Exploring the Association Between Physical Activity and Atrial Fibrillation: A Systematic Review of Meta-Analyses
Andreas Müssigbrodt12*, Alireza Sepehri Shamloo1*, John Mandrola3, Jawdat Abdulla4, Hakeem Ayinde5, Cristian Ricci6, Natale Daniele Brunetti7, Chun Shing Kwok89, Sanghamitra Mohanty10, Andrea Natale10, Jedrzej Kosiuk11, Tiago Luiz Luz Leiria12, Simon Kircher1, Nikolaos Dagres1, Sergio Richter1, Arash Arya1, Andreas Bollmann1, Gerhard Hindricks1, Michael Doering1
1Department of Electrophysiology, Heart Centre Leipzig at University of Leipzig, Leipzig Heart Institute, Leipzig, Germany.2Cardiology Department, CHU Fort de France, Pierre Zobda Quitman Hospital, Martinique, France.3Baptist Health Louisville, Louisville, USA.4Department for Medicine, Section of Cardiology, Glostrup University Hospital, Copenhagen, Denmark.5Division of Cardiology, Section of Electrophysiology, Emory University, Atlanta, USA.6Africa Unit for Transdisciplinary Health Research (AUTHeR), North-West University, Potchefstroom Campus, South Africa.7Cardiology Department, University of Foggia, Foggia, Italy.8School of Primary, Community & Social Care, Keele University, Stoke-on-Trent, UK.9Department of Cardiology, Royal Stoke University Hospital, Stoke-on-Trent, UK.10Texas Cardiac Arrhythmia Institute, St. David’s Medical Center, Austin, TX, USA.11Rhythmology Department, Helios Klinikum Köthen, Köthen, Germany.12Cardiology Institute, Porto Alegre, Brazil.*Shared first authorship: Andreas Müssigbrodt and Alireza Sepehri Shamloo contributed equally.
Numerous studies suggest intensive and prolonged exercise is a risk factor for atrial fibrillation (AF); many other studies have shown that regular exercise can protect against AF in the general population. Meta-analyses of these studies have produced conflicting results. Thus, we performed a systematic review of meta-analyses to understand better the evidence base linking exercise and AF.
We conducted a systematic review of meta-analyses that evaluated the association between physical activity (PA) and AF. A search of MEDLINE, Scopus, and Google Scholar was performed. The Assessing Methodological Quality of Systematic Reviews 2 (AMSTAR 2) measurement tool was used to evaluate the methodological quality of the included reviews.
A total of twelve meta-analyses met the inclusion criteria. Five meta-analyses reported consistent evidence that the risk of AF was increased among athletes compared to non-athletes.The increased risk of AF ranged from OR 1.64(1.10-2.43) to OR 5.3(3.6-7.9). The results were less consistent among studies of different degrees of PA as three reviews suggest that PA was associated with a reduction in AF, but most studies reported no difference in AF risk. Subgroup analyses suggest that individuals younger than 54-60 years and men were more likely to develop AF with PA.
PA has a dose-dependent J-shape effect on AF risk, with increased risk at very low and very high levels of PA. This effect seems to be gender-specific and more pronounced in younger males.
Key Words : .
Andreas Müssigbrodt,Cardiology Department, CHU Fort de France, Pierre Zobda Quitman Hospital, Martinique, France
Atrial fibrillation (AF) is the most common sustained arrhythmia in adults, with an estimated prevalence of 1-2% in the general population1. Due to the increasing number of elderly adults and the increasing prevalence of cardiometabolic risk factors associated with AF, an upsurge of AF prevalence has been predicted 2, 3. A better understanding of AF pathophysiology and preventable factors may lead to the development of appropriate preventive programs that could play a significant role in promoting community health and reducing the costs associated with disease management4, 5.
Through its favorable effects on weight, lipids, blood pressure, and cardiorespiratory fitness, physical activity (PA) associates with a lower risk of heart disease.6 Although numerous studies have suggested that intensive and prolonged exercise as in endurance sports is a risk factor for AF, many other studies have shown that regular exercise can be a protective factor for AF in the general population7-9. Over the past two decades, more than 40 studies and twelve metaanalyses have investigated the link between physical exercise and the risk of developing AF. Systematic reviews allow us to enhance our understanding based on accurate, succinct, credible, and comprehensive summaries of the best available evidence on a topic10. However, in the case of exercise and AF, the available meta-analyses have produced conflicting results7, 8, 11-20. To improve understanding of this relationship, we performed a systematic review of meta-analyses,evaluating the association between PA and AF from different aspects. In addition, we discussed the possible mechanisms for this association.
We aimed to identify systematic reviews with meta-analysis,which examine the association between PA and AF. This systematic review of meta-analyses was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA Statement21.
2.2. Eligibility criteria
All studies that evaluated the association between PA and AF, were considered eligible. However, only systematic reviews with metaanalysis were included in the current study. Original papers, case reports, letters, conference abstracts, or comments were not included in this study. There were no restrictions on the definition of PA, which included varying degrees of PA or exercise as well as participants in sports or comparisons of athletes and non-athletes.
Databases including MEDLINE, Scopus, and Google Scholar, were searched to identify all relevant reviews, without language restriction, published before January 1, 2021. The search terms included the following keywords: (“atrial fibrillation” OR “arrhythmias, cardiac” OR “auricular fibrillation”) AND (“physical activity” OR “endurance” OR “exercise” OR “sports” OR “athletes”).
Titles and abstracts were screened for the exclusion of unrelated articles. References and citations of included studies were also reviewed for additional reviews that met the inclusion criteria. The selection of studies to be included was independently performed by two reviewers (AM; ASSH).
