Resolution of AV block after ablation for atrial fibrillation
Matthew Glassy1, Nayereh Pezeshkian1, Yingbo Yang1, Uma N Srivatsa1
1Division of Cardiovascular Medicine, UC Davis.
We report a case with complete atrioventricular block (AVB) present both during sinus rhythm and with atrial fibrillation (AF). He had declined pacemaker placement and opted for ablation for the symptomatic AF. He underwent staged hybrid approach with video-assisted thoracoscopic surgical maze (VATS) followed by endocardial ablation. VATS included ganglionic plexi cauterization. One month after the endocardial procedure, he had complete resolution of AF and AVB and remains so at 18 months follow up. We discuss possible abolition of vagal input for this improvement in AV conduction.
Key Words : Vagal denervation, Atrial fibrillation, AV block, Resolution.
Correspondence to: Uma N. Srivatsa, MBBS, MAS, FACC, FHRS 4860 Y street, ste 2820 Sacramento, CA, 95817 Phone: 916-734-3764 Fax: Fax: 916 7348394 Email: unsrivatsa@ucdavis.edu
Association of sick sinus syndrome(SSS) and atrial fibrillation (AF) is well known. Additionally, vagal stimulation evokes bradycardia, and predisposes to atrial fibrillation by the effect on the I kach,ado channels, and a reduction in atrial refractory period respectively.[1]Paroxysmal AF episodes also cause sinus node dysfunction through electrical remodeling.[2]Ablation of AF has been shown to significantly reduce sinus pause and avert pacemaker requirement, [3]however the effect of AF ablation on atrioventricular node (AVN) function is unknown. We report case with resolution of complete atrioventricular block (AVB) after AF ablation.
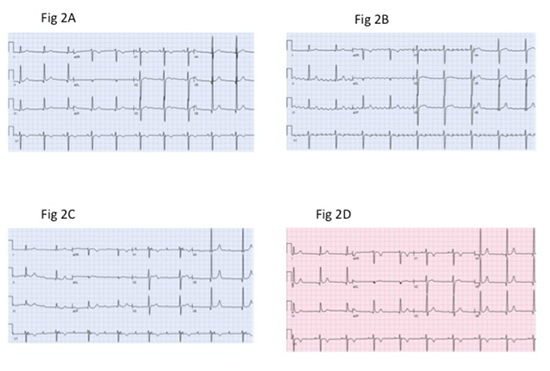
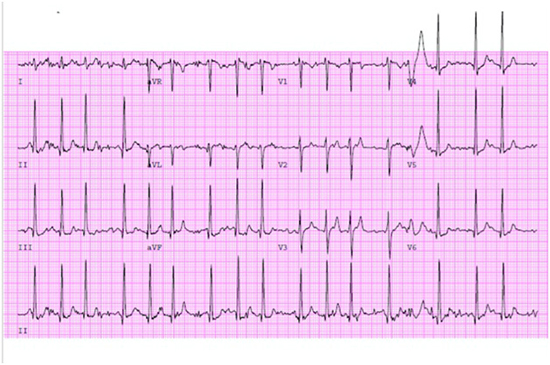
A 64-year-old athletic male presented with exertional fatigue and dyspnea. He has a known history of cavo-tricuspid isthmus dependent atrial flutter with 4: 1 AV block [Figure 1A], which was ablated in 2006 without recurrence. There after he had chronic asymptomatic bradycardia with a prolonged PR interval [Figure 1B] and Wenckebach AV block attributed to high vagal tone, with appropriate increase in heart rate on the treadmill. In June 2011, he reported symptoms of exertional fatigue and palpitations, electrocardiogram (ECG) revealed AF with slow ventricular rate, [Figure 1C] with 60% burden of AF on a 24 hour monitor. When in sinus rhythm, he also had complete AVB with good escape rate. [Figure 1D] Medical management was limited by low heart rate and the pauses noted on the monitor. He declined pacemaker and opted for ABL for AF after 40 months of having paroxysmal episodes. After multiple consultations, opinions and considering various options, he chose to have hybrid ablation with video-assisted thoracoscopic surgical maze (VATS) followed by endocardial ablation. VATS included epicardial pulmonary vein (PV) isolation, ablation of ganglionic plexi, roof and floor of left atrium (LA), right atrial line from SVC to IVC, ligament of Marshall (LOM) disconnection and left atrial appendage ligation. On post-operative day one, electrocardiogram (ECG) revealed transient resolution of AVB [Figure 2A], with subsequent paroxysmal atypical atrial flutter and complete AVB [Figure 2B][Figure 2C]. Nine weeks later, he underwent endocardial mapping (CARTO 3 system, Pentarray Nav Eco mapping catheter) and ablation (Navistar RMT 3.5 mm). He required isolation of one anterior connection in left superior pulmonary vein. The atypical flutter involved mitral isthmus, which terminated during ablation into sinus rhythm with transient Wenckebach AV block; it was confirmed to be at the level of AV node. The gap in roof line was reinforced and septal line to mitral annulus completed to eliminate fractionated signals. [Figure 3] During the first week he remained in Wenckebach AV block, however AV conduction normalized at one month follow up. He has remained in sinus rhythm with normal PR interval without recurrence of AF or atrial flutter after 18 months. [Figure 2D] Exercise stress test on the treadmill revealed an appropriate increase in heart rate with normal PR and Wenckebach AVB with longest PR 200 msec at peak exercise. [Figure 4] He continues to exercise without any limitations.
