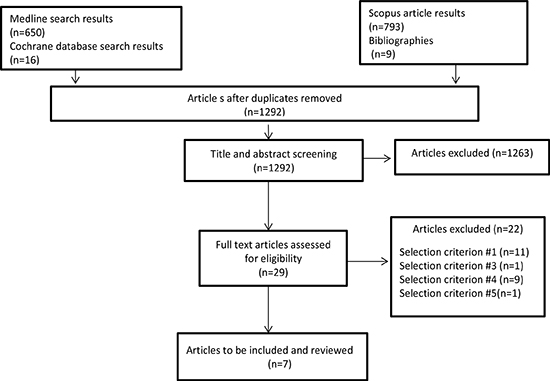
Our search strategy yielded 1292 distinct articles from all sources. 1263 articles were excluded by assessing the title and abstract. Full text assessment of the 29 articles was done and seven eligible studies were included in the final review [Figure 1].
Figure 1. flow diagram for selecting of studies
All papers were published after 2007. The following study types were present in our final selection: one observational study without controls [20], one non-RCT [21], three observational studies with controls [22]-[24] and two RCTs [13], [25]. The sample size of AF patients, varied from 44 [21] to 6,123 [20] [Table 2]. Two studies were conducted in an inpatient setting and five in an outpatient setting. Patients were excluded if they were ambulatory patients or on a cardiology service [24], receiving warfarin for less than 6 months [21], did not speak English [25], poor hearing or eyesight [13], cognitive impairment [13], [25], contraindication to ASA or warfarin [13], [25], taking warfarin for another indication [13], [25], nursing home residence [13], previous stroke or transient ischemic attack [25] , inpatients [23] and no patients were excluded from one study [22]. Computerized tools were used in six papers and an intervention consisting of a CDSS, education and feedback, was used in one paper [22]. Three of the tools were decision aids and were used by patients [13], [21], [25]. Five papers were of high quality and two papers were of poor quality (on a scale of 10, 5 or less than 5 was their score). Details of quality evaluation are presented in table 3.
Table 2. Characteristics of the included studies
| Authors, year of publication |
Sample size |
Setting |
Type of intervention |
audience |
Design of study |
| Cook, D. A. et al [24], 2015 |
Control period No. (n = 226 patients),
Notification period No. (n = 268 patients) |
inpatient |
CDSS(clinical alert system that notify providers of abnormal test results) |
Provider (physician) |
Observational study with controls |
| Robson, J. et al [22], 2014 |
4604 patients |
outpatient |
Mixed (altering professional beliefs using education, CDSS to facilitate decision making and motivating change using evaluative feedback) |
Provider (physician) |
Observational study with controls |
| Simmons, B. J. et al [21], 2012 |
44 patients |
outpatient |
Decision aid ( patient self-management (PSM) program) |
patients |
Non-RCT |
| Fraenkel, L. et al [13], 2012 |
Control group (n = 66 patients),
Intervention group (n = 69 patients ) |
outpatient |
Decision aid (a tool for nonvalvular atrial fibrillation (NVAF) to notify patients of their stroke and bleeding risks, assist in clarifying priorities) |
patients |
RCT |
| Hendriks, J. M. L.et al [23], 2010 |
ICCP group(n=111 patients)
control group(n=102 patients) |
outpatient |
CDSS(stroke risk score was calculated and 2006 guidelines for AF patients were implemented) |
Provider (nurse) |
Observational study with controls |
| Wess, M. L. et al [20], 2008 |
6,123 patients |
inpatient |
CDSS( a tool to calculate individual stroke and bleeding risk and risk–benefit analysis for anticoagulation is done)
|
provider |
Observational study without controls |
| Thomson, R. G [25], 2007
|
109 patients (intervention(n=53)control(n=56)) |
outpatient |
decision aid(applied in shared decision-making clinic) |
patients |
RCT |
Table 3. Details of quality evaluation
|
[24] |
[22] |
[21] |
[13] |
[23] |
[20] |
[25] |
| Allocation to study groups |
0 |
0 |
0 |
1 |
0 |
0 |
2 |
| Data analysis and presentation of results |
2 |
2 |
2 |
1 |
2 |
2 |
2 |
| Presence of baseline differences between the groups |
2 |
0 |
2 |
2 |
1 |
2 |
2 |
| Objectivity of the outcomes |
2 |
2 |
2 |
2 |
2 |
2 |
2 |
| Completeness of follow-up for the appropriate unit of analysis |
0 |
0 |
1 |
2 |
0 |
0 |
2 |
| Sum of scores |
6 |
4 |
7 |
8 |
5 |
6 |
10 |
Effects of CDSS on outcomes of studies
The included studies differed in study design and/or type of interventions and/or in their control groups. Main outcomes were: stroke events and major bleeding, changing doctor-nurse behavior, time in therapeutic INR range, decision conflict scale, patient knowledge and anxiety about stroke and bleeding [Table 4]. Below we address each outcome separately.
