Catheter Ablation for Persistent Atrial Fibrillation in Class IV Systolic Heart Failure: A Single-Center Case Series
Aaron Hesselson1*, Heather Hesselson2
1University of Kentucky Division of Cardiovascular Medicine, 900 South Limestone Street, CTW 305D, Lexington, KY 40536.2University of Kentucky, College of Pharmacy, 789 S Limestone, Lexington, KY 40508.
Questions remain as to how aggressively catheter ablation for atrial fibrillation may be applied to patients with advanced systolic congestive heart failure, owing to a historic under-representation in multicenter clinical ablation trials. We sought to describe the experience of catheter ablation for persistent atrial fibrillation in Class IV systolic heart failure patients at our institution. All Class IV systolic heart failure patients (left ventricular assist device patients excluded) between 2017 and 2020 referred for radiofrequency ablation were included. Out of 10 patients, 7 agreed to proceed, had restoration of normal sinus rhythm upon completion of the catheter ablation procedure, and of which five (71%) remain in normal rhythm at a mean follow-up of 23 months. Catheter ablation for atrial fibrillation in patients with Class IV chronic systolic heart failure, even on advanced heart failure therapies, is feasible, and can improve heart failure status with maintenance of NSR.
Key Words : Atrial Fibrillation, Catheter Ablation, Heart Failure.
Aaron B. Hesselson, MD, BSEE, FACC, CCDS, Director, Electrophysiologic Services, University of Kentucky Division of Cardiovascular Medicine, 900 South Limestone Street, CTW 305D, Lexington, KY 40536
Despite multiple observational and recent clinical trials supporting the efficacy of catheter ablation (CA) of atrial fibrillation (AF) for restoration of normal sinus rhythm (NSR), patients with Class IV systolic congestive heart failure remain under-represented [1]-[16]. Questions therefore remain regarding how aggressively ablation may be brought to bear in left ventricular systolic dysfunction (LVSD) and which operators should perform it? Additionally, there has been no prior report in the literature describing ablation in a cohort consisting only of Class IV systolic congestive heart failure (CHF) patients, including those on advanced therapies such as continuous ambulatory milrinone. We sought to address these issues by describing our experience for AF ablation in such patients.
We included all patients referred and who agreed to CA of persistent AF with Class IV systolic heart failure at our institution between 2017 and 2020 in this case series. Patients with a left ventricular assist device (LVAD) were excluded. Records were reviewed for history, medication management, electrophysiologic study results, with particular attention to clinical course after CA. [Table 1] summarizes the cohort characteristics and ablations performed. All had failed previous trials of amiodarone and cardioversion for rhythm control, and were on guideline-directed medical therapy (GDMT) for heart failure management. Informed consent was obtained on all patients prior to their CA procedure, and the study was approved by the University of Kentucky institutional review board.
Table 1. Patient Characteristics
| Case |
Sex (M/F) |
Age (y) |
Cardiomyopathy Type/Comorbidities |
EF/CO(L/min)/CI(L/min/m2) |
LA Volume (ml/m2) |
Duration of Continuous AF at Ablation |
Pre-procedure advanced CHF Rx |
Ablation(s) |
Follow-up |
| 1 |
M |
61 |
Ischemic/DM, HTN, ICD, OSA |
10%/NA |
68 |
3 months |
GDMT, DREAM HF Study |
WACA→PWI→LAF→PML→RAF→CTI→NSR |
42 months |
| 2 |
M |
43 |
Non-ischemic/DM |
20%/2.68/1.3 |
42-48 |
6 years |
GDMT, Milrinone 0.25mcg/kg/min |
WACA→PWI→CV→NSR |
31 months
|
| 3 |
M |
60 |
Non-ischemic/HTN, ICD |
12%/3.62/1.5 |
35-41 |
4 months |
GDMT, Milrinone 0.25 mcg/kg/min |
1) WACA→LAF→PML→RAF→CTI→NSR
2) NSR→Re-isolate RSPV |
29 months |
| 4 |
M |
66 |
Ischemic/DM, HTN, ICD |
30%/2.96/1.4 |
>48 |
4 months |
GDMT, Milrinone 0.125 mcg/kg/min |
WACA→LAF1→PWI→LAF2→AML→NSR |
5 months (deceased) |
| 5 |
M |
76 |
Ischemic/HTN, ICD |
10%/3.20/1.5 |