Figure 1. Preoperative electrocardiograms.A-Atrial flutter with 4: 1 block; B-Sinus Bradycardia with prolonged PR interval; C – Atrial fibrillation with bradycardia; D- Normal sinus rhythm with complete heart block and AV dissociation.
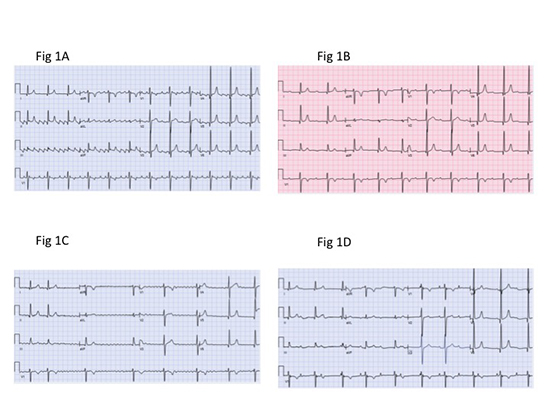
Figure 2. Post operative electrocardiograms.A-Normal sinus rhythm on post operative day one; B- Atypical flutter with complete heart block; C- Normal sinus rhythm with complete heart block and AV dissociation; D- Normal sinus rhythm with normal PR interval post endocardial ablation.
We have described a case of resolution of high-degree AVB after sequential epicardial and endocardial ablations for AF.He is known to have reduced AVN function as observed by 4: 1 block with atrial flutter and baseline complete AVB, in the absence of rate controlling agents.
AVN is richly innervated with cholinergic nerve terminals, with higher density compared to surrounding structures; on the other hand sympathetic innervation at AVN is similar to that of other locations.[4]The parasympathetic nerve terminals at the AVN receive input from the vagi through ganglionic plexi located in the epicardial fat pads.In the canine heart, AV node obtains signals from right and left vagi via ganglionic projections around right and left superior pulmonary veins respectively.[5]In a study among surgical patients, the stimulation of fat pad around right inferior pulmonary vein was found to cause block in the AV node and refractoriness of the surrounding atrial myocardium suggesting a pathway from right vagus.[6]
Figure 3. Electroanatomical map ( CARTO, Biosense Webster Inc) of left atrium PA view. Red color represents low voltage areas in sinus rhythm. Superior and inferior white arrows represent roof and mitral isthmus lines during endocardial ablation.
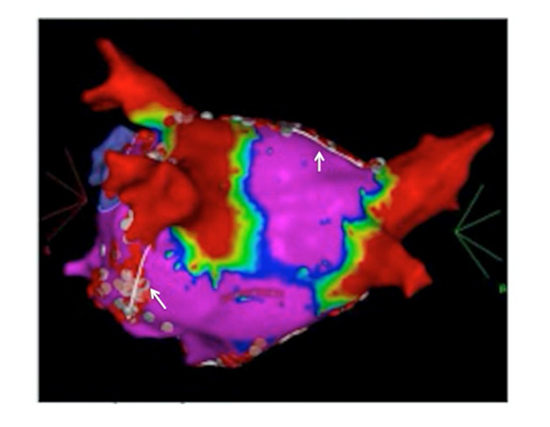
Figure 4. ECG recorded during exercise treadmill test - sinus tachycardia with normal PR interval with 3: 1 Wenckebach AV block.
In patients undergoing epicardial ablation for AF, Xhaet et al showed that ablation of posterior epicardial fat pads leads to a loss of vagal effect at the AVN demonstrated by lack of ventricular slowing with high frequency stimulation.[7]While ablation of the anterior right ganglionic plexus (ARGP) located near the sinus node has been shown to attenuate the vagally mediated slowing of ventricular rate, the combined ablation of ARGP and left inferior ganglionic plexus (LIGP)is needed to eliminate the ventricular slowing caused by vagal stimulation, thus emphasizing the significance of left sided parasympathetic terminals.[8] In addition, the LOM ablation attenuated the ventricular slowing response caused by stimulation of the left superior ganglionic plexus (LSGP). LIGP and LSGP are located near the atrial junction of the left inferior PV and left superior PV respectively, which along with LOM complete the epicardial portion of the mitral isthmus and its extension to the upper ridge. Thus these endocardial areas are likely important conduits for the parasympathetic inputs from left vagus.
In our patient ganglionic plexi around the pulmonary veins and LOM were ablated epicardially and absence of aystole or bradycardia on high frequency stimulation post ablation was confirmed during surgery. After epicardial ablation, on post operative day one, there was a transient resolution of AV block, which recurred later through the hospital stay. During endocardial ablation, besides reinforcement of roof and left superior PV isolation and septal fractionated areas, mitral isthmus was ablated for the atrial flutter. Though there was a transient resolution of AVB after epicardial ablation, the complete resolution subacutely after endocardial ablation could represent a need for both endocardial and epicardial approaches to cause transmural elimination of nerve terminals at the mitral isthmus from the left vagus.
After eighteen months, he has normal AV conduction at rest with an excellent exercise capacity, and a mild degree of Wenckebach AVB at heart rate > 100/min. To our knowledge this is the first case to show significant improvement in AVN function of AF ablation. The effect on AVN function in AF ablation, mediated by elimination of parasympathetic terminals needs to be further investigated.






