Reversible Mechanical Atrioventricular Block Caused By A Steerable Introducer Sheath During Transseptal Catheterization
Gregory P. Siroky1*, Devendra Bisht1*, Hieu Huynh1, Mena Yacoub1, Shawn Lee1, Seth Keller1, Ranjit Suri1
1Mount Sinai Morningside, Icahn School of Medicine at Mount Sinai, New York, NY 10025.*Drs. Siroky and Bisht contributed equally to this manuscript.
A 62-year-old woman presents for pulmonary vein isolation (PVI) for paroxysmal atrial fibrillation. During transseptal catheterization (TSC) the patient sustained mechanical injury to the atrioventricular node (AVN) with consequent complete heart block (CHB). Injury to the AVN and CHB recovered after approximately forty minutes. The patient subsequently underwent a successful PVI with the remainder of the hospital stay uneventful. We present a case of reversible injury to the AVN caused by a steerable introducer sheath during TSC and discuss the mechanisms of injury as well as potential measures to avoid such a complication in the future.
Key Words : Transseptal Puncture, Mechanical Atriventricular Block, Steerable Sheath.
Gregory P. Siroky, MD
Mount Sinai Morningside Hospital
1111 Amsterdam Avenue
New York, NY 10025
Peri-procedural atrioventricular block (AVB) is hypothesized to be caused by trauma or inflammation of the tissue surrounding the AVN.1,2 It may be caused after aortic valve intervention, alcohol septal ablation, ischemic injury during coronary intervention, ablation near the AV node, or during placement of catheters that mechanically interfere with one fascicle when conduction is already impaired in the remaining conduction system. AVB during transseptal catheterization is an uncommon complication which is hypothesized to be caused by mechanical collision of the sheath with the AVN. Two types of sheaths, fixed curve and steerable, are used for transseptal catheterization depending on availability and the operator’s preference. Steerable sheaths are relatively stiff and exert greater force on underlying cardiac structures compared to a fixed curve sheath. Being a subendocardial structure, the AVN may be susceptible to mechanical trauma as a result of catheter placement on or near the area, however, the occurrence of reversible AVB caused by a steerable sheath is rare and likely underreported. We present a case of reversible AVB secondary to sheath-induced trauma to the AVN during TSC.
A 62-year-old woman presents for pulmonary vein isolation (PVI) in treatment of symptomatic paroxysmal atrial fibrillation (PAF). A pre-ablation cardiac computed tomography (CT) scan showed a common left sided pulmonary vein (PV), normal PV anatomy on the right side, and a dilated main pulmonary artery suggestive of pulmonary hypertension. Electrocardiography (EKG) showed sinus bradycardia with normal QRS duration [Figure 1A]. The echocardiogram showed left ventricular hypertrophy (LVH) and mild left ventricular systolic dysfunction.
Figure 1. (A) Pre-procedure electrocardiogram showing sinus bradycardia and left ventricular hypertrophy with strain pattern. (B) Intra-procedural development of complete heart block. (C) Resolution of AV block and resumption of normal conduction with normal HV interval.
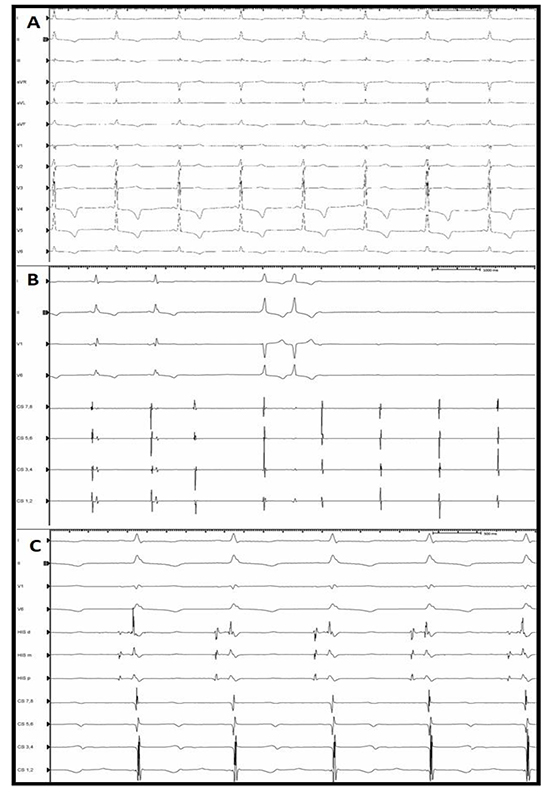
Right and left femoral venous access was obtained to advance a diagnostic decapolar catheter and an intracardiac echo (ICE) catheter to the coronary sinus (CS) and mid right atrium (RA), respectively. In anticipation of transseptal catheterization (TSC) the ICE catheter was positioned to visualize the interatrial septum (IAS). A 0.032-inch J-tip guidewire was advanced under fluoroscopic guidance from the right femoral vein to the superior vena cava (SVC). Keeping the same fluoroscopic and ICE projections, an 8.5F steerable introducer sheath (Agilis NXT, 16.8 mm St Jude Medical, MN, USA) was advanced over the guidewire to the SVC. Once the sheath was 3 to 4 cm superior to the cavoatrial junction, the wire was removed, keeping the tip of the sheath facing leftward in an AP view. The Brockenbrough TSC needle with stylet was advanced to within 3 cm of the sheath tip. The stylet was removed and the needle and the sheath were gradually pulled down with the Brockenbrough needle arrow maintained at a 5 o’clock position. During the descent of the sheath and needle assembly, the IAS was monitored for tenting using the ICE catheter. The Agilis sheath was felt to be too anterior in the fossa ovalis and this was confirmed by ICE and fluoroscopy in a right anterior oblique (RAO) view. When clockwise torque was applied to the Agilis sheath to direct the tip more posteriorly, the patient developed complete AVB [Figure 1B]. The decapolar (CS) catheter was immediately advanced to the right ventricular apex to provide ventricular pacing.