35-41 |
18 months |
GDMT, Milrinone 0.375 mcg/kg/min |
WACA→PWI→CV→NSR
Inducible AT→NSR
|
5 months(deceased) |
| 6 |
F |
77 |
Non-ischemic/DM, HTN, ICD |
20%/2.35/1.2 |
>48 |
7 years |
GDMT, Milrinone 0.25 mcg/kg/min |
WACA→PWI→LAF→PML→”slow” AF→CV→NSR |
12 months |
| 7 |
M |
60 |
Ischemic/DM, HTN, ICD |
40%/4.66/2.3 |
<35 |
4 months |
GDMT |
WACA→CTI→NSR |
5 months |
AF=atrial fibrillation, AML= anterior mitral line, AT= atrial tachycardia, CHF=congestive heart failure, CI=cardiac index, CO=cardiac output, CTI=cavo-tricuspid isthmus, CV=cardioversion, DM=diabetes mellitus, EF=ejection fraction, F-female, GDMT=guideline-directed medical therapy, HTN=hypertension, ICD=implantable cardiac defibrillator, LA=left atrium, LAF=left atrial flutter, M=male, NA=not applicable, NSR=normal sinus rhythm, OSA=obstructive sleep apnea, PML=posterior mitral line, PWI=posterior wall isolation, RAF=right atrial flutter, RSPV=right superior pulmonary vein, Rx=prescription, WACA=wide area circumferential ablation
All electrophysiologic studies (EPS) were performed as outpatient under general anesthesia with continuous invasive radial arterial blood pressure monitoring, and no discontinuation of GDMT, amiodarone, or inotropic agents. Procedural expectations were addressed between anesthesia and electrophysiology attendings with the patient in a shared discussion. Vasopressor (VP) agents were directed by anesthesia services, however upward titration of milrinone was done at the discretion of the attending electrophysiologist. Three-dimensional mapping of the left atrium was performed at the beginning of each procedure. Radiofrequency ablation was accomplished with a 3.5 mm irrigated contact force ablation catheter, a double trans-septal technique, and by personnel with a 2000+ experience with CA for AF. An intra-cardiac echocardiography catheter remained deployed throughout. Ablation parameters for WACA and posterior wall isolation (PWI) have previously been described [14]. CA consisted of a step-wise approach:
1) Wide area circumferential ablation (WACA) of the pulmonary veins, carinal lines allowed
2) Posterior wall isolation (PWI) only if remaining in AF after WACA with roof and inferior wall lines
3) Ablation of spontaneously converted rhythms at any step in the process. Increased power titration up to 40 Watts allowed for atrial flutter
4) Cardioversion if remaining in AF after WACA and PWI
5) Ablation of inducible focal or reentrant rhythms post initial ablation both off and on 10 mcg/min isoproterenol infusion with atrial programmed stimulation, and atrial burst pacing from a cycle length of 300 ms down to 200 ms.
All reentrant rhythms were ablated with a combination of activation mapping with entrainment confirmation. In instances of multiple critical isthmus targets being available, the chosen ablation path was individualized after mapping in each patient. Bi-directional block was confirmed with differential pacing across the ablation lines. Each patient received a single bolus of furosemide 60 mg intravenously at study completion. Post-CA plans were for a telemetry unit recovery and discharge the following day. All received amiodarone 200 mg daily on discharge. Electrophysiology (EP) follow-up was coordinated with the heart failure service and consisted of a 1-week phone call, 1-month EP visit, and 3-month EP/heart failure follow-up initially. Further follow-up consisted of every 6-month visits, or phone check allowing for difficulties in distant travel. Adjustment of inotropic therapy or GDMT occurred at the discretion of the heart failure service.
Specified data endpoints included procedure duration, VP utilization, minimum MAP (mMAP), average procedural urinary output > 100 ml/hour, length of stay, 30-day re-hospitalization, and longest time of continuous intervention (LTCI). A VP intervention was an instance of VP bolus in time or initiation/titration up or down of a VP drip. LTCI was defined as the longest time period of VP bolus and/or drip titration before a 5 minute charting gap not requiring an intervention was reached.