2.5. Data collection process
Using a data extraction table, the required information from each meta-analysis, including first author’s name, publication year, types of included studies, used databases, main inclusion criteria, pooled sample size, age and gender, main findings, and results of subgroup an alysis were extracted. In addition, for the results of meta-analyses, the effect estimates (odds ratios, relative risk, hazard ratios) and the number of studies pooled were collected, and any reported measure of statistical heterogeneity. The table was initially completed by one of the first authors (ASSH) and then verified by the other first author to control the accuracy of data entry (AM). After finalizing the first draft of this systematic review of meta-analyses, all corresponding authors (n=11) of the included meta-analyses (n=12) were invited to assess the correctness of the included data and contribute their expert opinion to the manuscript. Seven out of 11 authors accepted the invitation, whereas four authors did not respond. Those seven authors (JA, HA, CR, NDB, MM, CSK, TLLL) revised the entire manuscript and confirmed the authenticity of the final systematic review report after some minor changes.
2.6. Heterogeneity assessment
The heterogeneity between estimates of the AF risks for exposure to a high volume of PA concerning lower PA volume was investigated through Cochrane Q-test and I2 statistic. Heterogeneity assessment was evaluated by a random effect analysis in which study weights were computed as wi = 1/(si2 + t2) where si2 was the variance estimate from the i-th study, and t2 was the overall variance. The heterogeneity was investigated for estimates from all meta-analyses as a whole and meta-analyses based on the general population and athletes as well. The sensitivity analysis was conducted in the form of influence analysis, excluding a study at the time. Heterogeneity assessment was reported by forest plot. Heterogeneity assessment, forest plots, and influence analyses were performed using the metan and metaninf function of the STATA software (vers.12). We did not aim to perform an estimate of a meta-analysis of meta-analyses in order to avoid duplication bias.
The Assessing Methodological Quality of Systematic Reviews 2 (AMSTAR 2) measurement tool was used to evaluate the methodological quality of the included meta-analysis22. The AMSTAR contained 16 items for quality assessment of the reported information. Then studies were classified into four different groups critically low, low, moderate, and high based on the result of quality assessment calculated online via https://amstar.ca/. Quality assessment was performed by two different assessors (AM and ASSH) and a third assessor (CR) for discrepancies.
3.1. Selection of meta-analyses
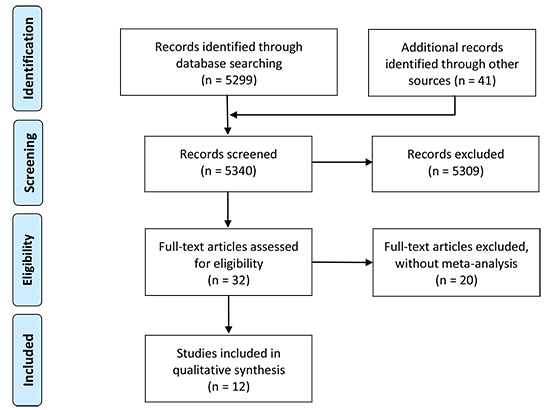
A total of 5340 unique abstracts were retrieved in electronic databases and manual cross-checking of reference lists. From this, 5309 were excluded, and the full text of the remaining 32 review articles was studied in detail. Finally, 12 meta-analyses were included in this review [Figure 1].
Figure 1. PRISMA flow chart describing study selection.
3.2. Characteristics of included meta-analyses
The included systematic reviews and meta-analyses are summarized in [Table 1]. The reviews were published over an 11-year period between 2009-2020. The review with the largest pooled sample size was authored by Mishima et al. (n=1,464,539)20, while the smallest was the first published study by Abdulla et al. (n=1,550)7. The pooled gender ratio was reported only in two studies 7, 20, and the pooled age was reported by six studies 7, 12, 13, 18-20. Most of the reviews, included studies of only case-control or cohort/post hoc analysis of randomized controlled trials in design, but two reviews did include cross-sectional studies [Table 1].
