Postpacing Interval During Right Ventricular Overdrive Pacing to Discriminate Supraventricular from Ventricular tachycardia
Kivanc Yalin1, Ebru Golcuk2, Ekrem Bilal Karaayvaz3, Tolga Aksu4, Muhammet Arslane5, Selma Kenar Tiryakioglu1, Ahmet Kaya Bilge6, Kamil Adalet6
1Uşak University, Faculty of Medicine, Department of Cardiology, Uşak-Turkey.2Balıkesir University, Faculty of Medicine, Department of Cardiology, Baslıkesir-Turkey.3Bagcilar Education and Research Hospital, Istanbul-Turkey.4Kocaeli Derince Education and Research Hospital, Cardiology Clinic, Kocaeli-Turkey.5Medtronic Turkey Office, Istanbul-Turkey.6Istanbul University, Istanbul Faculty of Medicine, Department of Cardiology, Istanbul-Turkey.
Failure to differentiate supraventricular from ventricular arrhythmias is the most frequent cause of inappropriate implantable cardioverter-defibrillator (ICD) therapies. We hypothesized that the postpacing interval (PPI) after overdrive right ventricular pacing may differentiate ventricular (VT) from supraventricular tachycardia (SVT) such as sinus tachycardia, atrial flutter and atrial tachycardia. This hypothesis is based on the entrainment maneuver. Reentrant tachycardia circuit for VTs would haveshorter distance to RV apex than SVTs have, and the conduction time between a ventricular pacing site and the tachycardia origin is expected to be shorter in VTs than in SVTs.
220episodes from 38 patients with single chamber ICDs that RV overdrive pacing could not terminate or change the tachycardia cycle length (TCL) were retrospectively reviewed. Episodes were classified as VTs (n=115) and SVTs (n=105). TCLs, PPIs and PPI-TCL were compared between groups.
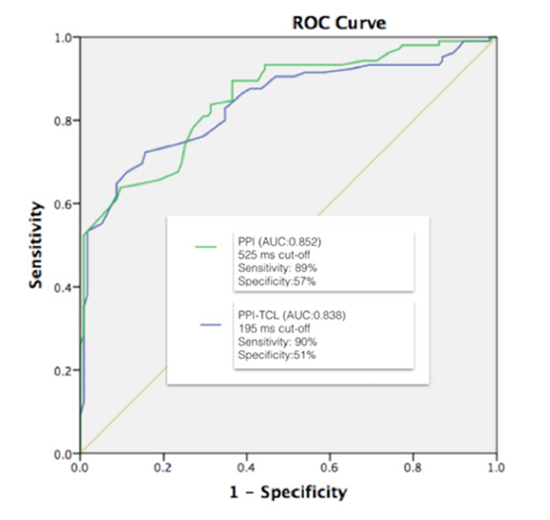
The cycle length of VTs was shorter than SVTs (320.6±30.3 vs 366.5±40 ms, p=0.001). PPI and PPI-TCL of VTs were shorter than SVTs (504.7±128.3 vs 689.2±121.8 ms, p=0.001, 184±103 vs 322.6±106.6 ms, p=0.001; respectively). ROC curve analysis demonstrated a 525 ms cut-off value for PPI has 89% sensitivity and 57.4% specificity to predict inappropriate ICD therapies due to SVTs (AUC:0.852). Similarly, A PPI-TCL <195 ms favored VT as a diagnosis rather than SVT with a 90% sensitivity, and 51% specificity (AUC:0.838).
Analyzing of PPI during overdrive pacing from RV apex may discriminate supraventricular from ventricular tachycardia. This criterion may have a potential role in implantable devices that use a single ventricular lead.
Key Words : Antitachycardia pacing, Inappropriate shock, Discrimination.
