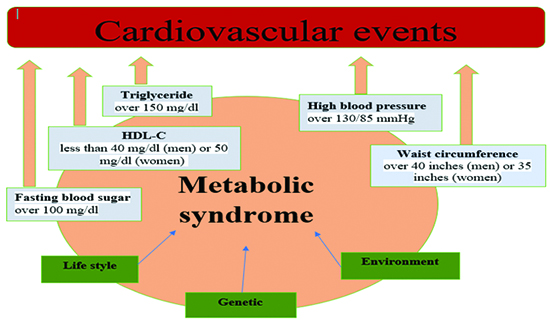
Metabolic syndrome (MetS) is a collection of conditions such as hypertension, obesity, insulin resistance, and dyslipidemia. Also, defined as a cluster of metabolic risk factors and this clustering category of metabolic syndrome is known as syndrome X. Various terms are used to refer to the Metabolic Syndrome in individuals like insulin resistance syndrome, metabolic syndrome X, and Reaven's syndrome. The primary clinical outcomes of metabolic syndrome are cardiovascular diseases. The prevalence of metabolic syndrome increases as age is increasing and in the USA about 34% of adult populations have Metabolic Syndrome 1,2. The defining criteria of metabolic syndrome, according to the National Cholesterol Education Program Adult Treatment Panel III guidelines, 3 explains in [Flowchart 1].
Flowchart 1 Metabolic syndrome leads to cardiovascular diseases: The defining criteria of metabolic syndrome according to the National Cholesterol Education Program Adult Treatment Panel III guidelines3.
Atrial Fibrillation (AF) is a common kind of cardiac arrhythmia in which heartbeats rate excess from normal rate and is mostly found in the elderly population which has increased the rate of mortality, morbidity, and disability. The risk of stroke, heart attack, and death rates have increased due to AF 4-6. Similarly, the pathogenesis of AF has been caused due to the numerous components of metabolic syndrome which affect AF triggers or the atrial substrate 7. In the same way, the initiation and maintenance of AF are due to the atrial electrical, electrical remodeling (changes the ion channel function and calcium handling of the cells) and structural remodeling. Numerous components of metabolic syndrome cause remodeling of the atrial. Interstitial fibrosis with structural remodeling leads to heterogeneous electrical substrates with differences in conduction velocities which promotes AF 8,9.
Furthermore, Watanabe et al. study had concluded that an increased risk of AF was linked to metabolic syndrome and metabolic derangements of the syndrome that might be important for the pathogenesis of AF 10. Similarly, Mechanical stress in the atrium might predispose the AF which was caused by metabolic syndrome whereas, electrophysiological remodeling, as well as structural remodeling, are criteria for atrial fibrillation to perpetuate 11-14. Likewise, the structural substrate such as dilatation, fibrosis, atrial stretch, at gap junctions’ disruption of cell coupling has occurred, and loss of muscle mass 11-13. In the same way, the integral components of metabolic syndrome including obesity and hypertension might cause atrial dilatation and stretch which had been resulted in a structural substrate predisposing to AF 15,16.
Further, Nicolaou et al study had reported that enlargement of an atrium in patients with nonvalvular AF was linked to metabolic syndrome 17. Also, structural remodeling might change the cellular electrophysiology which resulted in AF. During the episodes of atrial fibrillation, the rapid atrial rates could lead to further atrial remodeling, more frequent and severe episodes of atrial fibrillation a phenomenon recognized as “AF begets AF 18,19.
In addition, A biomarker or biological marker is a measurable indicator of some biological state or condition. It is used to evaluate or measure the normal biological process, pharmacologic response, and pathogenic processes to a therapeutic intervention. So, In MetS, many different biomarkers are used in the early detection and risk stratification in MetS patients and their role in cardiovascular diseases. It includes leptin, Interleukin-6, Tumor Necrosis Factor -Alpha, uric acid, Interleukin-10, ghrelin, adiponectin, paraoxonase, oxidized LDL, plasminogen Activator inhibitor – 1 20,21.
In this review article, we provided an overview and focus on the basic role of different biomarkers of metabolic syndrome and mainly focus on pathophysiological aspects of different biomarkers of metabolic syndrome in Atrial Fibrillation. There are many biomarkers of metabolic syndrome. However, our review article focuses only on adiponectin, leptin, Leptin/ Adiponectin ratio, TNF-α, Interleukin-6, Interleukin-10, PTX3, ghrelin, uric acid, OxLDL, and their pathophysiological role in the development and progress of AF. In conclusion, we have provided a viewpoint on the recent pathophysiological role in AF.
