Biomarkers of Myocardial Injury and Inflammation after Permanent Pacemaker Implantation: The Lead Fixation Type Effect
Dimitrios Varvarousis1, Nikolaos Goulas1, Kali Polytarchou2, Stavroula N. Psychari1, Konstantinos Paravolidakis1, Agapi Konstantinidou1, Dionysios Tsoukalas1, Delia Vlad1, Konstantina Bouki1, Athanasios Kotsakis1
12nd Department of Cardiology, General Hospital of Nikea-Piraeus “Agios Panteleimon”, D. Mantouvalou 3, 18454, Piraeus, Greece.21st Department of Cardiology, Evagelismos General Hospital of Athens, Ipsilantou 45-47, 10676, Athens, Greece.
Permanent pacemaker implantation is accompanied by minor myocardial damage, indicated by elevated serum levels of cardiac biomarkers. Aim of this prospective study was to comparably investigate the lead fixation type effect on the extent of myocardial injury and inflammation following pacemaker implantation, and to assess the possible clinical implications.
Cardiac troponin I (cTnI) and C-reactive protein (CRP) were measured at baseline, 6 and 24h after implantation in 101 patients, categorized into the active and passive lead fixation group. Patients were followed up for clinical adverse events or abnormal pacing parameters at 24h, 7 and 30 days post-procedure.
cTnI increased at 6h post-procedure (p<0.05) in 23.8% of patients, and returned to baseline after 24h. The passive group demonstrated significantly higher cTnI at 6h compared to the active group (p=0.006). CRP increased significantly at 6h, and maintained an upward trend after 24h (p<0.01) in both groups. The active group demonstrated significantly higher CRP at 6h compared to the passive group. We did not identify an association of positive biomarkers with adverse events.
cTnI and CRP can increase early after permanent pacemaker implantation, indicating mechanical myocardial injury and inflammation. The extent of these biomarkers elevation depends on the lead fixation type, and is not related to worse short-term prognosis.
Key Words : Pacemaker, Lead fixation, Troponin, C-reactive protein.
Correspondence to: Dimitrios Varvarousis
D. Mantouvalou 3, 18454 Nikea, Piraeus, Greece
Permanent pacemaker implantation is accomplished by transvenous insertion of endocardial leads, whose stability is secured and maintained using either active or passive fixation. A number of studies have demonstrated that the mechanical effect of both lead fixation types on the myocardium may lead to local injury, as evidenced by raised levels of plasma troponin and inflammatory biomarkers[1-9,12]. However, data are scarce regarding the association of the lead fixation type (active or passive) with the extent of myocardial injury, the subsequent systemic inflammatory response, and the possible clinical significance of cardiac biomarkers elevation, as clinical adverse events or abnormal change in pacing parameters. Aim of this prospective study was to comparably investigate the lead fixation type effect on the extent of myocardial injury and inflammation following permanent pacemaker implantation, by means of alterations in cardiac troponin I (cTnI) and C-reactive protein (CRP) plasma levels, and to assess the possible clinical impact of this phenomenon.
This was a prospective study, including consecutive adult patients, who underwent permanent pacemaker implantation for symptomatic bradyarrhythmia therapy in our institution. Indications for permanent pacing therapy included sick sinus syndrome, atrioventricular block and slow atrial fibrillation. All patients enrolled in the study were required to have normal baseline cTnI and CRP levels prior to the procedure. Exclusion criteria were unstable coronary artery disease, recent percutaneous coronary intervention, electrophysiological testing or cardioversion within the previous month and patients with temporary pacemaker, signs of any acute infection or chronic inflammatory disease, acute kidney injury or end-stage renal disease. Patients receiving cardiac resynchronization therapy pacing devices were also excluded. The study protocol was approved by the local scientific committee for human research conforming to the ethical guidelines of the 1975 Declaration of Helsinki. All patients gave informed written consent prior to inclusion into the study.