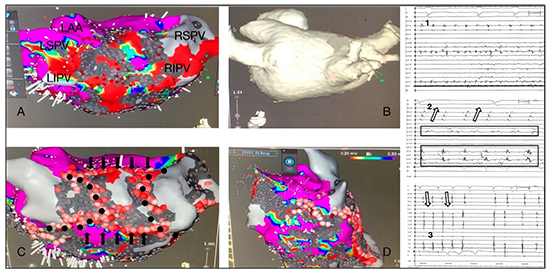
A 61-year-old male with prior history of paroxysmal AF, previously enrolled in the DREAM-HF mesenchymal cell study [17] for Class III chronic systolic heart failure, and on chronic daily amiodarone self-referred early to EP clinic with severe fatigue, resting shortness of breath, and increased ankle swelling consistent worsening to Class IV status. Interrogation of his implantable cardiac defibrillator (ICD) showed AF that had been persistent for 3 months. Hypotension did not allow further titration of rate controlling medications, and cardioversion did not maintain NSR. CA for AF was scheduled. Initial left atrial voltage mapping in AF showed diffuse areas of low/absent voltage suggesting scar ([Figure 1], panel A). WACA had no effect on AF. During PWI the AF organized into a clockwise peri-mitral flutter with prolonged conduction into the posterior wall before isolation ([Figure 1], panel 2). A posterior mitral ablation line ([Figure 1], panel D) converted the rhythm to a typical counter-clockwise right atrial flutter. A cavo-tricuspid isthmus (CTI) ablation converted flutter to NSR ([Figure 1], panel 3). Follow-up at 3 months was notable for resolution of resting symptoms and improvement in objective findings without change in medical therapies, save discontinuation of amiodarone. Interrogation of the ICD has been notable for a rare non-sustained atrial tachycardia of a few seconds duration without use of any anti-arrhythmic agent. Follow-up echocardiographic findings are unknown due to blinding from his heart failure research trial.
Figure 1. Case 1: Panel A: The initial bipolar voltage map (posterior left atrium) in atrial fibrillation (AF) demonstrating generous low voltage (threshold 0.2 mV) and scar (threshold 0.03 mV). Panel B: Posterior left atrium CT scan. Panel C: Path of WACA (black dots), and roof/inferior wall ablation (black arrows). Panel D: Caudal left lateral left atrium showing voltage map and posterior mitral line ablation lesion set (circle) consolidating an area of scar and low voltage. Panel 1: Baseline AF, Panel 2: clock-wise peri-mitral flutter during posterior wall isolation; arrow shows distal to proximal coronary sinus activation, and boxes prolonged fractionated signals within the posterior wall measured from a 20-pole circular catheter. Panel 3: Typical counter-clockwise (proximal to distal coronary sinus activation) right atrial flutter terminates with isthmus ablation. LAA=left atrial appendage, LIPV=left inferior pulmonary vein, LSPV=left superior pulmonary vein, RIPV=right inferior pulmonary vein, RSPV=right superior pulmonary vein
A 43-year-old male with at least 6 years of long-standing persistent AF was transferred from out of state for advanced heart failure therapy, including work-up for transplant candidacy. Previously, NSR could not be maintained on amiodarone 200 mg daily following loading and despite “numerous” cardioversions. Milrinone was initiated as well as oral anti-coagulation. He was not a candidate for surgical management of severe mitral regurgitation. Initial EP consult suggested an atrio-ventricular nodal ablation with bi-ventricular ICD for AF with rapid response. A second EP consult offered short-term return for CA of AF after discharge. EP study was initially notable for lack of scar/low voltage in the left atrium. He remained in AF despite WACA and PWI. Cardioversion returned NSR. Follow-up echocardiography 3-months later showed an improvement in ejection fraction (EF) to 45-50% with “trace” mitral regurgitation.Milrinone was discontinued. He remains well in NSR, and reluctant to stop amiodarone >2 years later.
