Contact-Force Guided Pulmonary Vein Isolation does not Improve Success Rate in Persistent Atrial Fibrillation Patients and Severe Left Atrial Enlargement: A 12-month Follow-Up Study
Enes E. Gul1, Usama Boles1, Sohaib Haseeb1, Wilma Hopman1, Kevin A. Michael1, Chris Simpson1, Hoshiar Abdollah1, Adrian Baranchuk1, Damian Redfearn1, Benedict Glover1
1Heart Rhythm Service, Kingston General Hospital, Queen’s University, Kingston, Ontario, Canada.
Catheter ablation is a cornerstone treatment strategy in atrial fibrillation (AF). Left atrial (LA) size is one of the contributors in development of AF recurrences. The impact of contact-forced (CF) guided catheter ablation on the success rate of persistent AF patients with severe enlarged LA has not been investigated yet.
Sixty-six patients with diagnosis of longstanding persistent AF undergoing catheter ablation were enrolled. All patients underwent a standard transthoracic echocardiography according to the guidelines. LA size was considered severely enlarged when LA diameter was ≥ 50 mm. CF catheter ablation with a Tacticath Quartz catheter (St Jude Medical, St. Paul, MN, USA) was used in all patients.
The mean age was 61.9 ± 9.9 years, and LAD 47.8 ± 11.6 mm. Among 66 patients with persistent AF, 32 (48%) patients were diagnosed with AF recurrences. Twenty-eight (42%) patients had severely enlarged LA. The recurrence of AF was comparable in patients with and without severe enlarged LA (47% vs. 42%, p=0.79). The recurrence of AF was lower in patients who underwent CF-guided ablation with a normal LA dimension (36 %, p=0.54). Procedure duration was longer in patients with severely enlarged LA. LA dimension was not significantly different between patients with and without AF recurrence (49.8 ± 7.9 mm vs. 45.9 ± 7.5 mm, p=0.15). LAD and was significantly correlated with the time to recurrence of AF (r:-0.60, p=0.02).
Our preliminary findings have demonstrated that CF guided ablation does not improve the success rate in longstanding persistent AF patients with severe LA enlargement.
Key Words : Atrial Fibrillation, Catheter Ablation, Contact-Force, Enlarged LA.
Correspondence to: Enes Elvin Gul,
Division of Cardiology, Department of Medicine, Kingston General Hospital,
Queen's University, Kingston ON, Canada
76 Stuart Street, Kingston, Ontario, K7L 2V7
Atrial fibrillation (AF) is the most common cardiac arrhythmia encountered in clinical practice with an increased cardiovascular morbidity and mortality[1]. Studies have shown the superiority of catheter ablation compared to medical treatment in patients with refractory symptoms[2]. Despite technological advancements, the recurrence rate of catheter ablation is still high, ranging from 35 to 50%. Patients with persistent AF are more prone to recurrences due to electrical and structural remodeling[3].
Left atrial enlargement has been shown to be associated with an inversed rate of AF recurrence after chemical or electrical cardioversion[4]. Previous studies have shown that an increase in the LA diameter is associated with higher AF prevalence; moreover LA diameter is an independent risk factor in the development of AF, and in determining the long-term outcomes of ablation[5]. The interaction between LA size and AF has been confirmed in many studies, and both conditions mutually exacerbate each other. Therefore, it is important to know whether catheter ablation is useful in treating persistent AF patients with an enlarged LA size. Recently, AF ablation appears to be effective in non-paroxysmal AF patients with severe LA enlargement using non-CF guided catheter. The study also showed that AF ablation is associated with LA reverse remodeling and improvement in LVEF [6].
Contact-force (CF) catheters provide information to the operator to assess the proximity of the catheter to the endocardium. Low CF during pulmonary vein isolation (PVI) has been shown to be a predictor of acute and chronic PV reconnections, and is associated with an increased risk of AF recurrence[7-10]. CF has been shown to improve the durability of the PV isolation and empower the efficacy of catheter ablation [11]. The impact of standard CF parameters using CF guided catheter RF ablation in patients with severe enlarged LA has not been investigated.
Consecutive patients from May 2015 to April 2016 with persistent AF who underwent catheter ablation using the non-CF (Therapy Cool Flex, St Jude Medical, St. Paul, MN, USA) and CF sensing catheters (Tacticath Quartz, St Jude Medical, St. Paul, MN, USA) were enrolled. All patients underwent transthoracic echocardiography (TTE) and cardiac computed tomography (CT) prior to catheter ablation. Persistent AF was defined as an episode of AF lasting between 7 days and 12 months [12]. Patient demographics and medications at the time of the initial ablation were obtained from medical records. Exclusion criteria were defined as follows: patients <18 years of age, prior valvular surgery, severe mitral valve disease, paroxysmal and/or permanent AF, patients with thrombus within the left atrial appendage, and unwillingness to participate in the study. All patients included in the study provided written informed consent for participation in the study. Anti-arrhythmic medications (except amiodarone for a minimum of 4 weeks) were discontinued for five half-lives prior to the procedure. This study was approved by the ethics committee of Kingston General Hospital and Queen’s University’s Institutional Review Board in Ontario, Canada.