Correspondence to: Kivanc YALIN, MD, FEHRA Uşak University, Faculty of Medicine Department of Cardiology, Uşak Turkey yalinkivanc@gmail.com
The most common cause of sudden death in patients with structural heart disease is scar related reentrant ventricular tachycardia[1]. The implantable cardioverter-defibrillator (ICD) therapy is the most powerful therapeutic tool in the treatment of ventricular tachyarrhythmia (VT) and for the prevention of sudden cardiac death[2],[3]. Atrial fibrillation or atrial tachycardia/flutter with fast AV conduction and sinus tachycardia are frequent causes of inappropriate ICD discharges due to misclassification of the tachycardia[4]. The rate of the conducted supraventricular tachycardia (SVT) may exceed the upper detection interval at which discriminators and morphology templates are programmed, leading to inappropriate shocks that are usually preceded by an episode of anti-tachycardia pacing [5]. Overdrive pacing from RV apex may successfully terminate the tachycardia in many cases. But if it is unsuccessful it may be expected to entrain the tachycardia. Entrainment maneuvers are widely used in electrophysiological studies to to differentiate between mechanisms of tachycardia. In a patient with ICD, the conduction time between a right ventricular apex and the tachycardia origin is expected to be shorter in VTs than in SVTs(provided there are no accessory AV connections). Depending on entrainment phenomenon, post-pacing interval (PPI) after unsuccessful ATP for VT should be shorter than the PPI for SVTs. Therefore, assessment of PPI on device stored EGMs may help to to discriminate between the VT and SVT.
For this study, we retrospectively analyzed 38 consecutive patients (30 male, 8 Female) with single lead ICD, who had ICD and tachyarrhythmia therapies. Events were adjudicated by three observers (KY, EG, MA) on the basis of arrhythmia onset, EGM configuration and regularity.Clinical features, tachycardia ECG if available, electrophysiological study findings were checked after ICD-EGM analysis were checked to increase tachycardia discrimination probability. Leads implanted other than RV apical site were excluded. Tachycardia episodes were classified into VTs and SVTs (sinus tachycardia, atrial flutter and atrial tachycardia).Atrial fibrillation episodes were excluded due to impossibility of entrainment. Episodes due to any non-physiological condition such as over-sensing, were excluded. Patients who have evidence of AV conduction disorder or extranodal conduction were also excluded. Onset and stability parameters were either turned off or programmed to monitor only to allow delivering ATP therapies to supraventricular arrhythmias. After first inappropriate shock, stability and onset parameters programmed on.
PPI was considered as the interval, in milliseconds, between the last stimulus artifact of the pacing train and the first rapid deflection crossing the baseline of the first non-stimulated beat, in the ventricular EGM channel. Difference between PPI and tachycardia cycle length (PPI-TCL) was also obtained. TCL was determined the average of five consecutive cycle lengths of the ambient tachycardia rate prior to ATP. The episode is excluded, if there is 50 ms or greater change in pre- and post-ATP TCL.
All continuous variables were represented as mean±standard deviation while categorical variables were expressed as numbers and/or percentages. Data were analyzed using SPSS software. Kolmogorov Smirnov test was used to assess statistical distribution.Student t-test or Mann-Whitney U test were used to assess significance and p value less than 0.05 was regarded as significant. Receiver operator curves (ROC) were used to determine cut-off values to discriminate VTs from SVTs.
Thirty-eight patients were enrolled to the study. Demographic data of the study patients was presented in [Table 1]. Mean age of the study patients was 56±12years and 30 were male. Twenty-four patients had ischemic cardiomyopathy and 14 had nonischemic cardiomyopathy. Mean LVEF was 28±17%. All the patients underwent single lead ICD implantation for secondary prevention. All defibrillators were from the same manufacturer (Medtronic Inc. Minneapolis, MN). Total 1063 tachycardia episodes that ATP therapy was delivered were reviewed. Eight hundred thirty-eight of these episodes were successfully terminated by ATP, and ATP was accelerated the tachycardia in 5 episodes. For this study, 220 tachycardia episodes that RV overdrive pacing could not terminate or change the TCL were enrolled and retrospectively classified as VT or SVT by experienced observers [Table 2]. Episodes classified as VTs (n=115) and SVTs (n=105). Hundred and five SVTs were diagnosed as follows; 25 atrial tachycardia, 55 sinus tachycardia and 25 atrial flutter.