Different databases including Google Scholar, PubMed, and Science direct were used to review the literature. The last date of the search was 10 July 2021. Many keywords were used for searching the literature such as metabolic syndrome, Atrial Fibrillation, interleukin- 6, interleukin -10, tumor necrosis factor-alpha, uric acid, leptin, adiponectin. The language of clinical studies was restricted to English. We did not limit the time frame although more recent studies were favoured.
Role of a major biomarker of Metabolic syndrome in AF
According to the literature, there are many biomarkers of metabolic syndrome. However, this review article has discussed only major biomarkers of metabolic syndrome such as adiponectin, leptin, leptin/adiponectin ratio, TNF-α, interleukin-6, interleukin-10, Pentraxin-3, ghrelin, uric acid, and Oxidized Lipoprotein Lipase which played their pathophysiological role in atrial fibrillation as explained in [Table 1].
Table 1. Summary of pathophysiological aspects of major Biomarkers of metabolic syndrome in AF
| Biomarkers of MetS |
Pathophysiological aspects in AF |
| Adiponectin |
. Atrial remodeling
. Elevated serum carboxy-terminal telopeptide of collagen type I (CITP)
. The pathogenetic aspects of AF were inflammation, atrial remodeling, and autonomic imbalance
. Influence cardiac remodeling.
|
| Leptin |
. Played electrophysiological effects through ionic profiles, contractility as well as changing action potential morphology
. To contribute to Angiotensin II- evoked AF and atrial fibrosis
. Reduces the effect of isoproterenol-induced arrhythmogenesis- irregular rhythm or rate of heartbeat
. Play favourable role in the pathophysiology of atrial arrhythmogenesis |
| TNF-α |
. More severe leukocyte infiltration, and more fibrosis
. Increased Left atrial diameter
. Atrial electrical remodeling
. Abnormalities in action potential propagation and Ca2+ handling
. Increase the PV arrhythmogenic activity and impair the calcium regulation
. Associated with atrial fibrosis
. Electrical, autonomic, structural, and contractile remodeling
. Changed connexin-40 expression |
| IL-6 |
. Increased left atrial size
. Rapidly induce atrial electrical remodeling by down-regulating cardiac connexins |
| IL-10 |
. Weakening the development of inflammatory atrial fibrosis |
| PTX-3 |
. The local production of the left atrium could reflect the local inflammation of atrial fibrillation |
| Ghrelin |
. Atrial fibrosis due to atrial structural remodeling which resulted in repolarization by interfering with atrial excitement as well as pulse transfer, and differences in atrial conduction.
. Cause changes in atrial ion channels which in turn could elevate the likelihood of repolarization and promote the onset of AF |
| Uric acid |
. Left atrial and left ventricular remodeling
. Causes atrial remodeling by oxidative stress, endothelial dysfunction, inducing inflammation, RASS activation
. Causes electrical remodeling
. Shortens the atrial refractory period
. Establishes a reentry circuit in the atrium
. Structural remodeling
. Slows the velocity of conduction, thereby allowing reentry. |
| OxLDL |
. Maximum diameter of the left atrium |
Adiponectin is produced from adipocytes and its high-molecular-weight form play role in most potent metabolic activity and circulating levels are higher in females as compared to males due to the stimulating activity of testosterone on adiponectin secretion 21. Moreover, an important role in metabolic balance and increases the risk of vascular, metabolic, and cardiac due to its low levels. Likewise, Maroni et al. study has reported decreased levels of adiponectin in metabolic syndrome patients 22. Conversely, Matsuzawa et al. study also demonstrated the positive effect on metabolic protection mainly in the atherogenic process by potentially inhibitory activity 23. On the contrary, Fu Y study et al. have conducted to show that metabolic syndrome components were inversely related to adiponectin levels and have beneficial effects on metabolic disorders 24.
Furthermore, Shimano et al. (2008) conducted a study that explained the atrial remodeling in atrial fibrillation occurred due to obesity-related conditions. Adiponectin has a beneficial effect on ventricular remodeling. So, the study has examined the potential link between atrial remodeling and circulating high plasma levels of adiponectin in AF patients. In conclusion, the authors had reported the elevated plasma levels of adiponectin were linked to the presence of persistent AF with elevated serum carboxy-terminal telopeptide of collagen type I (CITP). So, measuring the adiponectin plasma levels would be useful for the assessment of AF 25.