Table 4. Outcomes and effect sizes for the selected studies
| reference |
outcome |
Effect size |
effect on outcome |
Quality rating |
| [24] |
Prescription of warfarin |
In the control period 94 patients were high risk and 34 of them (36%) received warfarin but in the notification period 125 patients were high risk and 34 of them (27%) received warfarin. (Odds ratio, 0.66 [95% CI, 0.37–1.17]; p = 0.16). |
No effect |
6 |
| [22] |
• The proportion of AF patients with a CHA2DS2-VASc score ≥1 on anticoagulants• The proportion of AF patients with a CHA2DS2-VASc score ≥1 on aspirin |
• Oral anticoagulant use increased from 52.6% to 59.8% (trend difference P<0.001) Aspirin use declined from 37.7% to 30.3% (trend difference P<0.001). |
• Positive (statistically significant)• Positive (statistically significant |
4 |
| [21] |
• Time in the therapeutic INR range(TTR)• number of INR tests |
• No significant difference in TTR occurred between the before and after intervention periods (82.9% vs 81.2%, p=0.65).• Intervention increased the mean number of INR tests per patient (2.97 to 4.38, p<0.01). |
• No effect• Positive (statistically significant) |
7 |
| [13] |
• Decision conflict scale• Knowledge• Change in treatment• anxiety |
• Informed subscale (mean difference = −11.9, 95% CI =−21.1 to −2.7) and Values Clarity subscales (mean difference = −14.6, 95% CI=−22.6 to −6.6) were lower in the intervention group.• Participants in the intervention group knew medications for reducing stroke risk significantly better than the control group (61% vs 31%, p=0.001). |
• Positive (statistically significant)• Positive (statistically significant)• No effect• No effect |
8 |
| [23] |
Guideline adherence |
Guideline adherence was increased significantly to 96% in the ICT-supported integrated chronic care program (ICCP) group compared with 70% in the control group (p<0.001). |
Positive (statistically significant) |
5 |
| [20] |
• major gastrointestinal bleeding• acute stroke |
The patients who actually received an anticoagulant but decision support tool recommended not to use the anticoagulant, had a high risk of bleeding and for them receiving warfarin was related to increased hazard of gastrointestinal bleeding (Hazard ratio=1.54, p=0.03). |
• Positive (statistically significant)• No effect |
6 |
| [25] |
• decision conflict scale• anxiety• knowledge |
Decision Conflict Scale was lower in the computerized decision aid group versus the paper guidelines group in the post-clinic; mean Difference -0.18 (95% CI -0.34 to -0.01). |
• Positive (statistically significant)• No effect• No effect |
10 |
Stroke events and major bleeding
Acute stroke and major bleeding were assessed in a cohort study [20]. A decision support tool that determines patient’s risk of bleeding and stroke was proposed. The patients who actually received an anticoagulant when the CDSS was not in practice used but after that decision support tool recommended not to use the anticoagulant, had a high risk of bleeding and for them receiving warfarin was related to increased hazard of bleeding (Hazard ratio=1.54, p=0.03).