Table 1. Clinical characteristics (n=38), LVEF: left ventricular ejection fraction, CMP: cardiomyopathy.
| Variable |
Mean±SD or % |
| Age (years) |
56±12 |
| Male sex |
79% |
| LVEF |
28±17% |
| Ischemic CMP |
63% |
| Beta-blockers |
89% |
| Amiodarone |
73% |
The TCL of VTs was shorter than SVTs (320.6±30.3 vs 366.5±40 ms, p=0.001).PPI and PPI-TCL of VTs were shorter than SVTs (504.7±128.3 vs 689.2±121.8 ms, p=0.001 and 184±103 vs 322.6±106.6 ms,p=0.001; respectively). ROC curves applied to both PPI and PPI-TCL measurements [Figure 1]. ROC curve analysis demonstrated a 525 ms cut-off value for PPI has 89% sensitivity and 57.4% specificity to predict inappropriate ICD therapies due to SVTs(AUC:0.852). Similarly, APPI-TCL <195 ms favored VT as a diagnosis rather than SVT with a 90% sensitivity, and 51% specificity (AUC:0.838).Sixty-six of 115 episodes classified as VT had PPI<525 ms. And sixty-two of the episodes had PPI-TCL than 195 ms cut-off value.
Figure 1. ROC analysis of PPI and PPI-TCL measurements
The main finding of our study is PPI and PPI-TCL after failed ATP based on discrimination seems to be safe and effective in single lead devieces. Due to inappropriate ICD therapies occur mostly due to supraventricular arrhythmias 4and affect most of the patients,ICD programming strategies aimed at reducing inappropriate ICD therapies result in significant reduction in mortality, with no increase in the risk of syncope[6]-[8]. This emphasizes the need to improve ICDalgorithms to minimize inappropriate shocks and to enhance ATPas first-line therapy. By using the atrial rhythm, dual-chamber ICDs are expected to discriminate more precisely between SVT/VTs compared with single-chamber ICDs. Kolp C et al found that in patients with dual-chamber devices, inappropriate therapies are lower than patients with single-chamber devices[9]. The reason behind the wide usage of dual-chamber ICDs may lie on the benefit of them in SVT/VT discrimination. Peterson et al. [10]reported that, in clinical practice patients often receive dual-chamber ICDs, even without clear indications for pacing. The use of dual-chamber device compared with a single chamber device was associated with a higher risk of device-related complications and similar 1-year mortality and hospitalization outcomes. Dual-chamber devices are costlier for the initial implant and are associated with a greater risk of generator depletion. For these disadvantages of dual-chamber ICDs, several discrimination algorithms have been developed for single-chamber ICDs.
Table 2. Comparison of VTs and SVTs. TCL: tachycardia cycle length, PPI: postpacing interval, PPI-TCL: difference between postpacing interval and tachycardia cycle length.
| Variable |
VT (n=115) |
SVT (n=105) |
P value |
| TCL (ms) |
320.6±30.3 |
366.5±40 |
0.001 |
| PPI (ms) |
504.7±128.3 |
689.2±121.8 |
0.001 |
| PPI-TCL (ms) |
184±103 |
322.6±106.6 |
0.001 |
As onset and stability are nowadays the cornerstone of modern single-chamber discrimination algorithm, there are several limitations of the current algorithms. Swerdlow et al.[11]showed that the sudden onset failed to detect 0.5% of spontaneous VT episodes. Other limitation of the onset criterion is the inability to distinguish paroxysmal ATs with sudden onset. We hypothesized that the PPI following a failed episode of ATP for true VT is significantly shorter than the PPI for SVT and therefore may be used to discriminate the origin of the tachycardia, and therefore these parameters could be incorporated into ICDs redetection algorithms or a complement to the conventional algorithms. These conclusions are based on the presented statistically significant difference between PPI and PPI-TCL between VTs and SVTs.At first glance, a 90% sensitivity and 57% specificity seem to be still low in this settingand If PPI would be the sole discriminating factor, a cut-off of 195 ms would potentially miss one out of ten VTs not responding to ATP, falsely labeling it as SVT and potentially putting the patient in great danger. However, ATP is not just a discriminator it is also a therapeutic maneuver.ATP has been reported to successfully terminate VT in over 90% of cases, making this a very successful and pain free therapy in ICDs[12]. Therefore, programming strategies now use ATP as initial therapy even in fast VT episodes if the rhythm is found to be stable[13].Shock reduction can be accomplished with multiple bursts of ATP to treat fast VTs in patients with ICDs. Anguera et al.[14]compared the safety and effectiveness of a single ATP burst (Group 1) with a strategy of successive ATP sequences (Group 2) for termination of FVT episodes before shock therapy. Over a mean follow-up of 35 months, effectiveness of the 1st burst ATP in Group 1 was 73% and shocks were required in 27% of episodes. Effectiveness of the 1st burst ATP in Group 2 was 77%, and this increased to 91% with the 3rd or successive ATP bursts. Acceleration occurred in 8.9% of treated FVT episodes and 56.9% of accelerated episodes required shocks.
