Safety of Atrial Fibrillation Ablation in the Young – A Real World Analysis
Naga Venkata K Pothineni1, Dinesh Voruganti2, Kanishk Agnihotri2, Rakesh Gopinathannair3, Dhanunjaya Lakkireddy3, Pasquale Santangeli1
1Division of Cardiology, University of Pennsylvania, Little Rock, AR, USA.2Divison of Cardiology, University of Arkansas, Little Rock, AR, USA.3Kasnas City Heart Rhythm Institute, Overland Park, KS, USA.
Key Words : Atrial Fibrillation, Complications, Safety, Young.
Naga Venkata K Pothineni, MD
Division of Cardiovascular Medicine,
University of Pennsylvania
9 Founders, 3400 Spruce street, Philadelphia, PA, USA
Atrial fibrillation (AF) is the most frequently encountered cardiac arrhythmia seen in clinical practice, with an estimated prevalence expected to increase to an estimated 12.1 million by the year 2030.1 While most frequently encountered in the elderly, a significant proportion of younger adults are diagnosed with AF as well. It is with an estimated 1% of patients with AF are less than 60 years of age.1 Young patients with earlier onset of AF are exposed to a life time risk of recurrences, tachycardia-mediated cardiomyopathy, heart failure and stroke. In addition, long term adverse effects of anti-arrhythmic therapy and anticoagulation can be additive.3 To avoid risks from long-term medical therapy, it could be hypothesized that an early catheter ablation approach would be reasonable in younger patients who present with AF. However, safety data of AF ablation in this cohort is limited. We sought to examine the utilization and complications of AF ablation in younger patients (≤50 years) and compare with complication rates in older patients (> 50 years).
We identified all patients that underwent AF ablation using data from the National Inpatient Sample (NIS) from 2005 to 2014. Trends in utilization of AF ablation in the two age groups (<50 and >50 years) was computed. Rates of in-hospital procedural complications were analyzed and compared between the two groups. All statistical analysis was conducted using SPSS (IBM SPSS, Version 27.0. Armonk, NY).
A total of 112,998 AF ablations were identified within the NIS between the years 2005 to 2014, and were included in our analysis, which was weighted in order to represent the general U.S. population. Majority of the ablations occurred in the older patient group with about one-sixth of ablations performed in patients >50 years of age (n = 15,832). Trends in utilization of AF ablations stratified by age group is shown in the [Figure]. Mean age was 43.18±6.6 years in the younger age group. There was a significantly higher proportion of African Americans (6% vs. 3%) and Hispanics (6.2% vs. 2.9%) in the younger cohort compared to those >50 years. Prevalence of comorbidities such as diabetes, hypertension, peripheral vascular disease and obesity (p < 0.0001 for all) were also significantly lower in the younger cohort. A large majority (81.1%) of younger patients were privately insured while about half (52%) of patients >50 years of age had Medicare as the primary payer. Rate of in-hospital complications were significantly lower in the younger age group than in the older age group [Table]. Younger patients had significantly lower rates of vascular complications requiring surgery, cardiac tamponade, pneumothorax, need for pericardiocentesis, post-operative stroke/TIA, as well as AV fistula formation (p < 0.002 for all). Mean length of stay for those <50 years was 1.97 days compared to 2.38 days for those >50 years.
Figure 1. Trends in utilization of AF ablation stratified by age group. Primary Y axis on left depicting utilization of AF ablation in patients >50 years. Secondary Y axis on right depicting AF ablation utilization in patients >50 years.
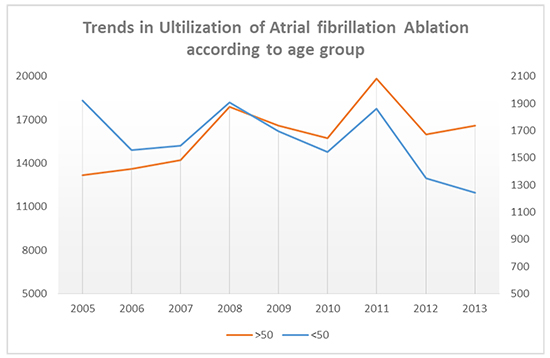
Table. Comparison of In-hospital Complications of Atrial fibrillation ablation in young (<50 years) patients with those >50 years old
|
Age ≤ 50(n = 15, 832) |
Age > 50(n = 97,165) |
Total(n=112998) |
P-value |
| Vascular Complications requiring Surgery (%) |
0.06 |
0.22 |
0.2 |
<0.0001 |
| AV fistula (%) |
0.03 |
0.12 |
0.11 |
0.0016 |
| Hemopericardium (%) |
0.29 |
0.36 |
0.35 |
0.1719 |
| Cardiac Tamponade (%) |
0.58 |
1.03 |
0.97 |
<0.0001 |
| Pericardiocentesis (%) |
1.15 |
1.79 |
1.7 |
<0.0001 |
| Stroke/TIA (%) |
0.46 |
0.85 |
0.79 |
<0.0001 |
Our analysis suggests that younger patients <50 years of age comprise about one-sixth of all AF ablation procedures performed in the United States. Young patients have shorter lengths of stay and significantly lower in-hospital complication rates compared to those >50 years of age. These findings are similar to other smaller single center studies that have been reported previously which demonstrated safety and efficacy of AF ablation in younger patients with excellent rates of arrhythmia free survival.3-5 In these prior studies, ablation was offered as second-line therapy to patients with drug-refractory AF. This practice is in accordance with current AHA/ACC guidelines for management of AF, with first-line catheter ablation for AF is listed as a class IIB recommendation1. However, our analysis suggests that a lower threshold to offer ablation to younger patients with AF as first line therapy may be reasonable given its efficacy and safety, and merits further study. Lower rates of overall complications should also be utilized during shared decision making while discussing AF ablation with younger patients.