Table 1. Characteristics of include dreviews
| Reference |
Primary studies (n); Types |
Participants (n) |
Main Databases |
Main inclusioncriteria |
Age (A)
Gender (G) |
Subgroupanalyses |
Main aim/question of review |
| Abdulla 7, 2009 |
6
Case-control 6 |
1550 |
Medline EMBASE Cochrane |
Case–-control studies reporting the number of AF or AFlu in athletes compared with controls |
A: 51 ± 9 years
G: 93% male |
N/A |
Is the risk of AF higher in athletes than in the general population? |
| Nielsen 8, 2013 |
10
Case control 6
Cross-sectional 4 |
1550 (onlycasecontrols) |
Medline EMBASE Cochrane |
Case–-control studies reporting number of incidental AF or AFlu in athletes compared with non-athletes |
A & G: N/A |
-Athletes and nonathletes
-PA categories |
To examine the relationship between PA and risk of newonset AF or AFlu. |
| Ofman 11, 2013 |
4
Prospectivecohort 4 |
95526 |
Medline EMBASE Cochrane |
Both prospective cohort and case–-control studies examining the relation of regular PA and AF risk |
A & G: N/A |
N/A |
To examine the association between regular physical activity and the risk of AF |
| Kwok12, 2014 |
19
Post hoc RCT 2
Cohort 10
Case-control 7 |
511503 |
Medline EMBASE |
1. Studies assessing the link between the history of PA and the subsequent risk of AF
2. Studies assessing outcomes in athletes for PA
3. There was no strict definition of PA |
A: Range
41-73 years
G: N/A |
-Nature of PA
-Studies quality |
To examine the relationship between AF and the extent of PA |
| Brunetti13, 2016 |
11
Post hoc RCT 1
cohort 5
Case-control 5 |
81787 |
Medline |
1. Studies assessing the risk of developing AF in subjects practicing PA or sport activity
2. There was no strict definition of PA |
A: Range 43-73 years
G: N/A |
-Gender
-Age groups |
To examine the association of age and gender with the Incidence of AF in subjects practicing PA |
| Mohanty14, 2016 |
22
Cohort 12
Case-control 5
Post hoc RCT 1
Cross-sectional 2
Prospective
observational 1
Retrospective 1 |
656750 |
Medline Bio Med Centra Cardio source EMBASE clinicaltrials. gov ISI Web of Science |
1. Report relation between PA and incidence of AF
2. A case-control or population-based design
3. Specify AF incidence and number of participants for men and women |
A & G: N/A |
-Athletes and nonathletes
-Gender
-PA categories |
To examine the association of different intensities of PA with the risk of AF in Men and Women |
| Zhu 15, 2016 |
13
Post hoc RCT 2
Prospective cohort 10
Case-control 1 |
568072 |
Medline Cochrane Science Direct |
Studies estimating the association between PA and developing AF in the general population |
A & G: N/A |
-PA categories
-Region
-Gender |
To examine the association between PA and incident AF, as well as to determine whether a sex difference existed |
| Ricci 16, 2018 |
19
Cohorts 18
Case-control 1 |
29855 (all were AF subjects) |
Medline EMBASE Cochrane CINAHL |
Studies reported relative risk (RR) estimates of the association between PA and AF in the general population |
A & G: N/A |
-Region
-Publication date
-Studies quality
-Adjustment for CAD RFs |
To examine the association between PA volume and AF risk |
| Ayinde 17, 2018 |
8
Cohorts 6
Case-control 2 |
9113 |
Medline EMBASE Scopus SPORT Discus |
Studies assessed the association between competitive or semi-competitive sports and AF |
A & G: N/A |
-Studies quality
-Age groups |
To examine the association between competitive sports sport and AF risk |
| Li 18 2018 |
9
Cohort 3
Case-control 4
Cross-sectional 2 |
8901 |
PubMed Embase Cochrane |
1. Case-control or cohort studies that focused on the association of endurance exercise and AF
2. Comparison of athletes group with nonathletes
group (control). |
A: mean age 39-72.8 years
G: N/A |
-Gender
-Mean age
-Study type
-Sample size
-Sports mode |
To quantitatively assess the risk of AF in athletes and the general population |
| Garlipp 19 2019 |
11
Cohort 10
Post hoc RCT 1 |
276323 |
Medline BVS Health Cochrane |
All cohort studies, prospective, crosssectional, observational and randomized clinical trials with patients who performed physical exercises and the development of AF. |
A: Range 12-90 years
G: N/A |
N/A |
To analyze the effects of physical activity on the incidence of AF |
| Mishima 20 2020 |
15
Prospective cohort studies |
1,464,539 |
Medline Embase |
Prospective cohort studies, with a minimum follow-up of 4 years, reporting the association between PA and incident AF |
A: median age 55.3 years
G: 51.7 % female |
-Gender |
to systematically summarize the evidence on the 82 association between PA and risk of AF |
AF: Atrial fibrillation; AFlu: Atrial flutter; N/A: Not available; PA: physical activity; CAD RFs: Coronary artery disease risk factors; RCT: Randomized Controlled Trial
Subgroup analyses were performed in most of the studies (11/12). The most common types of subgroup analyses were for PA categories and gender. Ricci et al.16 performed the greatest variety of subgroup analyses, including region, publication date, studies quality, and adjustments for CAD risk factors [Table 2]-[Table 3]. Most of the conducted meta-analysis compared AF risk in two groups of high PA versus no PA (n=6), or high PA versus low PA (n=6); followed by athletes versus non-athletes (n=5), high/moderate PA versus low/no PA (n=4), and high PA versus moderate PA (n=1) [Table 2].