An echocardiographic study was performed to all patients prior to the procedure, for the assessment of left and right ventricular function. All implantation procedures were performed by trained, experienced physicians, ordinarily involved in cardiac pacing therapy, and took place in the relevant operation room of our institution, following our usual protocol for pacemaker implantation. Patients received active (Vitatron Crystalline® Actfix ICQ09B, Vitatron BV, The Netherlands) or passive fixation leads (Vitatron Crystalline® ICM09B/09JB, Vitatron BV, The Netherlands) according to the operators’ judgment. Steroid eluting leads were used in all patients. In case of dual-chamber pacemaker implantation, patients received passive fixation atrial leads in the right atrial appendage, with the only exception of previous cardiac surgery, in consideration of the altered atrial anatomy. In case of use of active fixation atrial leads, the active fixation system was also chosen for the ventricular lead. Patients were categorized into the passive or active group, according to the ventricular lead fixation type. The procedure duration was also recorded and was defined as the time interval between the insertion of the first lead into the cephalic or the subclavian vein and the fixation of the pulse generator.
Blood samples were collected from each patient from a peripheral vein before the beginning of the implantation procedure (baseline values), and at 6 and 24 hours after the end of it. All blood samples were analyzed immediately upon receipt by the biochemical laboratory. Cardiac troponin I and CRP levels were measured by immunoassay technique (cTnI assay troponin I Flex and C-reactive Protein Extended Range Flex) on a Dimension RxL Max analyzer (Siemens Dade Behring, USA). The upper reference limit for cTnI is<0.1 ng/ml and for CRP <5 mg/L.
All patients were monitored for 24 hours after the procedure for clinical signs of myocardial ischemia, hemodynamic instability or any early complication related to the procedure (pneumo- or haemothorax, cardiac tamponade/perforation, haematoma, lead dislodgement, signs of infection, venous thrombosis), and were regularly followed-up at 7 days and at 1 month. Any complication or abnormal change in pacing parameters was also recorded.
Data are expressed as proportions, mean ± standard deviation (SD) and median as appropriate. Student’s t-test was applied to continuous variables with normal distribution, whereas non-parametric analyses were applied to variables demonstrating non-normal distribution. Qualitative variables and differences in ratios between the two groups were assessed with the use of chi-square test. The level of statistical significance was set at a=0.05. All statistical analyses were performed using SPSS version 16 (SPSS Inc., Chicago, IL, USA) software.
A total of 164 patients were enrolled in the study, from which 63 were excluded. The final study population meeting inclusion/exclusion criteria consisted of 101 patients (62 males and 39 females). The average age of the studied population was 78±7 years. Study demographic and clinical characteristics are presented in detail in [Table 1]. Only 4 patients (3.96%) received active fixation atrial (and ventricular) leads. Echocardiographic parameters were similar between the two groups. The use of passive lead fixation was accompanied by a more prolonged procedure duration compared to active, a difference that was found marginally statistically significant (p=0.055).
Table 1. Patients’ clinical characteristics and procedural technical variables.