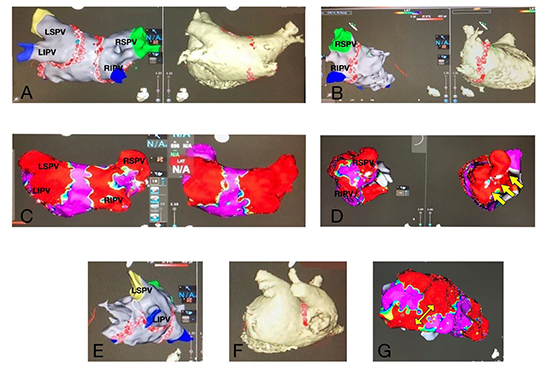
A 60-year-old male was referred by the heart failure service for persistent AF with rapid response management, and agreed to CA. Partial ablation around the left pulmonary veins converted AF to a counter-clockwise peri-mitral flutter. WACA was completed ([Figure 2], panel A), and a posterior mitral ablation line ([Figure 2], panel E) converted the rhythm to a CTI counter-clockwise flutter. CTI ablation converted flutter to NSR. Milrinone and amiodarone were discontinued at 3-month follow-up. The EF improved from baseline, yet was significantly depressed (20-25%). A primary prevention ICD was implanted. Near 1-year follow-up from initial CA he had worsened shortness of breath and fatigue. ICD interrogation showed frequent episodes of AF hours to weeks at a time. Milrinone was restarted. Repeat EP study showed an opening in the ablation line around the right superior pulmonary vein that was easily re-isolated ([Figure 2], panels C+D). Bi-directional block remained across the prior flutter lines ([Figure 2], panel G posterior mitral line). Milrinone was discontinued at follow-up due to absence of AF on ICD interrogation and improvement in hall walk test. Repeat echocardiogram 4 months after repeat ablation demonstrated an ejection fraction improvement to 45%. Remote and in-clinic ICD evaluations show maintenance of NSR > 1 year from second ablation.
Figure 2. Case 3: Panels: A; Posterior left atrium, B; Right lateral left atrium, E and F; Left lateral left atrium showing ablation and CT anatomy from index procedure. Panels: C; Posterior left atrium and D; Right lateral left atrium showing bipolar voltage maps before (left) and after re-isolation (right). The yellow arrows point to the area of ablation. Panel G: Left lateral voltage map from the repeat ablation displaying the durable posterior mitral ablation line. Note lack of low voltage (threshold 0.2 mV) outside of ablation aspects on all maps. LIPV=left inferior pulmonary vein, LSPV=left superior pulmonary vein, RIPV=right inferior pulmonary vein, RSPV=right superior pulmonary vein.
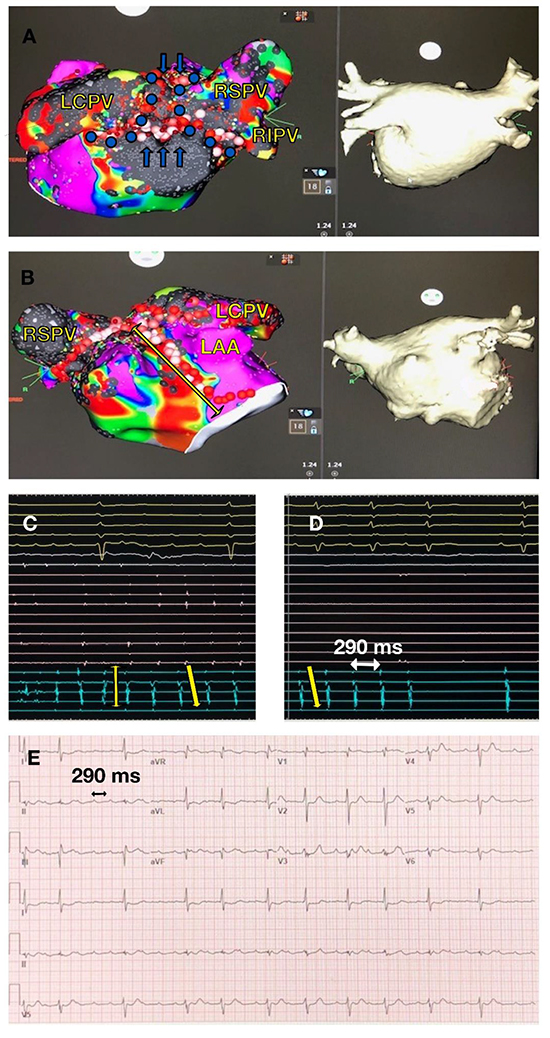
A 66-year-old male with persistent AF was referred by the heart failure service for management. CA was agreed to be the next best management option. Diffuse posterior wall scarring was noted with initial mapping ([Figure 3], panel A). During WACA, AF converted to an atypical flutter that utilized the posterior wall ([Figure 3], panel C). PWI converted this to a counter-clockwise peri-mitral flutter, and an anterior mitral line terminated the flutter to NSR ([Figure 3], panel D). The CA was otherwise remarkable for brief hypotension early in the procedure that resolved after up-titration of the milrinone. The milrinone rate was returned to the pre-procedure setting before proceeding to recovery. ICD interrogation at the 3-month follow-up showed no arrhythmia events and he had subjective improvement in symptoms. Milrinone was stopped. Subsequent demand remote monitoring initiated by the patient a few days later showed initiation of atrial flutter starting hours after the 3-month follow-up visit ([Figure 3], panel E). Milrinone was restarted shortly thereafter. Elective plans were made for repeat ablation due to persistence of the atypical flutter, however were cancelled due to a spontaneous intra-cranial hemorrhage while on both apixiban and clopidagrel. He convalesced, and neurology service subsequently approved restarting the apixiban only. The patient was re-admitted shortly after with a second spontaneous intra-cranial hemorrhage and expired.