In contrast, Choi et al. study in 2012 has analyzed the beneficial effects of adiponectin on cardiac function and reported the association with glucose metabolic, insulin resistance, and glucose metabolic. In obese individuals, serum levels of adiponectin were decreased as compared to the non-obese individual. The increased incidence of atrial fibrillation was linked to obesity. In conclusion, the paroxysmal AF was significantly linked to the lower plasma levels of adiponectin. The important risk of AF could be potentially hypoadiponectinemia 26.
Moreover, in 2018, Kim et al study have revealed the independent relationship between AF recurrence after catheter ablation for paroxysmal AF with elevated circulating levels of adiponectin in younger subjects than 65 years old individuals 27. Besides, Macheret et al study examined the association between the high incidence of atrial fibrillation in an elderly population with elevated adiponectin concentration 28. Similarly, according to the previous studies, it might be hypothesized that the link between AF and adiponectin might be age and gender-dependent. In addition, the pathogenetic aspects of atrial fibrillation were inflammation, atrial remodeling, and autonomic imbalance 29-31.
On the other hand, Ybarra et al. study revealed a novel inverse link between left atrial size with adiponectin which might inhibit atrial interstitial fibrosis as well as reverse atrial remodeling. More, adiponectin might be a connection between the heart and adipose tissue that influence cardiac remodeling 32.
Leptin is a hormone that produces from adipose tissue and is secreted mainly from white adipose tissue, but also produced from non-adipose ones such as the immune system, placenta, mammary gland, and stomach 33,34. Its regulation is achieved through numerous factors dependable on the metabolic status. The pathogenic mechanisms of leptin comprise obesity syndrome, metabolic dysfunctionalities, energy homeostasis, bone metabolic, and neuroendocrine function. The different mechanisms follow similar targets to cause the pathogenic pathways of leptin 33. When leptin binds to its functional receptor and activates numerous transduction pathways, for instance, mitogen-activated protein kinase, Janus kinase JAK/ single transducers, activators of transcription, AMP-activated protein kinase, and phosphatidylinositol -4, 5- bisphosphate 3-kinase/ protein kinase B 35,36.
In addition, various studies have been confirmed that leptin levels correlate mainly with waist circumference and obesity. Under normal physiological conditions, leptin helps to reduce appetite, increase sympathetic activity, increase energy expenditure, improve insulin sensitivity and facilitate glucose utilization 37.
Obesity is an independent risk factor for the development of AF. So, obesity increase the prevalence of ischemic heart disease, hypertension, ventricular dysfunction, and congestive heart failure that might be contributed to the process of AF 38-40,10. Similarly, Lin et al studies conduction in 2012 and 2013 have reported that Adipose tissues could yield many adipokines that have played electrophysiological effects through ionic profiles, contractility as well as changing action potential morphology 41,42.
Moreover, Fukui et al revealed that leptin signaling has been shown to contribute to angiotensin II- evoked AF and atrial fibrosis 43. Likewise, Lin et al reported that Leptin regulates the Left Atrial electrophysiological features and calcium homeostasis. Leptin reduces the effect of isoproterenol-induced arrhythmogenesis- irregular rhythm or rate of heartbeat, which may play a favourable role in the pathophysiology of atrial arrhythmogenesis 42.
3.Leptin/Adiponectin Ratio
Adipocytes secrete from the two key hormones such as leptin and adiponectin. They both play several important physiological mechanisms. Their central role is in energy homeostasis and a marker of metabolic derangement 44. Likewise, Metabolic syndrome and obesity are categorized by elevated levels of leptin concentration in circulation which are corresponding to lower levels of adiponectin in blood. The leptin/adiponectin ratio is a marker of adipose tissue dysfunction. The leptin/ adiponectin ratio is associated negatively with Body Mass Index (BMI). It is powerfully connected with surrogate measures of insulin resistance (IR) such as homeostatic model assessment (HOMA) and the quantitative insulin sensitivity check index (QUICK) formulas for the measurement of insulin resistance. It is interrelated with insulin resistance better as compared to leptin and adiponectin values alone, even HOMA. The normal value of adiponectin/leptin ratio is equal or larger to 1.0 while the moderate -the medium risk is increased when its ratio is between 0.5 and 1.0, severe risk of cardiovascular diseases is indicated when the ratio is below 0.5 45-47.