|
Passive Fixation (n=62) |
Active Fixation (n=39) |
p-value |
| Age (years) |
79.27 ± 7.56 |
77.64 ± 7.88 |
ns |
| Male sex, n (%) |
41 (66.1) |
21 (53.9) |
ns |
| Procedure duration (minutes) |
32.5 ± 17.14 |
26.41 ± 9.79 |
ns |
| Pacemaker type |
|
|
|
| -Dual chamber, n (%) |
44 (71) |
28 (71.8) |
ns |
| -Single chamber, n (%) |
18 (29) |
11 (28.2) |
ns |
| Indication for permanent pacing |
|
|
|
| -Sick sinus syndrome, n (%) |
23 (37.1) |
15 (38.5) |
ns |
| -Atrioventricular block, n (%) |
21 (33.9) |
13 (33.3) |
ns |
| -Bradyarrhythmia - atrial fibrillation, n (%) |
16 (25.8) |
10 (25.6) |
ns |
| -Other, n (%) |
2 (3.2) |
1 (2.6) |
ns |
| Approach: |
|
|
|
| -Cephalic vein, n (%) |
24 (38.7) |
16 (41) |
ns |
| Clinical adverse events, n |
|
|
|
| -Clinical signs of myocardial ischemia |
0 |
0 |
ns |
| -Early complications related to the procedure |
1 |
2 |
ns |
| -Abnormal change in pacing parameters |
4 |
3 |
ns |
Data are presented as mean ± standard deviation and percentages. ns = non-significant
Biochemical data are presented in [Table 2]. Baseline values of cTnI and CRP were within normal limits without differences between active and passive lead fixation groups. Plasma cTnI increased at 6h post-procedure (p<0.05) in 23.8% of patients, and returned to baseline after 24h in both groups [Figure 1]. Of note, one patient of the passive lead fixation group had a marked increase in serum cTnI level at 6h (1.74 ng/ml), a value that also declined after 24h back to normal [Figure 1]. The passive fixation group demonstrated significantly higher cTnI at 6h compared to the active fixation group (p=0.006, [Table 2]), a discrepancy that was not maintained at 24h (p=0.452). Plasma CRP increased significantly at 6h, and maintained an upward trend after 24h (p<0.01) in both groups. Statistical analysis yielded a significant difference (p<0.05) between the two study groups at 6h, with the active group demonstrating higher CRP levels compared to the passive group [Table 2]. A total of 5 patients (3 in the active and 2 in the passive group) demonstrated marked elevation in CRP levels (above 20 mg/dl), although this was not related to cTnI values.
There was no correlation between elevated cTnI or CRP levels with demographic, clinical or technical aspects, including age, sex, pacemaker type (single or dual chamber), procedure duration, echocardiographic parameters and implantation approach (p=non-significant).
There was no clinical suspicion of myocardial ischemia, by means of chest pain or anginal equivalent in any patient, and all patients remained hemodynamically stable post-procedure. A total of 3 complications were identified in the post-procedural phase, one patient from the active group with pneumothorax and two patients with lead displacements, recognized at 24h (1 patient from the active and 1 from the passive group). Moreover, there were 7 patients showing significantly increased pacing thresholds during follow-up, from which only 2 patients have had elevated cTnI levels after the implantation. Thus, no correlation could be found between these adverse events and elevated cTnI/CRP levels or study group (active/passive).
Figure 1. Correlation of the change in cTnI plasma levels from baseline to 6h with their change from 6 to 24h, for the active and passive lead fixation group.
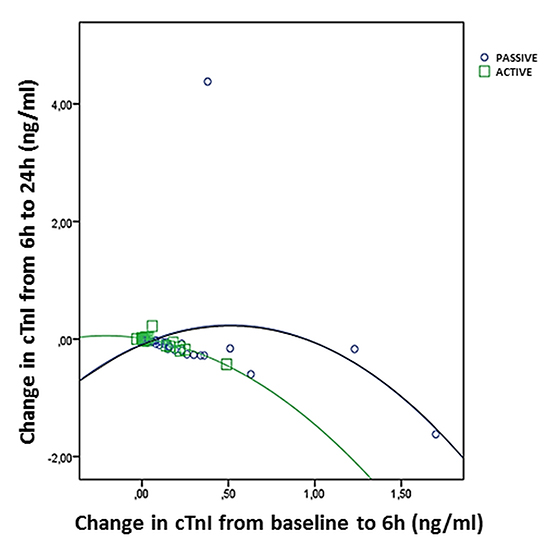
Table 2. Serial changes of cTnI and CRP plasma levels.