Table 2. A summary of main findings of conducted meta-analyses
| Reference |
Studies and Participants (n) |
Effectsize (95% CI) |
Narrative findings |
Definition forphysical activity |
| Studies comparing athletes versus non-athletes |
| Abdulla 7, 2009 |
6 studies 1550 |
OR=5.29 (3.57 - 7.85) |
The risk of AF or atrial flutter was significantly higher in athletes than in controls. |
N/A |
| Nielsen 8, 2013 |
6 studies 1550 |
OR=5.3 (3.6- 7.9) |
AF increased in athletes compared to non-athletic |
N/A |
| Kwok 12, 2014 |
6 studies 1973 |
RR=1.98 (1.00 - 3.94) |
The risk of AF was increased in athletes or participants with a history of sports activity (lowquality studies) in comparison with controls |
N/A |
| Ayinde 17, 2018 |
8 studies 9113 |
OR=1.64 (1.10 - 2.43) |
Athletes have an increased risk of AF compared to the general population. Age appears to modify the risk of AF in athletes |
Competitive or semi-competitive sports (no further definition) |
| Li 18 2018 |
9 studies 8901 |
OR=2.34 (1.04–5.28) |
The risk of AF was significantly higher in athletes than in the general population |
N/A |
| Studies comparing high PA versus low PA |
| Ofman 11, 2013 |
4 studies 95,526 |
OR=1.08 (0.97-1.21) |
AF was not different in maximum versus the minimal amount of PA |
Based on cumulative PA per week (4-5 categories) |
| Nielsen 8, 2013 |
3 studies N/A |
OR=0.92 (0.80 - 1.05) |
AF was not different in high PA compared with low PA |
N/A |
| Zhu 15, 2016 |
10 studies N/A |
RR=0.98 (0.90 - 1.06) |
Comparing the most physically active vs. the least physically active groups |
PA categories |
| Ricci 16, 2018 |
19 studies 29,855 |
RR= 0.97 (0.85 - 1.10) |
High PA, in comparison to low PA, did not affect AF risk |
Based on MET-h/week
<3 (light intensity PA like slow walking)
3–6 (moderate intensity PA like slow cycling)
>6 (vigorous-intensity PA like fast running). |
| Garlipp 19 2019 |
11 studies 276,323 |
RR=0.914 (0.833 - 1.003) |
Individuals who exercise are less likely to have AF. |
N/A |
| Studies comparing high PA versus no PA |
| Nielsen 8, 2013 |
3 studies N/A |
OR=0.78 (0.68 - 0.89) |
AF reduced in high PA compared with no PA |
N/A |
| Kwok 12, 2014 |
8 studies 152,925 |
RR=1.0 (0.82 - 1.22) |
Engaging more intensive PA in comparison with controls had no effect on AF risk |
N/A |
| Mohanty14, 2016 |
7 studies 93,995 |
OR=2.47 (1.25 - 3.7) |
A sedentary lifestyle compared to moderate or intense activities was RF for AF |
Study reports (Based on 3 to 5 PA or exercise levels) |
| Brunetti13, 2016 |
11 studies 81,787 |
OR=0.92 (0.84 - 1.01) |
The risk of AF was not significantly higher in subjects practicing PA than in controls |
Nostrictdefinition |
| Zhu 15, 2016 |
11 studies N/A |
RR=1.07 (0.93 - 1.25) |
The risk of AF was not significantly increased in individuals with intensive physical activity (vigorous, high intensity, or heavy workload) |
High-intensityexercise>2000 hours |
| Garlipp 19 2019 |
11 studies 276,323 |
RR=0.914 (0.833 - 1.003) |
Individuals who exercise are less likely to have AF. |
N/A |
| Studies comparing high PA versus moderate PA |
| Nielsen 8, 2013 |
3 studies N/A |
OR=1.01 (0.88 - 1.17) |
AF was not different in high PA compared with moderate PA |
N/A |
| Studies comparing high/moderate PA versus low/no PA |
| Nielsen 8, 2013 |
2 studies N/A |
OR=0.89 (0.83 - 0.96) |
AF reduced in moderate/high PA compared with none/very low PA |
N/A |
| Kwok 12, 2014 |
4 studies 112,784 |
RR=0.95 (0.72 - 1.26) |
Spending more time on PA in comparison with controls had no effect on AF risk |
N/A |
| Mishima 20 2020 |
15 studies 1,464,539 |
HR 0.94, (0.90-0.97) |
PA at guideline-recommended levels and above are associated with a significantly lower AF risk. However, at 2000 MET-minutes per week and beyond, the benefit is less clear |
N/A |
AF: Atrial fibrillation; CI: confidence interval, N/A: Not available; PA: physical activity; MET-h: Briefly, a metabolic equivalent (MET-h) is defined as an energy expenditure of 1 kcal/kg per h and is roughly equivalent to the energy cost of sitting quietly. OR: odds ratio, RR: risk ratio
3.3.1. Studies comparing athletes versus non-athletes
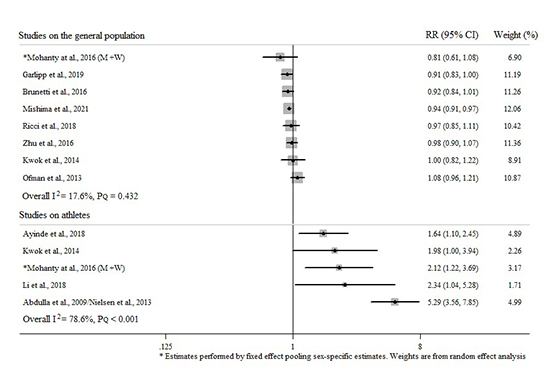
Five meta-analyses assessed the differences in AF risk between athletes and non-athletes 7, 8, 12, 17, 18. These found a significantly higher risk of AF or atrial flutter in athletes compared with non-athletes or controls (odd ratio (OR) range [95% CI] 1.64 [1.10-2.43] - 5.3 [3.6-7.9] and relative risk (RR) range 1.98 [1.00-3.94] 7, 8, 12, 17, 18 [Table 2].Results from heterogeneity assessment pointed out a large variability when all studies were considered a whole (I2 = 88.6%). Nevertheless, a low variability among AF risks estimates from studies conducted on the general population was observed (I2 = 17.6%). On the other hand, a consistent heterogeneity among AF risks estimates from metaanalyses conducted among athletes was observed (I2 = 78.6%) [Figure 2]. The heterogeneity from meta-analyses conducted among athletes was nullified (I2 = 0%) in a sensitivity analysis, excluding the study with the highest AF risk7.
Figure 2. Forest plot of meta-analytical estimates of AF risk for higher vs. lower physical activity volume in athletes and the general population. PQ is the P-value for the Cochrane Q test for heterogeneity
3.3.2. Studies comparing high versus low/no physical activity
Five out of five meta-analyses revealed no difference between low PA and high PA for risk of AF 8, 11, 15, 16, 19 [Table 2].