In addition, Finucane et al had reported that in non-diabetic adults, LAR is a useful marker of insulin resistance 48. Furthermore, increased waist circumference increased vasoconstriction due to angiotensin II and decreased vascular response to acetylcholine were accompanying the imbalance of leptin/adiponectin. Both leptin and adiponectin have contradictory effects on subclinical inflammation and insulin resistance. Insulin resistance and type 2 diabetes mellitus are linked to proinflammatory cytokines such as interleukin-6 and TNF-α which are upregulated by leptin. In dissimilarity, adiponectin has anti-inflammatory properties and downregulates the expression and release of several pro-inflammatory immune mediators. Leptin/ adiponectin imbalance and angiotensin II are interrelated which are mediators of amplified risk of cardiovascular diseases and developing type 2 diabetes linked to abdominal obesity 49.
4.Tumoral necrosis factor-alpha
Tumoral necrosis factor-alpha is an inflammatory cytokine that is mostly formed by macrophages cells, also from another type of inflammatory cells. It is an acute inflammatory response protein that increased C- reactive proteins concentration and also regulates insulin resistance by interacting with insulin receptors 50. Similarly, it played role in the regulation of lipid metabolism, adipokines synthesis as well as cholesterol metabolism 51.
Furthermore, Tumoral necrosis factor-alpha might be formed by inflammatory cells from the dysfunctional adipose tissue, like Interleukin-6. Numerous studies have shown that Tumoral necrosis factor-alpha is linked with all the components of metabolic syndrome that are involved in numerous metabolic syndrome pathways and alterations, in IR through a similar mechanism of Mammalian target of rapamycin (mTOR) and protein C kinase activation and systemic inflammation 52.
Moon et al study confirmed that tumor necrosis factor-alpha had a higher concentration in obese patients, even elevated levels in male subjects. Likewise, Body Mass Index, triglycerides, waist circumference, and diastolic blood pressure were positively correlated with tumor necrosis factor-alpha. But TNF-α was inversely correlated with HDL cholesterol but after adjustment for Body Mass Index and waist circumference, only the association with triglyceride levels persisted 53. Similarly, Sookoian et al conducted a meta-analysis on 16 homogeneous studies that shown that systolic blood pressure, obesity, and serum insulin levels were positively correlated with tumor necrosis factor-alpha -308A gene variant and govern 23 per cent increased risk to develop the metabolic syndrome 54.
Moreover, TNF-α involvement has been shown in the pathogenesis of chronic Atrial Fibrillation. Valvular Atrial Fibrillation patients showed high levels of TNF-α, more severe leukocyte infiltration, and more fibrosis. Higher TNF-α levels in the plasma and left atrial diameter in patients with rheumatic heart disease and chronic AF. Higher plasma interleukin-6 correlated with the presence and duration of AF and increased left atrial diameter 55.
Similarly, Saba et al. study explained the growing evidence that indicates the atrial electrical remodeling has been caused due to the tumor necrosis factor-alpha in which atrial myocytes isolated from failing heart overexpressing tumor necrosis factor-alpha, abnormalities in action potential propagation and Ca2+ handing which could contribute to the initiation and maintenance of re-entrant atrial arrhythmias including flutter and AF 56.
Ren et al. study had confirmed the comparison between control pulmonary vein (PV) cardiomyocytes, the tumor necrosis factor-alpha- treated pulmonary vein cardiomyocytes had a significantly larger amplitude of the delayed afterdepolarizations (DADs), larger transient inward currents, a smaller intracellular calcium transient, large diastolic intracellular calcium, a decreased sarcoplasmic reticulum ATPase (SERCA2a) expression, a longer decay portion of the calcium transient, larger Na+ – Ca2+ exchanger currents, smaller ICaL and a longer decay portion of the calcium transient. In conclusion, these findings had suggested that tumor necrosis factor-alpha could increase the PV arrhythmogenic activity and impair the calcium regulation, thereby causing inflammation-related AF 57.
In the same way, Deng et al. also demonstrated that tumor necrosis factor-alpha increased levels in the plasma as well as left atrial tissue which had a positive association with left atrial diameter in patients of chronic atrial fibrillation. It has resulted from rheumatic heart disease which collectively shown that tumor necrosis factor-alpha was strongly associated with atrial fibrosis in AF subjects 58. Also, Tumor necrosis factor-alpha play’s role in atrial remodeling including electrical, autonomic, structural, and contractile remodeling. It has been substrate for atrial fibrillation maintenance which has anti TNF- α therapeutic strategy for atrial fibrillation is theoretically appropriate 57.