Figure 3. Case 4: Panel A: Bipolar voltage map and CT scan of posterior left atrium in AF. Highlighted blue dots and arrows represent WACA and roof/inferior wall ablation lines respectively. Note generous dense scar (threshold 0.03 mV) and low voltage (threshold 0.2 mV). Panel B: Bipolar voltage map and anterior mitral ablation line (yellow arrow) with CT anatomy. Panel C: AF converts to organized flutter (vertical and diagonal arrows) that occasionally utilize posterior wall during WACA. Panel D: Counterclockwise peri-mitral flutter only after PWI isolation (pink signals) that terminates to NSR with anterior mitral ablation line. Panel E: 12-lead ECG 4 months post-CA with atypical flutter at same cycle length as peri-mitral flutter at ablation. LAA=left atrial appendage, LCPV=left common pulmonary vein, RIPV=right inferior pulmonary vein, RSPV=right superior pulmonary vein.
A 76-year-old male with rate-controlled long-standing persistent AF presented to EP clinic with a remarkable interval history of milrinone initiation from the heart failure service. His condition had not improved despite up-titration of the milrinone. Given prior failure to maintain NSR on amiodarone, CA was scheduled after an extensive discussion of the risks and perceived potential benefits. He remained in AF following WACA and PWI. Cardioversion returned NSR. He had a sustained right atrial tachycardia induced that was terminated with ablation at the coronary sinus ostium. Amiodarone was continued post-ablation. At 1-month follow-up his condition had not changed and ICD interrogation showed recurrence of AF 3-weeks after CA. He was successfully cardioverted. Four months later he returned for admission due to a hip fracture following a fall. He appeared in AF with bi-ventricular pacing at lower rate on the 12-lead ECG. He became hypoxic while undergoing hip repair, and was resuscitated from a pulseless electrical arrest. However, he developed persistent cardiogenic shock, was made do-not-resuscitate, and expired after withdrawal of care.
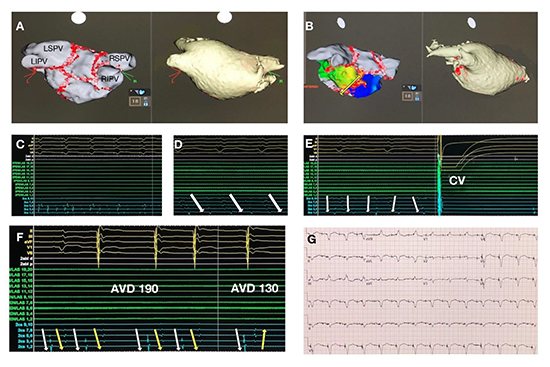
A 77-year-old female with non-ischemic cardiomyopathy and 7 years of long-standing persistent rate-controlled AF was referred by the heart failure service to re-establish ICD management. A detailed rhythm history revealed an EF of 40% at initial discovery of AF, a subsequent pacemaker insertion with atrioventricular nodal ablation, upgrade to a bi-ventricular ICD, and optimization of ICD programming. Worsened symptoms and cardiac function (EF 25%) had prompted ambulatory milrinone. Amiodarone given at initial discovery of the AF did not maintain NSR despite cardioversion. The patient was enthusiastic to proceed with CA given her limited quality of life. Following WACA, PWI converted the AF to a counter-clockwise peri-mitral flutter ([Figure 4], panel D). A posterior-inferior mitral ablation line converted flutter to “slow” AF ([Figure 4], panel E). AF was cardioverted to NSR. The biventricular ICD was reprogrammed for AV optimization ([Figure 4], panel F) based on the near and far-field signals on the diagnostic coronary sinus catheter. A small right groin hematoma was noted at CA completion. It remained stable, and she was observed in the intensive care unit overnight. She was managed with an intravenous saline bolus for a brief drop in blood pressure. Discharge to home occurred later the next day