3.3.3. Studies comparing high versus no physical activity
Two different categories of results were found in this group of studies. Three studies found no significant difference in AF risk between high PA and no PA12, 13, 15, whereas three others found a protective effect of high PA on AF development8, 14, 19 [Table 2].
3.3.4. Studies comparing high/moderate versus low/no physical activity
In this category, although Nielsen et al. and Mishima et al. reported a reduction in AF with moderate/high PA compared to none/very low PA8, 20; the review by Kwok et al. showed no significant difference between any physical activity or leisure-time activity and risk of AF (RR 0.95 [0.72-1.26])12 [Table 2].
3.3.5. Studies comparing high versus moderate physical activity
The only conducted meta-analysis on this issue revealed that AF risk was not significantly different for individuals with high levels of PA versus moderate levels of PA (OR 1.01 [0.99-1.17]) 8 [Table 2].
3.4.1. Gender and Age Subgroups
Subgroup analysis based on gender suggests that men have a greater risk of AF with PA13-15, 18. Mishima et al. reported that PA above the guideline-recommended level was associated with a lower risk of AF in women, but not in men20. In two meta-analyses, a subgroup analysis of patients younger and older than 54 years was performed 13, 17, and individuals younger than 54 years in both studies reported a higher risk of AF. In contrast, individuals older than 54 years showed no association between PA and AF17 or a protective effect of exercise 13 [Table 3]. Li et al. showed that AF risk was significantly higher in male athletes <60 years old the general population18.
Table 3. Studies comparing the impact of PA on AF based on different factors
| Reference |
Subgroups Effectsize |
(95% CI) |
Narrative findings |
| Genders |
| Brunetti13, 2016 |
Male OR=7.49 (3.12 - 19.01) |
Male and/or female OR=0.89 (0.81– 0.97) |
The risk of AF seems higher in male subjects practicing physical exercise |
| Mohanty14, 2016 |
Male Moderate 0.81 (0.26 - 1.003)
Intense 3.30 (1.97 - 4.63) |
Female Moderate 0.91 (0.78 - 0.98)
Intense 0.72 (0.57 - 0.88) |
Moderate and intense exercise compared to sedentary were protective factors for AF in women.
Although moderate exercise was a protective factor, intense exercise was a risk factor for AF in men. |
| Mohanty14, 2016 |
Male Athletes 3.3 (1.72 - 5.91)
Non-athletes 3.4 (1.26 - 5.42) |
Female Athletes 0.67 (-0.59 - 1.92)
Non-athletes 0.85 (0.51 - 1.21) |
Vigorous PA versus leisuretime exercise in man was found to be associated with a significantly high risk of AF in athletes with endurance sports practice |
| Zhu 15, 2016 |
Male Total PA RR=1.18 (1.02 - 1.37)
Intensive PA RR=1.12 (0.99 - 1.28) |
Female Total PA RR=0.92 (0.87 - 0.97)
Intensive PA RR=0.92 (0.86 - 0.98) |
Association between total PA exposure and the risk of AF
Association between total intensive PA exposure (vigorous, high intensity, or heavy workload) and the risk of AF |
| Li 18 2018 |
Male Athletes OR=4.03 (1.73–9.42) |
|
The risk of AF was significantly higher in athletes compared with the general population, especially in male athletes <60 years old. |
| Mishima20, 2020 |
PA above the guidelinerecommended level
Male HR 0.96 (0.93 – 1.00)
Highest PA HR 1.03 (0.94 – 1.12) |
PA above the guidelinerecommended level
Female HR 0.91, (0.88-0.95)
Highest PA HR 0.88 (0.83 – 0.92) |
PA above the guidelinerecommended level was associated with a lower risk of incident AF in women and men. Highest PA was associated with a lower risk of AF in women, but not in men, compared to inactive. |
| Age |
| Brunetti13, 2016 |
Younger than 54 years OR=5.30 (3.43 - 8.20) |
Olderthan 54 years OR=0.84 (0.76 - 0.92) |
A reverse correlation between age and risk of AF seems to be evident |
| Ayinde17, 2018 |
Younger than 54 years OR=1.96 (1.06 - 3.65) |
Olderthan 54 years OR=1.41 (0.81 - 2.44) |
Age appears to modify the risk of AF in athletes. |
| Li 18 2018 |
Younger than 60 years OR=3.24 (1.23 - 8.55) |
|
The risk of AF was significantly higher in athletes compared with the general population, especially in male athletes <60 years old. |
| Region |
| Zhu 15, 2016 |
American RR=0.95 (0.86 - 1.06) |
Non-American RR=1.05 (0.86 - 1.27) |
The impact of total PA on AF risk was not related to the region of studies |
| Zhu 15, 2016 |
American RR= 1.02 (0.89 - 1.17) |
Non-American RR: 1.23 (0.68 - 2.21) |
Impact of Intensive PA (vigorous, high intensity, or heavy workload) on AF risk was not related to the region of studies |
| Ricci 16, 2018 |
American RR=1.24 (0.97 - 1.60) |
Non-American
Europe RR=0.86 (0.71 - 1.04)
Australia and New Zealand RR=0.80 (0.62 - 1.03) |
The impact of PA on AF risk was not related to the region of studies |
| Publicationrelatedissues |
| Kwok12, 2014 |
Low risk of bias OR=0.80 (0.52 - 1.24) |
High risk of bias OR= 1.12 (0.94 - 1.32) |
The impact of any PA or leisure-time activity on AF risk was not related to the bias risk of the studies |
| Kwok12, 2014 |
Low risk of bias RR=1.04 (0.87 - 1.24) |
High risk of bias OR=1.04 (0.73 - 1.49) |
The impact of intensive PA on AF risk was not related to the bias risk of the studies |
| Ricci 16, 2018 |
NOS1>6 RR= 1.06 (0.92 - 1.22) |
NOS≤6 RR= 0.87 (0.66 - 1.14) |
The impact of PA on AF risk was not related to the quality score of studies |
| Ayinde17, 2018 |
NOS ≥ 6 OR=2.23 (1.45 - 3.41) |
NOS < 6 OR=1.22 (0.81 - 1.83) |
The impact of PA on AF risk was related to the quality score of studies |
| Ricci 16, 2018 |
After median RR= 1.02 (0.66 - 1.57) |
Before median RR= 0.96 (0.85 - 1.08) |
The impact of PA on AF risk was not related to the publication date of studies |
| Li 18 2018 |
Case control group OR=5.10 (3.07–8.46) |
|
In the subgroup analysis based on study type, a significant risk was found in the case control group |
| Sample size |
| Li 18, 2018 |
sample sizes <300 OR=4.91 (3.08 - 7.84) |
|
Based on the sample sizes, the group with sample sizes <300 demonstrated significant results |
| Mode of sport |
| Li 18, 2018 |
Single typesports OR=3.97 (1.16 - 13.62 |
|
In the subgroup analysis based on sports mode, a significantly increased risk was found in the group with a single type |
1: NOS: Newcastle Ottawa Quality
3.4.2. Geographic regions
Two meta-analyses reported that the influence of American and non-American studies on PA on AF risk, and the studies conclude that the impact of PA on AF risk was not significantly affected by the region where the study took place15, 16 [Table 3].
