Hemoptysis post Radiofrequency Ablation of Atrial Fibrillation
Ana de Leon1, Simon Hansom1, Sanoj Chacko1, Adrian Baranchuk1, Andres Enriquez1
1Division of Cardiology, Queen’s University, Kingston, Canada.
Key Words : Pulmonary hemorrhage, Catheter ablation, Atrial fibrillation.
Dr. Andres Enriquez MD
Division of Cardiology, Queen’s University
76 Stuart Street, Kingston, Ontario K7L 2V7
A 41-year-old female with symptomatic paroxysmal atrial fibrillation (AF), intolerant to antiarrhythmic drugs, was referred for catheter ablation. The patient had an elevated body mass index with no other significant comorbidities. She underwent an elective radiofrequency (RF) pulmonary vein isolation under general anesthesia (GA) with pressure-controlled ventilation volume-guaranteed (PVC-VG) (tidal volume 500 ml, respiratory rate 12 breath/min, peak airway pressure 25 cmH20, positive end-expiratory pressure 5 cmH20). Intravenous unfractionated heparin was administered during the procedure, with a mean and maximum activated clotting time (ACT) of 250 and 267 seconds, respectively. The procedure was well tolerated, no ventilatory issues were observed and she required transient non-invasive ventilation with CPAP after extubation. Anticoagulation was partially reversed with protamine at the end and Apixaban was restarted 4 h after removal of sheaths. The patient was discharged the following morning.
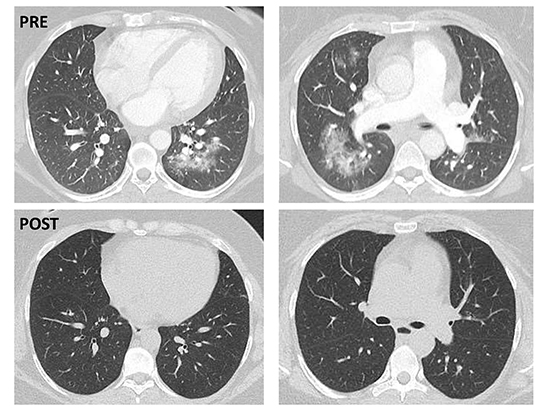
Six days post-ablation, the patient presented with dyspnea on minimal activity, cough, and blood in her sputum. Computed tomography (CT) of the chest with contrast revealed multifocal groundglass opacities surrounding the perihiliar pulmonary vasculature within the upper and lower lobes bilaterally, suggestive of alveolar hemorrhage ([Figure 1], upper panel). The pulmonary arterial phase ruled out acute pulmonary embolism and there was no evidence of pulmonary vein stenosis. She was admitted to Intensive Cardiac Care for monitoring. Anticoagulation was temporarily discontinued. A complete rheumatology panel was negative. The hemoptysis gradually resolved within the next 24 h and she was discharged home after 3 days with only occasional dry cough. Anticoagulation was restarted 48 hours post discharge without recurrence of hemoptysis. A repeat CT scan, 3 weeks following initial imaging, revealed complete resolution of the pulmonary infiltrates ([Figure 1], lower panel).
Figure 1. Upper Panel, Lower Panel
Hemoptysis is a rare complication of AF ablation. The differential diagnosis includes conditions such as pulmonary embolism or pulmonary vein stenosis, but the latter typically develops weeks to months post procedure1. Hemoptysis has also been described post cryoballoon ablation due to bronchial trauma or cryoinjury to the lung parenchyma2. Only a few cases of alveolar hemorrhage related to RF ablation have been reported3. Possible etiologic factors that have been postulated include mechanical ventilation-induced lung injury, the effect of high-dose intraprocedural anticoagulation, idiosyncratic lung injury related to anesthetic agents, and negative pressure pulmonary hemorrhage due to acute upper respiratory obstruction during extubation. The first two mechanisms seem unlikely in this case as the ACT levels were lower than usually used in most left atrial ablations and the ventilation mode used in our patient is associated with lower incidence of barotrauma compared to other modes4.
Alveolar hemorrhage is a potentially serious complication associated with RF ablation of AF. The mechanism is not clearly understood. Post procedure acute hemoptysis should raise suspicion and a chest CT is indicated. Mild cases as the described above may resolve after a short period of anticoagulation interruption.