with a stable blood count (Hct 31.3), renal function comparable to baseline (1.97 mg/dL versus 1.86 mg/dL), blood pressure 99/58 (111/50 pre-op) and serial hallway ambulation at baseline. Call-back 5 days later found her to be feeling “good”. She was readmitted 2 weeks after ablation with generalized fatigue, “hypotension” (105/61 mm Hg), and an elevated white blood cell count [15]. Hematocrit was 33.5, creatinine 2.87 mg/dL, NT-proBNP level 1619 pg/mL (normal 0-1700 pg/mL) and urinalysis positive for bacteria. 12-lead ECG showed AV sequential pacing and capture ([Figure 4], panel G). There was no pericardial effusion or access site bleeding. Conservative management with intravenous fluids and antibiotics improved her symptoms. Creatinine dropped to 1.67 mg/dL and she was discharged after 3 days. Four months post ablation the milrinone was discontinued after having been on it for 26 months. Seven months from ablation she remained in normal rhythm with 0% AF burden on ICD interrogation. Subjectively she feels “like a new person”. Her EF improved to 29%.
Figure 4. Case 6: Panel A: Posterior left atrium; 3-dimensional map and CT scan with WACA, PWI, mitral lesion sets. Panel B: Postero-lateral left atrium with activation during counter-clockwise peri-mitral flutter. The yellow arrow shows the chosen ablation path through an area of “early-meets-late” slowed conduction. Panel C: AF remains after WACA (green 20-pole circular catheter signals in left pulmonary veins, blue signals decapolar coronary sinus catheter). Panel D: Counter-clockwise peri-mitral flutter with proximal-to-distal coronary sinus activation following PWI. Panel E: “Slow” AF after mitral ablation line cardioverts to NSR. Panel F: Post cardioversion DDDR 80 bpm sensed AV delay 190 ms. There is insufficient ventricular paced pre-excitation (proximal-to-distal far-field left ventricular signals on coronary sinus catheter, yellow arrows) initially, remedied with shortening the sensed AV delay (distal-to-proximal far-field left ventricular signals on coronary sinus catheter). White arrows represent near-field atrial activity. Panel G: 12-lead ECG at 2 weeks follow-up showing AV sequential capture. AVD=atrio-ventricular delay, CV=cardioversion, LIPV=left inferior pulmonary vein, LSPV=left superior pulmonary vein, RIPV=right inferior pulmonary vein, RSPV=right superior pulmonary vein
A 60 year-old male with chronic ICM, and aortic valve replacement X 2 had EF improved to 40% following insertion of a biventricular ICD in 2019. Over 9 weeks time beginning in April 2020 he was admitted five times for heart failure in the setting of rate controlled persistent AF and typical atrial flutter that had begun in March. He could not maintain NSR despite amiodarone and cardioversion. Right heart catheterization did not support the initiation of ambulatory inotropic therapy. Renal function was notable for a creatinine of 1.14 mg/dL at the beginning of April 2020 that worsened to 3.35 mg/dL by the end of June. Electrophysiology service was agreeable to urgent ablation. WACA and then CTI ablation returned NSR. He remained hospitalized for 8 days to manage pre-procedure fluid overload. Over the course of admission renal function did not worsen and creatinine improved to 2.95 mg/dL by discharge. He has remained arrhythmia free, off amiodarone, to date and has not required titration of GDMT or been re-admitted.