3.4.3. Publication related issues
In two studies, the impact of “included studies quality” was assessed16, 17, while in two meta-analyses, the effect of publication bias was investigated16, 20. These studies revealed that neither publication bias nor quality scores were associated with the impact of PA on AF risk. In another study, the effect of the publication date of studies was assessed, which showed no significant impact too16 [Table 3]. The impact of sample size and mode of sport on the risk of AF was also reported by Li et al.18
3.4.4. Levels of Activity
Ricci et al.16 performed the only meta-analysis linking exercise dose to the risk of AF. They showed that in individuals with PA at volumes of 5–20 metabolic equivalents per week (MET-h/week), PA was associated with a significant reduction of AF risk (RR for 19 MET-h/week=0.92 (0.87 - 0.98). By comparison, PA volumes exceeding 20 MET-h/week were unrelated to AF risk (RR for 21 MET-h/week=0.95 (0.88 - 1.02).
In the subgroup analysis based on sports mode - performed by Li et al. 18, a significantly increased risk was found in the group with a single type of sport (OR=3.97, 95% CI=1.16–13.62, Pheterogeneity=.018, I2=70.4%)
The overall quality of the included studies using the AMSTAR-2 tool was evaluated and reported in [Table 4].
Table 4. Evaluation of quality of included studies using the AMSTAR-2 tool
The main findings of this systematic review can be summarized as follows: First, there is consistent evidence from few reviews that athletes are at greater risk of AF than non-athletes. Second, in a general population with both genders, there is evidence that high or moderate PA compared to low or no PA is associated with a lower risk of AF. Third, the literature suggests that men are more likely to develop AF with PA compared to women. Finally, patients younger than 54-60 years appear to have a greater risk of AF with increased levels of PA.
4.2. Overview of the results of twelve different meta-analyses
Abdulla and Nielsen published the first meta-analysis of 6 casecontrol studies in 2009 7. They then published another meta-analysis in 2013, which now included prospective comparative data on the intensity of PA in populations with and without AF 8. Despite the addition of newer studies, they still found an increased risk of AF in athletes than non-athletes or the general population. Nevertheless, a new observation from the three prospective studies was that moderate/high habitual PA was associated with a significantly reduced risk of AF compared with none or very low-intensity PAOR=0.898.
Also, in 2013, Ofman et al. published a meta-analysis with the opposite result: “Our data do not support a statistically significant association between regular PA and increased incidence of atrial fibrillation” 11. The reason for the disparate findings was likely that Ofman et al. evaluated the relation between increased level of PA and AF among non-athletes, while Nielsen et al. conclusion was mainly based on the comparison between athletes and non-athletes.
In 2014, Kwok et al. performed a larger meta-analysis of 19 studies including ≈ 511k individuals and confirmed the findings of Ofman et al. that there was no association between higher levels of PA and AF12. Further more, due to the larger size of the study, Kwok et al., were able to conduct subgroup analyses based on the effect of vigorous PA, level of PA.
The meta-analysis by Brunetti et al. from 2016 also confirmed previous findings that found no significant associations between PA and increased risk of AF13. Brunetti et al. even noted a trend towards a lower risk of AF, though the strength of this finding was limited by high heterogeneity 13.The heterogeneity might be due to gender and age; they argued that AF development risk seemed to be increased in studies enrolling younger and male subjects13.
The gender-dependency of AF hypothesis was then re-assessed by Zhu et al. and Mohanty et al.. Zhuet al. showed that increased PA exposure was associated with an increased risk of AF in males, with a significantly reduced risk of AF in women 15. Similarly, Mohanty et al., found intensive PA associated with an increased risk of AF in men and a decreased risk of AF in women 15.
Mohanty et al. also observed that a sedentary life style significantly increases the risk of AF while a moderate amount of PA reduces the risk of AF14. Ricci et al. described a J-shaped relation between PA volume and AF risk, where PA at volumes of 5 to 20 MET-h/week was associated with a reduced AF risk, whereas both, sedentary lifestyle and intensive PA of more than 20 MET-h/week, showed no protective effect on AF risk and no difference in direct comparison.