Another study had concluded that tumor necrosis factor-alpha is involved in the pathogenesis of atrial fibrosis and changed connexin-40 expression in mice through the Transforming growth factor-beta / TGF-β signaling pathway increased secretion of Matrix metalloproteinases (MMPs) and activation of myofibroblasts. In summary, these changes might contribute to the arrhythmogenic substrate and processes of atrial fibrillation 59.
Interleukin-6 (IL-6) has played role in acute and chronic inflammation, the pathogenesis of the autoimmune disease, and immune cell development. It has increased the risk of developing diabetes mellitus that is linked with increased activity of the interleukin-6 gene 60. Similarly, interleukin-6 is associated with all the components of the inner immunity and produced a pro-inflammatory effect. Despite that, various studies have been conducted to confirm that interleukin-6 also controls the process involved in the resolution of inflammation and also focuses on its anti-inflammatory function 61. Various studies have been reported to confirm that interleukin-6 is associated with all five metabolic syndrome components but the main fact explains the dysfunctional adipose tissue has encourages macrophagic proliferation with an elevated level of interleukin- 6 production 62.
Likewise, Weiss et al. have investigated that interleukin-6 is linked with fasting plasma glucose, hypertension, and hypertriglyceridemia 63. Similarly, Sarbijani et al. also gave the same result which has reported that elevated levels of interleukin-6 are related to metabolic syndrome severity 64.
Furthermore, the increased left atrial size was linked to the interleukin-6 because it is a well-known risk factor for atrial fibrillation. The authors have given the possibility in which interleukin-6 may result in atrial fibrillation because of left atrial remodeling 65. In the same way, Psychari et al. study also shown the significant association between interleukin-6 with increased left atrial size which is an important risk factor for atrial fibrillation 66. Additionally, postoperative atrial fibrillation has been linked to the polymorphisms in the promoter region of the interleukin-6 67,68.
Besides, Gaudino et al. study had analyzed that the -174G/C lL-6 promoter gene variant could modulate the inflammatory response to surgery and also influence the development of postoperative AF. They suggested that inflammatory component of postoperative atrial arrhythmias as well as a genetic predisposition to this complication 67. Similarly, Marcus et al. study has concluded that CAD subjects had increased levels of interleukin-6 and interleukin-6 -174CC genotype that were significantly linked to AF. The authors did not find any association with other biomarkers such as CRP. In the end, the authors had suggested which interleukin- 6 is a uniquely important mediator in the pathophysiology of AF 69.
In the same line, Conway et al. study had concluded the existence of an inflammatory state such as elevated plasma interleukin-6, plasma viscosity, and CRP among the typical population with chronic atrial fibrillation. These indexes of inflammation are related to indexes of the prothrombic state which was also connected to the clinical variables including underlying vascular disease and co-morbidities rather than simply to the existence of atrial fibrillation itself 70.
Moreover, the Lazzerini study had given the suggestion systemic inflammation including elevated levels of interleukin-6 could rapidly induce atrial electrical remodeling by down-regulating cardiac connexins. These changes could significantly increase the risk for AF and related complications during active inflammatory processes 71.
Interleukin -10 (IL-10) is a powerful anti-inflammatory cytokine that played role in the immune response to stop excessive activation and auto-damage, also in modulating insulin resistance and development of atherosclerotic 72. Moreover, a cross-sectional study has been conducted on children and young adolescents, they have found that the plasmatic level of interleukin-10 was lower in obese or overweight children. Then, they concluded that interleukin-10 might be a marker of metabolic risk 73. Interleukin-10 family members might induce numerous host defence processes against diverse infections, encourage innate immune response to alleviate infection-induced damage, sustain the integrity and homeostasis of tissue epithelial layers. Moreover, even after viral or bacterial infections, these factors can accelerate the process of tissue healing 74.
In contrast, Esposito et al. reported that interleukin-10 levels were decreased in obese as compared with normal-weight women, but were lower in both groups that had metabolic syndrome criteria 75. Similarly, Van Exel et al reported that reduced plasmatic levels of interleukin-10 in patients with metabolic syndrome and diabetes mellitus 76. A recent study had conducted to explain the balance between inflammatory and anti-inflammatory including tumor necrosis factor-alpha and interleukin-10 which had been linked to atrial fibrillation recurrence after catheter ablation 77.