Mean duration of persistent AF entering the CA procedure was 27 ± 35 months. NSR was returned spontaneously with ablation in 4/7 (57%) of the patients. All pulmonary veins were successfully isolated. Bi-directional block was achieved at initial ablation in all atrial flutter instances with endocardial ablation only. Mean procedure time for initial ablations was 175 ± 24 minutes. Six out of 7 patients (86%) required a VP during CA. Case 5 required no VP support. The procedure mMAP was 62 ± 8 mmHg, LTCI 9 ± 2 minutes, and average number of VP interventions per patient 4 ± 2. VP agents were discontinued before leaving the procedure room for all patients. Urinary output average > 100ml/hour was present in each case. Serum creatinine was 1.75 ± 0.80 mg/dL pre-procedure versus 1.77 ± 0.84 md/dL post-procedure (p=NS). Six out of 7 (86%) recovered on the telemetry unit, and all but Case 7 were discharged home the next day. None of the patients required bi-level positive airway pressure during their recovery on the telemetry unit. Follow-up has been 23 ± 15 months for the surviving patients.
[Table II] summarizes the management of amiodarone and rhythm surveillance post-CA.
Table II. Post-Ablation Amiodarone Management and Rhythm Surveillance
| Case |
Amiodarone Management Post-CA |
Rhythm Surveillance |
| 1 |
Discontinued at 3 months |
Q6 month in-person and remote ICD monitoring |
| 2 |
Continued 200 mg daily indefinitely at patient request |
In-person/ambulatory monitoring, telephone follow-up Q6 month |
| 3 |
Discontinued at 3 months |
Q6 month in-person and remote ICD monitoring |
| 4 |
Continued until expiration at 5 months |
In-person and remote ICD monitoring |
| 5 |
Continued until expiration at 5 months |
In-person and remote ICD monitoring |
| 6 |
Discontinued at 3 months |
Q6 month in-person and remote ICD monitoring |
| 7 |
Discontinued at 3 months |
Q6 month in-person and remote ICD monitoring |
CA = catheter ablation, ICD = implantable cardioverter defibrillator, Q = every
Three patients did not to proceed with CA. One 25-year-old with persistent AF and non-ischemic cardiomyopathy wished to continue milrinone and no other intervention. A 45-year-old with chronic non-ischemic cardiomyopathy and 5 years of long-standing persistent AF on milrinone, desired advancement to a left ventricular assist device as a bridge to possible cardiac transplantation. The third, a 63-year-old male with chronic non-ischemic cardiomyopathy, 7 years of long-standing persistent AF and left bundle branch block, was hospitalized for LVAD and transplant work-up. A cardioversion returned NSR, however the heart failure service did not accept electrophysiology recommendation for a staged intervention of biventricular ICD and then ablation. He received an LVAD.
This case series provides insight to questions regarding CA for AF in LVSD that have not previously been answered. CA appeared safe in this cohort. All patients had successful completion of the CA without any apparent difficulty with operative hemodynamic status. All patients except Case 5 required vasopressor support during the ablation. This is consistent with the hemodynamic management during AF CA for any patient at our institution regardless of heart function status (unpublished data). Case 4 had transient up-titration of milrinone to compensate for the presumed negative inotropic effects from the inhaled anesthetic. The infusion drip rate was returned to baseline at procedure’s end. No patient needed any post-ablation blood pressure or respiratory support. There were no significant procedural vascular or bleeding complications despite uninterrupted oral anti-coagulation. The use of ultrasound to assist in procedural vascular access likely contributed to this. All patients remained on anti-coagulation post-CA except for Case 4 due to intracranial hemorrhage. There did not appear to be any significant exacerbation of heart failure status from exposure to the CA process. Only in Case 7 was a patient not discharged home the day after the CA. They did not appear euvolemic pre-procedure, and stayed longer post-ablation at the operator’s discretion to achieve improved volume status in the face of already tenuous renal function.
Procedure times were significantly greater than that of LVSD EF < 40% contemporaries for our institution, 175 ± 24 min. vs. 153 ± 33 min. (p=0.009) (unpublished data), likely driven by the additional need for PWI, typical and atypical arrhythmia ablation. Case 6 was observed in the ICU transiently after CA, treated with an intravenous fluid bolus for brief hypotension, and discharged later the next day after serial re-evaluations. It was successfully managed conservatively with return to baseline status.