Changing doctor-nurse behavior
Two trials reported changing physician behavior [22], [24]. In one cohort study with historical control, an automated system for identifying newly diagnosed AF was proposed [24]. A computerized clinical alert system was developed by decision rules intended to automatically notify physicians. In the control period 94 patients were high risk and 34 of them (36%) received warfarin but in the notification period 125 patients were high risk and 34 of them (27%) received warfarin. (Odds ratio, 0.66 [95% CI, 0.37–1.17]; p = 0.16). The intervention did not change provider behaviors. In [22] was performed a cross sectional analysis with a mixed intervention (guidance, education, software enhancements and evaluative feedback). CHA2DS2-VASc and HAS‑BLED scores were calculated and Pop-up reminders were used. From April 2011 to April 2013, oral anticoagulant use increase from 52.6% to 59.8% (trend difference P<0.001). One trial reported changing nurse behavior. The cohort study with historical control reported guideline adherence in the treatment of AF as an outcome [23]. Computer-Assisted Decision Support System directed medical therapy according to the patient’s profile and clinical guidelines. Guideline adherence was increased significantly to 96% in the ICT-supported integrated chronic care program (ICCP) group compared with 70% in the control group (p<0.001).
Effects of decision aids on outcomes of studies
Time in the therapeutic INR range
One before and after study reported the Percentage of time spent within the therapeutic range (TTR) [21]. Patients received the recommended dose of a decision support tool. No significant difference in TTR occurred between the before and after intervention periods (82.9% vs 81.2%, p=0.65).
Decision conflict scale [26] was used for reporting the decision conflict between treatment choices (antiplatelet drugs or warfarin therapy) in two studies [13], [25]. Four subscales of the decision conflict scale are: uncertainty, informed, values clarity, and support.
In a randomized control trial, a decision aid presented advantages and disadvantages of warfarin treatment and an assessment of DCS (Decision Conflict Scale) was done. It was lower in the computerized decision aid group versus the paper guidelines group, mean differences (95% CI) were 0.02 (-0.22 to 0.26), -0.18 (-0.34 to -0.01) and -0.15 (-0.37 to 0.06) at pre-clinic, post-clinic and three month follow-up [25]. In a clustered randomized controlled trial, a decision support tool was developed as an application that runs on a laptop computer and risks of stroke and bleeding for both antiplatelet drug and warfarin were shown. Informed subscale (mean difference = −11.9 , 95% CI =−21.1 to −2.7) and Values Clarity subscales (mean difference = −14.6, 95% CI=−22.6 to −6.6) were lower in the intervention group [13].
Anxiety about stroke and bleeding
Two RCT studies reported anxiety or worry about stroke and bleeding as an outcome [13], [25]. The decision aid was designed for informing patient’s stroke and bleeding risks and clarifying priorities but did not affect participants’ anxiety (mean difference = −0.38, 95% CI = (−1.4 to .67), p=0.477)in [13]. Furthermore, in [25] the intervention was a computerized decision aid applied in shared decision-making and reduction of anxiety by the decision aid did not differ from the control group (F (1, 95) =0.001; p=0.98).
Two trials assessed patient knowledge [13], [25]. Participants in the intervention group knew medications for reducing stroke risk significantly better than the control group ( 61% vs 31%, p=0.001) [13]. Knowledge scores were improved after the clinic (participants taking warfarin had a higher mean warfarin knowledge score than participants on aspirin (difference=1.79 with 95% CI 1.00 to 2.59)) but after three months were back to the pre-clinic level and there was no significant difference between the decision aid and the guidelines groups [25].
In this study we assessed the effect of CDSS on all aspects of AF. We systematically reviewed seven studies. Two RCTs that had the highest quality reported positive effect on main outcome [13], [25]. Two of the observational study with controls reported positive effect on all their outcomes [22], [23] but one of them reported no effect on its outcome [24]. Mix of positive, absence of, and negative effects was considered as one class of the measured effects in [27] and was reported in four of selected studies (two RCTs and one non-RCT and one observational study without controls).
We began to do a systematic review study with focus on a well-defined question and assessed the quality of included studies. But as we will explain bellow we had only one or two studies that reported the same results for outcomes and we had different study designs. we could not answer specific review questions so we decided to do the scoping review that had broader topics and is possible with many different study designs [28].