After an almost forty-minute waiting period, during which the patient was hemodynamically stable, AV nodal conduction returned [Figure 1C]. Following resolution of CHB, TSC was performed uneventfully with a standard, fixed curve Swartz braided SL-1 transseptal (TS) sheath (St. Jude Medical, MN, USA), Brockenbrough TS needle, and Safesept wire (Cardio medical products, INC, USA) using fluoroscopic and ICE guidance. The SL-1 sheath was exchanged for the Agilis sheath using an Amplatz exchange wire. PVI was performed without incident and the rest of the hospital stay was uneventful.
Atrioventricular conduction disturbance during AF ablation is a rare complication and has been reported during cryoablation.4,5 It has been described that during cryoablation, mechanical bumping of the AVN during cryo-energy delivery around the right inferior pulmonary vein as well as vagally mediated reactions are potential mechanisms for transient AV block.
In our patient, AVB likely occurred due to mechanical, traumatic injury to the AVN during manipulation of the steerable, Agilis sheath, despite fluoroscopic and intracardiac echocardiographic guidance. Clockwise torque applied to direct the sheath posteriorly across the mid part of septum likely traumatized the AVN resulting in conduction block. The degree of AV block was determined to be at the level of the AVN as there was no evidence of distal conduction disease once normal conduction resumed [Figure 1C].
While in our case, AV block lasted for about 40 minutes, Schweiss et al. reported a case of transient heart block which lasted for a total of 3 days.6 In addition, it was the only reported case found in the literature of traumatic injury to the AV node leading to prolonged CHB during TSC. The authors initially believed that the heart block occurred after ablation of a left lateral accessory pathway as a result of damage to the left lateral extension of the AV node, however, after close inspection of the electrograms, they determined that injury occurred to the AV node during TSC. The only piece of information lacking from their case report was the type of sheath used during the TSC.
Steerable sheaths are being increasingly used for PVI which allows better catheter stability in addition to achieving target contact forces of 10-40gms for ablation lesions.7 As shown by Reddy et al. in the TOCCASTAR study, there was a higher median contact force when using a steerable sheath (Agilis) versus a fixed curved sheath (23.3grams vs. 14.6grams).8 While contact force is not directly monitored during TSC, it can be extrapolated to our case that a steerable sheath can be more prone to cause mechanical damage to the compact AV node compared to a fixed curve sheath.
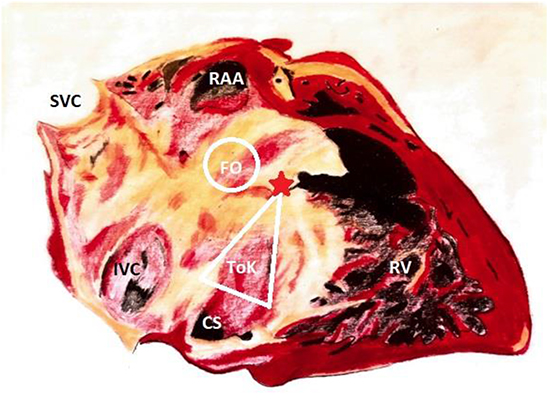
In addition, a basic knowledge and understanding of the cardiac anatomy is required for a safe and successful TSC [Figure 2]. The initial positioning of our sheath prior to TSC was likely too anterior, near the region of the compact AVN, and with clockwise torque to position the sheath more posteriorly, the tip of the sheath mechanically injured the AVN leading to complete heart block.
Figure 2. Right anterior oblique view of the right sided cardiac anatomy demonstrating proximity of the compact AV node (red star) to the fossa ovalis (FO). SVC = superior vena cava; IVC = inferior vena cava; CS = coronary sinus; ToK = triangle of Koch; RV = right ventricle; RAA = right atrial appendage. (Illustrated by Shawn Lee, MD and adapted from Alkhouli et al. J Am Coll Cardiol Intv. 2016;9(24):2465-80)9.
Based on the above and the development of AVB during this case we propose that TSC be performed with a standard fixed curve sheath (e.g. Swartz braided SL-1 transeptal sheath), which can then be exchanged over a wire for a steerable sheath (e.g. Agilis NXT, 16.8 mm St Jude Medical, MN, USA). Alternatively, TSC can be performed with the VersaCross® system (Baylis Medical, Montreal, QC, Canada) which is a needleless apparatus utilizing a stiff radiofrequency-powered pigtail wire advanced through a softer guiding sheath. Once through the atrial septum, the stiff pigtail wire provides adequate support for an exchange to a stiffer steerable sheath. In addition, in this era of routine ICE use for TSC we must still use the RAO projection to ensure that we are not starting too anterior with the transseptal assembly.
We present a rare case of reversible AVB caused by mechanical injury to the AV node during transseptal catheterization by a steerable introducer sheath. This case highlights the critical role of imaging and hardware selection during transseptal catheterization. The approach we suggest of using a fixed curve sheath for initial transseptal access may avoid this complication and allow for safer TSC.