The death in Case 5 occurred after a sequence of events prompting an urgent orthopedic procedure that was not tolerated. By contrast the elective CA for which he did not require any VP support at all, had no complications. The death in Case 4 occurred with concomitant dual direct oral anti-coagulation (DOAC) and monotherapy platelet inhibition use. The deaths were not related to the CA, and serve to emphasize the increased mortality of this at-risk population. While many studies for CA in AF and heart failure have included Class IV patients [2],[6],[14],[15], none have provided a focused report for us to provide safety comparisons. One suspects limited numbers, such as at our institution, to be the reason.
Does the procedure actually do what it purports? More specifically, is it efficacious for maintaining NSR, and does it result in improved heart failure status? Overarching conclusions cannot be drawn from our limited experience regarding long-term AF burden reduction. It has been shown that duration of AF before CA is predictive of freedom from AF following CA in larger groups [18]-[20]. Our cohort is heterogeneous as regards duration of AF before CA (3-months to 7-years) and underlying cardiac substrate. We did not exclude anyone for CA consideration based on duration of AF or left atrial size, but did for presence of a LVAD. The likely atypical flutter recurrence in Case 4 may have been managed successfully with a repeat procedure had intra-cranial bleeding not intervened. We chose our step-wise approach for the CA process as an attempt to limit the amount of ablation, given prior trial experience showing potential for worsened outcomes [21]. PWI following WACA was chosen as the second step, absent conversion of AF, given multiple studies suggesting added benefit to pulmonary vein isolation, despite understanding the difficulties with durability [22]-[24] and energy limitations on the posterior wall. Subsequent to initiating our CA process, recent findings have suggested that adjunctive PWI may not have added benefit in a broader group of persistent AF [25]. The potential need for repeat ablation should be expected.
No study to date has reported the concomitant application of CA for AF in patients with continuous ambulatory milrinone infusion. Milrinone is a phosphodiesterase III inhibitor which increases cyclic adenosine monophosphate and intra-cellular calcium. Myocardial contractility is enhanced and systemic vascular resistance decreased as a result, without the expense of increased myocardial oxygen consumption [26]. Thus, milrinone is an attractive management strategy in severe forms of heart failure. However, calcium also plays a promotional role in AF [27]. Clinical data regarding milrinone use has shown an increased incidence of AF in post-cardiac surgery [28],[29] and with a short-term use inpatient heart failure study [30]. Ours is the first to report the use in patients undergoing CA for AF. All patients achieved NSR with their procedure and remained arrhythmia-free during their brief hospital stay. Four out of 5 patients maintained NSR following CA up to the 3-month follow-up mark, in spite of milrinone use over that time. As such, milrinone use does not appear to be an impediment to maintaining NSR following CA in this limited experience, despite its pro-arrhythmia propensity. Conversely, CA appears to enhance the likelihood of discontinuing milrinone due to improved subjective symptomatology and 6-minute hall walk evaluations.
Minnesota living with heart failure questionnaires were not applied to our group pre- and post-ablation. Long-term follow-up echocardiographic data would be informative as well, and has been limited by study blinding in 1 patient and death in 2 patients. Conclusions applying broadly to Class IV heart failure patients for CA of AF improving heart failure status cannot be drawn based on our smaller case load. Multiple studies have reported improved heart failure status with successful CA for AF in Class II and III patients [2],[5],[7],[9]-[11], so it does not seem unreasonable to believe the same may not ultimately prove true in Class IV.
Who should be performing CA of AF in LVSD? Our experience is certainly not the basis with which to solely answer this question. The Heart Rhythm Society admits that exact numerical skills for CA in AF in general are hard to determine [31]. What is evident regarding success of CA for AF is that higher volume centers fare better [32],[33].
Other Limitations This study represents a single-center, single-operator experience that prevents generalizability to the EP community as a whole. As mentioned above, limited numbers and follow-up do not allow firm conclusions to be drawn. Referral bias cannot be excluded, and might ultimately affect the true safety and success in this population. As a pilot “exercise” in this selected group of patients, though, the results are encouraging, and don’t preclude further pursuit.
CA for persistent AF in Class IV chronic systolic heart failure even on advanced therapies is feasible. Milrinone does not appear to impede the ability to attain and maintain NSR in short-term follow-up from CA. Heart failure status and EF may be improved on an individual basis. The possibility of needing repeat ablation should be expected. Enhanced experience of CA will be required from a multi-center approach, including measurement of consistent endpoints across the entire cohort, before conclusions may be more broadly applied to this severe form of LVSD.