In contrast, Krishnamurthy et al. study had a conclusion which suggested that interleukin- 10 reduces the severity of proinflammatory responses and contributes to improving left ventricular function and remodeling with effects on Matrix metallopeptidase 9 (MMP-9) activation, fibrosis, and angiogenesis after Myocardial infarction which had happened due to the activation of signal transducer and activator of transcription 3 (STAT3) and suppression of p38 Mitogen-activated protein kinases (MAPKs) 78. Additionally, Kondo study had examined that interleukin-10 plays a vital role in weakening the development of inflammatory atrial fibrosis and susceptibility to atrial fibrillation in mice with high-fat diet-induced obesity. In the obese human population, interleukin-10 could be a novel therapeutic way to stop atrial fibrillation 79.
Pentraxin-3 is a marker of local and general inflammation and immune response. Immune cells produced the PTX3 as a response to endotoxins, IL-1, bacterial substance and tumor necrosis factor-alpha. PTX3 has very low serum levels because it is an acute-phase protein. The levels of PTX3 rapidly raise as a response to diverse inflammation stimuli 80-82.
Recent studies have reported the association between increase PTX3 levels with the development and progression of metabolic syndrome. Likewise, Kardas et al study has reported that PTX3 levels were higher in subjects with obesity and metabolic syndrome. Moreover, they also have observed that increased PTX3 levels were linked with high triglycerides as well as low HDL cholesterol 83. Similarly, Zanetti et al revealed that independent association between low HDL cholesterol level with PTX3 and in patients with metabolic syndrome and subclinical atherosclerosis had a higher level of PTX3 84. Further, a recent study found that after multivariate analysis, the severity of metabolic syndrome correlates with PTX3 which in turn correlation persisted for glucose level, HDL cholesterol and waist circumference 85. As a result, PTX3 might be a valuable biomarker of metabolic syndrome prediction and needs further studies.
Moreover, Saeki et al study also demonstrated that PTX3 in the local production of the left atrium could reflect the local inflammation of AF. Additionally, PTX3 could be superior to other inflammatory markers that were reported to be elevated in AF 86.
Ghrelin is secreted from the stomach and played role in appetite stimulation which is directly control by the hypothalamus by the activation of GH secretagogue receptor 1a as GHSR-1a. It is a neuroendocrine hormone and has the protective function of vasculature by antagonizing the effects of vasoconstrictors, for instance, endothelin-1, and promoting the effects of vasodilators, including nitric oxide (NO). with the help of hypothalamic AMP-activation protein kinase stimulation, it plays role in lipolysis. In contrast, many studies have shown there were two protective pathways (vasoprotective and lipolytic properties) of ghrelin that played role in protection against metabolic syndrome 87-89.
Moreover, Low levels of ghrelin are linked to the severity of the metabolic syndrome and associated with the different components of metabolic syndrome such as hypertension, insulin resistance, and obesity. When the number of metabolic syndromes derangements is increasing the levels of ghrelin also decrease 90-95.
Additionally, there are the following conditions that have explained the link between AF and ghrelin such as atrial fibrosis due to atrial structural remodeling which resulted in repolarization by interfering with atrial excitement as well as pulse transfer, and differences in atrial conduction. All events are occurred due to the presence and persistence of AF. Atrial myocytes apoptosis was closely associated with atrial fibrillation 96.
However, studies have further reported that a decreased ghrelin level could cause changes in atrial ion channels which in turn could elevate the likelihood of repolarization and promote the onset of atrial fibrillation. Also, Dixit et al study has reported that inflammation has played a significant role in hypoxic, myocardial fibrosis, and ischemic conditions which triggered the AF that might additionally exaggerate inflammatory responses. So, ghrelin has strong anti-inflammatory effects and could inhibit the expression of interleukin- 6, TNF- α and interleukin-1β 97.
Therefore, ghrelin could be considered to be a possible anti-inflammatory compound. Sharma et al study also revealed that oxidative stress also played a role in the process of atrial fibrillation. So, ghrelin can inhibit oxidative stress 98. In the same way, Ma et al study has shown that serum ghrelin concentration in patients with atrial fibrillation was reduced and significantly increased after treatment. Also, there was a positive association between the LVEF and serum ghrelin level in the patients of the atrial fibrillation group 99.