One study reported that a computerized clinical alert system did not change providers’ behaviors and reported no effect [24] but another reported improvement in clinical management AF [22]. The quality of the former was higher than the latter and the latter used a mixed intervention. It is difficult to estimate which part of the intervention pertained to the reported improvement. Furthermore, only one low quality study reported the effect of CDSS on guideline adherence[23] thus we have not enough evidence to determine the effect of CDSS on improving guideline adherence and changing doctor-nurse behavior in the treatment of AF.
Reporting no effect of the CDSS on changing physician behavior was unsurprising. Other studies of decision support systems showed that these do not perform as expected [29]. Inappropriate timing and need to click to access information[24] and alert fatigue [30] were reported as the main reasons. Improving the human-computer interface, providing recommendations for patients in addition to practitioners [31], prioritizing and filtering recommendations for the user [32] can improve the effectiveness of CDSS interventions.
Due to scarcity of evidence for clinical improvement [33], [34] we had only one study that evaluated stroke events and major bleeding [20]. The rates of bleeding were higher in patients who received warfarin, but the decision support system indicated they should not so a decision support system can be a good predictor of bleeding for who warfarin might be harmful. Furthermore, only one study reported the percentage of time spent within the therapeutic range (TTR) and it did not report on a statistically significant improvement. This lack of evidence is a main limitation of our study.
This study had other limitations. The large heterogeneity in the studies meant that meta-analysis is not meaningful. We also could not perform pooled analysis because the two high quality RCTs that reported on anxiety, the decision conflict scale and patient knowledge [13], [25] had different comparison groups: one study compared the decision aid group to a usual care group [13] ,the other compared the decision aid group with an evidence-based paper guidelines group [25]. Furthermore, randomization methods and blinding differed markedly, resulting in further heterogeneity among studies.
Two RCT studies [13], [25] reported no significant difference in psychological outcomes such as anxiety between groups. This coincides with [35] that reported no difference in anxiety scores between decision aid and usual care groups. So decision aids did not have psychological negative effects.
Two studies [13], [25] reported the decision aids for patients with AF decrease decisional conflict. This result is similar to a review [36] that evaluated effects of educational and behavioral interventions on reducing decision conflict for oral anticoagulation therapy (OAT) in patients with AF. Moreover, these two RCTs showed that the decision aids improve knowledge of patients with AF although one study reported that knowledge returned to the baseline level after three months and there was no significant difference between the decision aid and the guidelines groups [25]. The paper guidelines that were used in control group may limit findings significant effect of decision support systems on patient knowledge.
Clear and intuitive user interface was reported as a feature for evaluation of CDSS [37] but only two of the included studies [24], [25] presented the screen of the computerized intervention. If characteristics of output such as content, channel, timing and format [38] were clearer, we could more accurately interpret the results of interventions and evaluate the effect of these characteristics on success of the intervention.
Strengths of the current review include the fact that we searched Medline, Scopus and Cochrane databases and conducted this review in accordance with the PRISMA statement [39] for reporting on review. As far as we know, this is the first review of studies that evaluate the effect of CDSS on all aspects of AF.
Several trial protocols describe trials that investigate the effect of CDSS on AF management [12], [40], [41] but their results are not published yet. These randomized control trials may provide supplemental evidence.
Although limited by a small number of studies, decision aids seems to have significant benefits in decisional conflict reduction and improve knowledge of patients with AF. Computerized tools that addressed AF patients did not show the psychological negative effect and did not affect participants’ feeling of worry about stroke and bleeding. The included studies did not show significant effect of CDSS on stroke event rates, time in the therapeutic INR range and doctor-nurse behavior. We need more studies to evaluate the role of computerized decision support system in patients with atrial fibrillation.
RS and EN screened the titles and abstracts and evaluated the eligibility of studies and extracted data. Disagreements were resolved by MS. RS and MS drafted the paper. AH as a clinical expert and SE and AA that are experts in medical informatics, were involved in interpretation and revising the final version.
This work was supported by Mashhad University of Medical Sciences (MUMS). MUMS had no role in the study design, data collection and analysis, reporting the outcomes and decision to publish this paper.
None of the authors has any financial and personal relations with relevant people or organizations that could have affected this work.