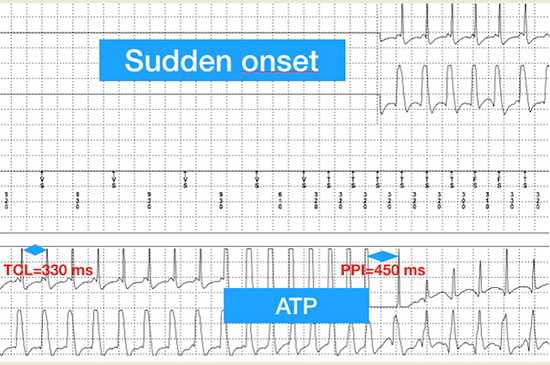
Figure 2. An example of a VT episode. ATP: antitachycardia pacing, PPI: postpacing interval, TCL: tachycardia cycle length.
Even ATP failed to terminate VT episode, this can still be used to differentiate SVTs from VTs in ICDs. Using the current algorithm as a discriminator, ATP would terminate 90 of 100 VTs, and our 195 ms cut-off would successfully discriminate 9 of remaining VTs and allow further therapies. Thisconcept of entrainment has been defined as a basic electrophysiologicalmaneuver to indicate the proximity of a rovingpacing catheter to a macro-reentrant circuit or focal tachycardia[15],[16]. Consistent with literature, our discrimination technique based on entrainment maneuver seems to be safe.
Michael KA et al.[17]postulated that the PPI and PPI - TCL would be greater in AT/AF vs. VT after episodes of failed ATP. They evaluated patients implanted with dual (DR)/biventricular (BIV)ICDs. Cut-offs of 615 ms for the PPI[AUC 0.93; 95% confidence interval (CI): 0.84–1.00; P<0.01] and 260 ms for PPI - TCL (AUC 0.86; 95% CI: 0.74–0.98; P<0.01) were identified to discriminate SVTs from VTs.Although their study did not enroll patients with single-chamber ICDs, they concluded that their results may have particular relevance in patients with single-chamber ICDs, in which atrial EGMs are not available for analysis, and in patients with chronic AF to differentiate rapidly conducted AF from dual tachycardia.Our results are concordant with the previous studies. Entrainment based discrimination algorithm has been shown to be effective in single chamber ICDs.
In our cohort antitachycardia pacing, could terminate or differentiate the VT from SVT in 904 of 1063 episodes (85%), but accelerated only 5 episodes %0.4). Our results confirm both efficacy and safety of ATP, and gives rise to the rationality of programming early ATP for both discrimination and therapy. The role of programming the device to deliver early ATP and combining it with other discrimination algorithms should be interest of further research.
The sample size of this study is small and our findings need to be validated in a larger cohort of patients. No patients with dual tachycardias were included in the study and our findings are not applicable in this subgroup. Leads implanted to non-RV apical sites were not included, so the clinical significance of current algorithm in this population is unclear. Only a single manufacturer’s devices were used and by this way a homogeneous patient population could be afforded and observer-related errors could be reduced. Due to single chamber devices, atrial EGM was not available to see AV relationship of the tachycardias. Simultaneous surface ECGs of the episodes was also not available for SVT/VT discrimination.The EGMs of the episodes were evaluated by experts who were blinded to study protocol. Due to lack of EP study data and surface ECGs, this may limit exact discrimination of SVTs and VTs.In patients with extensive LV scar and epicardial VTs may have probably much farther than the usual RV apical lead, and may cause misdiagnosis.The study was retrospective and criteria for ATP programming werenot standardized for all patients. Although potentially useful, in our study onset and stability parameters were turned off or programmed to monitor only. The question if PPI could improve the already existing, multi-parametric, discriminating algorithms, should be further research area.Despite limitations this study is a hypothesis generating study, and will light to further studies on this field.
Our data strongly suggest that the PPI and PPI - TCL parameters may have the potential to be incorporated into ICDs as a method of redetection or dynamic discrimination of the underlying rhythm and a complement to the conventional algorithms. However, a larger study to validate this concept is required.