Uric acid is a heterocyclic organic compound with a molecular weight of 168 Dalton. C5H4N4O3 is the basic formula of uric acid. Metabolic breakdown of purine nucleotide gives uric acid which is the normal part of urine is excreted from kidneys and less amount is excreted from faeces. Furthermore, the most important organ of the body is the liver which produces uric acid. It can be produced from cells, tissues, and organs. The uric acid level is diverse and dominantly generated from endogenous purines and rests from the exogenous 100,101. Moreover, Oxidative damage has occurred in the ischemic liver, diabetes, atherosclerosis, and chronic heart failure due to uric acid which is a circulating marker of it 102. High levels of uric acid are an eminent risk factor for stroke, hypertension, dyslipidemia, and myocardial infarction. A positive association was found between uric acid and hypertension, BMI, triglycerides, and a negative association was found with HDL-C 103. Also, a Greek patient first showed Atrial fibrillation associated with serum uric acid in the case-control study 104.
In addition, a high level of serum uric acid has a role in left atrial and left ventricular remodeling and finally in the development of atrial fibrillation. CRP, IL—6, and TNF are related to AF and left atrial enlargement. At the same time, they were associated with higher uric acid levels. Hyperuricemia and gout exert pro-oxidant effects and decrease nitric oxide bioavailability in the vessel wall, endothelial dysfunction, and inducing inflammation. All these effects promote the conduction changes directly and increase the incidence of cardiovascular risk factors for AF such as metabolic syndrome, diabetes mellitus, and hypertension. The linking pathophysiological issues between AF and serum uric acid were inflammation and tissue remodeling 105.
Further, Increased levels of uric acid are related to permanent AF. Moreover, elevated levels of uric acid could be related to the burden of AF. Undoubtedly, more research will require to examine this potential association 104. Similarly, Liu et al. study had demonstrated an independent link between AF and increased serum uric acid in hypertensive subjects. Further studies require to examine potential association and underlying pathophysiological mechanisms 106.
In addition, Zhang et al. study had reported the increased risk of AF was linked to hyperuricemia 107. Similarly, Sun et al study revealed that in rural China, AF is positively linked to the SUA 108. In the same way, Chen et al. study had demonstrated that s significant relationship between increased prevalence of AF and elevated SUA concentrations in the Chinese population. The authors explained the gender-specific mechanism underlying the association between atrial fibrillation serum uric acids levels. There was no exact underlying mechanism that has explained the association between uric acid and AF 109. However, uric acid causes atrial remodeling by oxidative stress, endothelial dysfunction, inducing inflammation, RASS activation, which increases the risk of AF 110.
Similarly, Uric acid causes electrical remodeling which further shortens the atrial refractory period and establishes a reentry circuit in the atrium 111. Furthermore, Maharani et al study has reported that uric acid also causes structural remodeling and slows the velocity of conduction, thereby allowing reentry 110.
10.Oxidized Lipoprotein Lipase (OxLDL)
The product of lipid oxidation is the oxidized LDL as OxLDL and is also a marker of oxidative stress. The making of reactive oxygen species (ROS) is contributed by lipid oxidation and all the products form components of OxLDL. Lower concentrations of OxLDL, ROS and lipid oxidation products could be served as signaling components for pathways for cellular antioxidants. Cell damage and apoptosis were resulted due to the dysfunctional capacity of antioxidants in the cell and also seen in components of metabolic syndrome that contribute to the oxidation cascade 112.
Furthermore, Polovina et al. study (2017) has investigated the role of oxidative stress in the development of chronic kidney disease in AF. Further, the authors had concluded that AF had increased OxLDL as compared to sinus rhythm control 113. Also, Tousoulis et al. study concluded a strong association between endothelial function and inflammation in patients with AF. The only independent predictor of OxLDL is the maximum diameter of the left atrium. The authors had given the suggestion that predicts oxidative stress status might be the left atrium distension 114.
Additionally, Early afterdepolarization delayed afterdepolarization and intracellular Ca 2+ levels were regulated by an increase of L type Ca 2+ current and sarcoplasmic reticulum (SR) Ca 2+ load. They were caused due to ox-LPL in human AF. Another study also reported the pathogenicity of human AF caused by ox-LPL due to endothelial dysfunction, enhanced IcaL due to LPC – induced mitochondrial ROS production in cardiac myocytes that resulted to increase native Ca 2+ current (Ica) and vascular wall inflammation 115-117.