Two different meta-analyses by Ayinde et al.17. and Li et al.18, both conducted in 2018, reconfirmed the early findings from Abdulla and Nielsen, and showed that athletes have an increased risk of AF compared to the general population. Subgroup analysis by Ayinde et al.17 demonstrated an increased risk for adults younger than 54 years. Li et al. similarly reported an increased risk for men younger than 60 years.
Garlipp et al.19 included studies with athletes and studies with the general population in their meta-analysis. The combined analysis of the studies did not suggest a significant increase in AF in subjects submitted to exercise (RR = 0.914, 95% CI = 0.833 – 1.003, heterogeneity: p < 0.001). Garlipp et al. concluded that individuals who exercise are less likely to have AF.
In 2020, Mishima et al.20 published a meta-analysis with the most participants so far. It included 1,464,539 individuals. According to their results, individuals achieving the guideline-recommended level of PA (450 MET-minutes per week)had a significantly lower risk of AF (HR 0.94, 95% CI 0.90-0.97, p=0.001). Dose-response analysis showed that PA levels up to 1900 MET minutes per week were associated with a lower risk of AF, with less certainty beyond that level.
The publication of 12 meta-analyses on AF and PA in the last 12 years demonstrates a strong interest in the topic. Individual meta-analyses led to different, apparently contrary conclusions. Our interpretation of the existing body of evidence refers to a dose-response association between PA dose and AF risk. Whereas moderate PA seems to have a protective effect, it seems that no PA and vigorous exercise may increase the risk for AF. The next question is whether the pathophysiology supports the epidemiologic observations.
4.3. Potential mechanisms for altered risk of AF with physical activity
4.3.1. Athletes are more at risk of AF than non-athletes
AF pathophysiologyis characterized by Coumel’s triangle consisting of focal triggers, arrhythmogenic substrate created by e.g. increased left atrial size with anisotropy and fibrosis, and additional factors as autonomic imbalance or disturbed electrolyte homeostasis23-25.
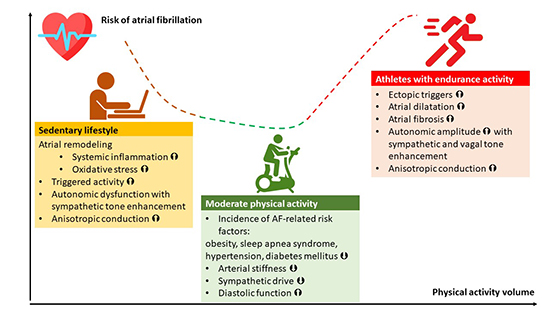
Typical, non-athletic patients with AF are overweight elderly patients with arterial hypertension. Athletes with AF exhibit a different phenotype. So even though similar pathophysiology may exist in both non-athletic patients and athletes with AF, other mechanisms or a different degree of influence of the above-mentioned factors seems likely [Figure 3].
Figure 3. Different possible mechanisms through which physical activity may contribute to atrial fibrillation.
Athletes show specific characteristics that may favor the development of AF. These characteristics mainly occur in endurance athletes, which seem to be more prone to AF than athletes from non-endurance sports26. In addition, athletes exhibit an increased autonomic influence by both antipodes of the autonomous nervous system, the vagal and the adrenergic system27.
Strong support of an exercise-induced model of AF came from Guasch et al., who compared exercised rats with sedentary control rats. Training caused enhanced atrial fibrosis, increased AF vulnerability, and vagal tone. Detraining reversed AF vulnerability and vagal tone28. Studying human subjects, Wilhelm et al. reported that vagal activity, p-wave duration, premature atrial contractions, and LA volume were associated with lifetime training hours in a study with runners29.
Wijffels et al. observed in goats that atrial refractory period shortening (electrical remodeling) by pacing occurred directly, where as persistent AF occurred after two weeks. The authors hypothesized, therefore, that persistent AF needed a “second factor” 30. A potential “second factor” could be an atrial structural disease such as tissue fibrosis31.
Findings of direct histological substrate characterization in patients with AF have also confirmed atrial substrates’ presence, mainly fibrosis, in the development and progression of AF32.
Another risk factor for AF is arterial hypertension33. Arterial hypertension leads to impaired diastolic function by cardiac remodeling and associates with an enhanced risk of AF 33-35. Thus, arterial hypertension induced and/or enhanced by exercise may also increase the probability of developing AF in athletes. However, as only a minority of athletes develop AF, it is still unknown, which specific factors most likely determine the AF risk. In addition, genome-wide association studies in the general population described common variants in specific genomic regions related to AF36. Nonetheless, no typical mutation has been reported in athletes with AF.
4.3.2. In the general population, moderate physical activity seems to be protective against AF
Regular PA by physical work, moderate leisure-time sports, or daily commuting by walking or using a bicycle has many positive effects on physical and mental health. It increases general fitness, helps to maintain average weight, blood pressure,and blood sugar 26. In addition, regular PA has positive effects on mood and mental health. It may balance the negative effects of the increasingly sedentary lifestyle in industrialized countries, and there is evidence that it increases life expectancy.
As regular PA counteracts risk factors for AF as overweight, arterial hypertension, and diabetes mellitus, it is not surprising that a sedentary lifestyle is associated with an increased prevalence of AF. In contrast, regular physical work seems to reduce the risk for AF.