|
Passive Fixation |
Active Fixation |
p-value |
| cTnI (normal value <0.1 ng/ml) |
|
|
|
| -Baseline |
0.05±0.02 (0.04) |
0.04±0.01 (0.04) |
ns |
| -At 6h |
0.21±0.3 (0.11) |
0.1±0.11 (0.05) |
0.006 |
| -At 24h |
0.2±0.68 (0.06) |
0.08±0.07 (0.05) |
ns |
| CRP (normal value <5 mg/L) |
|
|
|
| -Baseline |
2.81±1.49 (2.5) |
3.13±1.89 (2.4) |
ns |
| -At 6h |
7.21±7.19 (4.55) |
14.29±20.41 (7) |
0.032 |
| -At 24h |
16.29±16.84 (14.3) |
15.32±9.55 (13.3) |
ns |
Data are presented as mean ± standard deviation and percentages. ns = non-significant
The important findings of this prospective study are the confirmation that permanent pacemaker implantation can be associated with an early detectable rise of cardiac biomarkers, indicative of reversible mechanical myocardial injury and inflammation, and the demonstration that the pacing lead fixation type seems to be related to the extent of this phenomenon. Our findings are in line with other similar clinical studies which have reported transient increases in cardiac troponin after elective permanent pacemaker implantation[1-4,6,10].
Rapid increase and decrease in cardiac troponin plasma levels are characteristic of reversible myocardial mechanical injury, especially due to the physical contact between lead and endocardium, resulting in direct cardiomyocyte destruction during the implantation procedure[1,2]. A small percentage of troponin is found in the myocyte cytoplasm in a soluble free form, which is released into the circulation under such circumstances[5]. A rapid troponin washout occurs within 24 hours, as there is no obstructive myocardial blood flow[3,4,6]. As we did not identify any association with clinical adverse events, cardiac troponin elevation seems not to be of clinical importance. However, high sensitivity troponin loses its specificity and the early post-procedural period has to be considered diagnostically “blind”[1]. An acute rise of cardiac troponin occurring in this period may raise clinical concern regarding the differential diagnosis of an acute coronary syndrome, tachyarrhythmias, cardiac perforation, pulmonary embolism or direct coronary artery trauma[11].
Concerning the effect of the lead fixation type on the extent of this phenomenon, the type of lead fixation seems to be related to differences in troponin release. Contrary to previous studies[1] and to what one might expect, we have demonstrated that actively fixed leads result in less evident troponin release compared to passive leads, despite the fact that they are screwed into the myocardium[1]. This interesting finding could possibly be attributed to the greater number of lead manipulations and repositioning attempts needed until satisfactory final lead lodgement in passive fixation systems. This hypothesis is further supported by our finding of slight prolongation of the procedure duration using passive, as compared to active fixation leads. Consequently, it is reasonable to assume that the extent of troponin elevation after pacemaker implantation strongly depends on technical procedural issues, as reflected possibly by more prolonged procedure duration.
Furthermore, according to our data, progressively elevating CRP plasma levels illustrate the systemic, non-infectious, inflammatory response following pacemaker implantation. The significantly greater and earlier acute CRP rise of the more traumatic active compared to passive fixation leads corroborates the hypothesis of the primary regional inflammatory response, stimulated by the electrode contact with the endocardium[1,12].
Finally, in this study we attempted to address whether elevations in cardiac biomarkers following pacemaker implantation are linked to worse short-term prognosis. However, we could not identify any relation of increased biomarkers with procedure-related complications, lead displacement or rise in pacing threshold during a 1-month follow-up period. Consequently, this elevation in plasma cardiac biomarkers most likely represents the minimal myocardial damage that occurs during device implantation and seems not to be of clinical importance[13,14].
Our study included a relatively small sample size and that allocation of patients into the active or passive lead fixation group was not completely randomized. Moreover, we did not include a control group of patients undergoing pacemaker device replacement, in order to draw safer conclusions with regard to the effect of the surgical preparative manipulations, such as device pocket formation, on CRP elevation. Finally, this study was underpowered to investigate possible clinical implications of elevated biomarkers.
Permanent pacemaker implantation results to mechanical myocardial injury, as indicated by elevated cTnI plasma levels during the early post-procedural phase, a phenomenon that seems to be related to the lead manipulations during pacing lead fixation. The systemic inflammatory response seems to be more pronounced in active lead fixation systems.