Still though, our review cannot answer the often-asked: What distinguishes athletic activities that seem to increase the risk for AF from daily life physical activities that decrease the risk? It seems logical that PA volume and intensity are increased in athletes, compared to “normal” physical in the general population. Another factor might be the increased vagal and adrenergic activity in athletes, compared to the general population. Thus, the dose response relation between PA volume and AF risk appears to follow a J- or U-shaped curve. PA at the bottom of the curve with volumes of 5 to 20 MET-h/week may result in a reduced risk for AF, whereas lower and higher volumes of PA may lead to an increased risk for AF16.
4.3.3. In the male gender, physical activity seems to act as a risk factor for AF development, while in females as a protective factor
Male gender has been found as a risk factor for AF in athletes 37. At similar amounts of exercise, males showed - compared to females - a more pronounced atrial remodeling and an impaired diastolic function. In addition, arterial hypertension at rest and during exercise and an increased sympathetic tone in males might increase the AF susceptibility 37. Another reason may be the taller stature of males that associates with increased LA size as an independent risk factor for AF 38, 39. However, Myrstad et al. observed that intensive endurance exercise might also increase AF’s risk among athletic females 40.
4.3.4 Physical activity in individuals younger than 54-60 years old is associated with a higher risk of AF
We do not know yet why PA in individuals younger than 54-60 years is associated with a higher risk of AF. We hypothesize that this finding is caused by the effect of several competing, age-dependent risk factors and protective factors. Nevertheless, we can assume that exercise volume and intensity might be greater in younger individuals than in older individuals with the corresponding increased effects on the autonomous nervous system. Perhaps the susceptibility of the autonomous nervous system by intensive exercise decreases with advanced age? Perhaps intensive exercise makes AF occur earlier in people with a predisposition for the development of AF?
As advanced age on its own also is a risk factor for AF, the risk modifying effect of exercise seems to become less important or may even reduce the risk for AF in individuals older than 54-60 years.
4.3.5 Previous literature
Valenzuela et al.41 first published a meta-analyses review to summarize the evidence on the association between PA/sports practice and AF risk. The authors included 11 meta-analyses in their research. We suggest a slightly different interpretation of the existing body of evidence than the interpretation of Valenzuela et al.. In their summary, they stated that“according to the meta-analytical evidence that is currently available, overall PA does not appear to influence the risk of AF, but sports practice, particularly in endurance events, can increase AF risk.” In contrast to Valenzuela, we interpret the existing body of evidence that moderate PA compared to no PA is associated with a lower risk of AF in a general population. Whereas gender and age were not analyzed by Valenzuela et al., our results suggest that males and patients younger than 54-60 years are more likely to develop AF with increased levels of PA. As Valenzuela et al. we can confirm that athletes are at greater risk of AF compared to non-athletes. An essential aspect of our manuscript is that most of the authors of the included etaanalyses agreed to contribute and approved the results.
Publication bias in the included papers of the conducted metaanalyses was a significant limitation to conclude the association between AF and PA. Possibly, negative or neutral studies were less likely to be published. Furthermore, grey literature often is not considered. Heterogeneity was the other limitation of the included studies in the meta-analyses, which was reported to be significant in most of them. Different study designs, different definitions for PA intensity and duration, different methods of AF diagnosis seem to be the potential causes of heterogeneity, and only some studies’ reasons for the heterogeneity were determined.
Moreover, in case-control studies on athletes with cases and controls belonging to two different populations, the logistic analysis often lacked to be adjusted for confounding factors. Another limitation would be that many studies, e.g., on athletes, did not report the exposure to PA in terms of MET/h-week so that these could not be included in dose-response analysis. Furthermore, a critical limitation of exercise studies showing gender-specific effects is that the intensity of PA is not standardized in any of them. Possibly, what is a high PA for women, could be moderate PA for men. Specific studies with objectively assessed measures of PA (training schedules, accelerometry) should therefore be performed in the future. Finally, the difference between AF risks concerning PA from meta-analyses conducted in athletes and the general population is affected by the different study designs. In particular, estimates from retrospective case control studies conducted in athletes may have overestimated the effect of PA on the AF risk compared to the findings of prospective cohort studies conducted on the general population. However, the magnitude of the AF risk difference between athletes and the general population suggests the concrete existence of a possible association between AF risk and the volume of PA.
Our review suggests that athletes have an increased risk of AF compared to the general population. In the general population, PA has a dose dependent, J-shaped effect on AF risk, with increased risk at very low and very high levels of PA. This effect seems to be genderspecific and more pronounced in younger males. Population groups with a higher risk of AF may benefit from opportunistic screening for AF, especially with cardiac symptoms. Moderate physical activity seems to reduce the risk for AF.
Authorship and Contributorship
All authors mentioned earlier substantially contributed to the conception or design of the work (AM, ASS), or the acquisition, analysis, or interpretation of data (AM, ASS, JM, JA, HA, CR, NDB, CSK, SM, AN, JK, TLLL, SK, ND, SR, AA, AB, GH, MD). Furthermore, all above named authors contributed either to the drafting of the work (AM, ASS) or revised it critically (JM, JA, HA, CR, NDB, CSK, SM, AN, JK, TLLL, SK, ND, SR, AA, AB, GH, MD). All authors finally approved this manuscript and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved (AM, ASS, JM, JA, HA, CR, NDB, CSK, SM, AN, JK, TLLL, SK, ND, SR, AA, AB, GH, MD).
Andreas Müssigbrodt and Alireza Sepehri Shamloo contributed equally to this work and shared their firstauthorship.
Thanks to all authors named in the references for building the scientific base for this work.