All patients underwent a transthoracic echocardiography (TTE) with a Vivid E95 machine (GE Healthcare, USA) according to ASE guidelines [13]. The LA size was measured in the short and long-axis parasternal view. LA size was considered enlarged when LAD ≥ 50 mm. Transesophageal echocardiography was performed to exclude any atrial thrombi 24 hours before ablation.
Periprocedural Anticoagulation
Patients who were receiving warfarin did not discontinue this prior to the procedure with a target INR of 2.0 and 3.0. Patients on non-vitamin K-antagonists withheld their anticoagulation for 48 hours prior to the procedure. After transeptal access was gained, intravenous unfractionated heparin was administered at 10 to 20 minute intervals to achieve a target-activated clotting time of 300-350 seconds.
Electrophysiology Study and Ablation
Patients were brought to the electrophysiology lab in a fasted state, and the procedure was conducted under conscious sedation with intravenous fentanyl and midazolam. Venous access was gained from the femoral veins. Standard intra-cardiac catheters were introduced through the right femoral vein: (1) A decapolar catheter (IBI Inquiry, St. Jude Medical, St. Paul, MN, USA) was positioned in the coronary sinus, (2) duodecapolar catheter (Supreme, St. Jude Medical, St. Paul, MN, USA) was positioned in the right atrium, (3) mapping and ablation catheter (Therapy Cool Flex, St. Jude Medical or TacticathTM Quartz, St. Jude Medical, St. Paul, MN, USA) delivered through a 9 Fr femoral sheath (St. Jude Medical, Minneapolis, MN) (4) A spiral multipolar PV catheter (AFocus II, St. Jude Medical, St. Paul) was placed through the long steerable sheath (Agilis, St. Jude Medical, Minneapolis, MN, and (5) quadripolar catheter (Supreme, St. Jude Medical, St. Paul, MN, USA) placed at the right ventricular (RV) apex. Intracardiac echocardiography (ICE) (ViewFlex XTRA, St.Jude Medical) was used to guide transseptal punctures in some cases. A 3-D reconstruction of the LA and pulmonary veins was created with the use of EnSite VelocityTM system (St. Jude Medical, St. Paul, USA)
AF ablation was performed with a wide area circumferential ablation (WACA) approach. The primary end point was considered as entry and exit block in all PVs. RF was delivered using a 4 mm externally irrigated-tip ablation catheter at a flow of 17-25 ml/min with a power range from 25 to 30 W. For each lesion, CF of at least 10 grams, and lesion duration of 40 seconds were reported as the minimal requirement. In sites with low CF such as LA/LAA ridge, force-time-integral (FTI) > 400 gs was aimed. PV isolation was considered complete when the circular PV potentials were no longer recorded. Acute reconnection was defined as LA-PV conduction spontaneously occurring during a waiting period of 20 minutes following the completion of the PV isolation, or when PV dormant conduction was evoked by an intravenous adenosine.
Post ablation, all patients received anticoagulation for at least 3 months and beyond this. Patients were evaluated by 24-h ECG Holter monitoring at 3 months, 6 months, and yearly thereafter. Recurrence was defined as an episode of any atrial arrhythmia lasting more than 30 seconds and occurring at least 3 months after ablation (post-blanking period) [12].
Data was collected in an Excel file and imported into IBM SPSS (Version 21 for Windows, Armonk, New York, 2015) for statistical analysis. Data were initially described using means, standard deviations and medians for continuous data, and frequencies and percentages for categorical data. Continuous data was also graphed to assess the underlying distribution. Associations between LAD and continuous data (time to AF recurrence) were assessed using Pearson correlations, with Spearman’s-rho correlation in the event of non-normal distributions. The comparison of 4 groups analyzed with a one-way ANOVA test, and time to event was assessed using a Kaplan-Meier curve. The association between the presence of enlarged LA and recurrence was assessed using independent samples t-tests, with the Mann-Whitney U test in the event of non-normal distributions. A p-value of less than 0.05 was considered statistically significant.
Sixty-six consecutive patients with persistent AF undergoing catheter ablation for AF were included in this study. Baseline demographics and procedure details are described in Table 1. Baseline LAD was 47.8 ± 11.6 mm, and LVEF was 54 ± 10 % (Table 1). During a follow-up of 12 months after a single ablation procedure, 34 patients (52 %) maintained sinus rhythm.
Analysis of the groups (group 1: non-CF and normal LA, group 2: non-CF and severe LA enlargement, group 3: CF and normal LA, and group 4: CF and severe LA enlargement) revealed that baseline demographic and echocardiographic parameters were comparable among the 4 groups. Patients who underwent CF-guided ablation with a normal LA dimension had lower recurrence rate (36 %, p=0.54). There was no significant difference in the other groups. Procedure duration and fluoroscopy time were shorter in patients who underwent CF-guided versus non-CF-guided ablation [Table 1].
Table 1. Demographic and procedural data of patients with persistent AF.
|
Overall |
Group 1 |
Group 2 |
Group 3 |
Group 4 |
P-Value |
|
n=66 |
n=16 |
n=16 |
n=22 |
n=12 |
| Age, years |
63.5 ± 9.5 |
63.4 ± 10.2 |
67.1 ± 7.5 |
63.8 ± 11.2 |
58.3 ± 5.8 |
0.12 |
| Gender, male |
46 |
8 |
10 |
17 |
11 |
0.08 |
| BMI, kg/m2 |
31.6 ± 5.8 |
31.6 ± 6.4 |
30.4 ± 5.6 |
31.3 ± 5.4 |
34.0 ± 6.0 |
0.42 |
| DM, n (%) |
14 (21) |
3 (19) |
4 (25) |
4 (18) |
3 (25) |
0.90 |
| HTN, n (%) |
46 (70) |
13 (81) |
9 (56) |
15 (68) |
9 (75) |
0.35 |
| CAD, n |
5 |
1 |
0 * |
1 |
3 * |
0.04 |
| CVA-TIA, n (%) |
10 (15) |
1 (6) |
3 (19) |
3 (14) |
3 (25) |
0.71 |
| SA, n (%) |
19 (29) |
4 (25) |
3 (19) |
9 (41) |
3 (25) |
0.35 |
| CHA2DS2VasC |
2.1 ± 1.4 |
2.0 ± 1.5 |
2.2 ± 1.4 |
2.3 ± 1.3 |
1.7 ± 1.3 |
0.71 |
| AAD, n (%) |
31 (47) |
6 (38) |
6 (38) |
13 (59) |
6 (50) |
0.44 |
| EF, % |
54 ± 10 |
57 ± 6 |
59 ± 9 |
56 ± 12 |
47 ± 8 |
0.07 |
| PT, min |
288 ± 69 |
309 ± 55 |
300 ± 59 |
265 ± 75 |
291 ± 82 |
0.24 |
| FT, min |
24 ± 10 |
26 ± 10 |
31 ± 15 * |
19 ± 14 * |
22 ± 8 |
0.02 |
| Recurrence, n (%) |
32 (48) |
9 (56) |
8 (50) |
8 (36) |
7 (58) |
0.54 |
* p value < 0.05 Group 1: non-CF and normal LA Group 2: non-CF and severe LA enlargement Group 3: CF and normal LA Group 4: CF and severe LA enlargement BMI, body mass index; DM, diabetes mellitus; HTN, hypertension; CAD, coronary artery disease; CVA-TIA, cerebrovascular accident-transient ischemic attack; SA; sleep apnea; AAD, anti-arrhythmic drug; EF, ejection fraction; LAD, left atrial diameter; PT, procedure time; FT, fluoroscopy time.
As shown in [Table 2], age, the presence of comorbidities, LVEF, and procedure details were comparable in patients with AF recurrence and severely enlarged LA to those without recurrence. Table 3 shows comparison of patients with and without AF recurrence and normal LA size. AF recurrences were more common in patients who had longer procedure duration (305 ± 75 min vs. 267 ± 63 min, p=0.09) and in females (10 vs. 3, p=0.006) [Table 3].
Table 2. Comparison of patients with severe LA enlargement in terms of recurrence of AF.
|
Recurrence |
Non-Recurrence |
P-value |
|
n=15 |
n=13 |
|
| Age, years |
64.5 ± 7.4 |
62.0 ± 8.8 |
0.44 |
| Gender, male |
12 |
9 |
0.67 |
| BMI, kg/m2 |
31.0 ± 5.4 |
33.0 ± 6.6 |
0.39 |
| DM, n (%) |
4 (27) |
3 (23) |
0.84 |
| HTN, n (%) |
10 (67) |
8 (62) |
0.96 |
| CAD, n |
2 (13) |
1 (8) |
0.64 |
| CVA-TIA, n (%) |
4 (27) |
1 (8) |
0.33 |
| SA, n (%) |
2 (13) |
4 (31) |
0.36 |
| CHA2DS2VasC |
2.4 ± 1.1 |
1.6 ± 1.4 |
0.15 |
| AAD, n (%) |
4 (27) |
8 (62) |
0.09 |
| EF, % |
49 ± 9 |
54 ± 11 |
0.41 |
| LA, mm |
54.0 ± 6.3 |
52.4 ± 6.0 |
0.49 |
| PT, min |
291 ± 84 |
301 ± 53 |
0.72 |
| FT, min |
28 ± 12 |
25 ± 13 |
0.60 |
| CF, n (%) |
7 (47) |
5 (38) |
0.72 |
BMI, body mass index; DM, diabetes mellitus; HTN, hypertension; CAD, coronary artery disease; CVA-TIA, cerebrovascular accident-transient ischemic attack; SA; sleep apnea; AAD, anti-arrhythmic drug; EF, ejection fraction; LAD, left atrial diameter; PT, procedure time; FT, fluoroscopy time; CF, contact-force.
Table 3. Comparison of patients with non-severe LA size in terms of recurrence of AF.
|
Recurrence |
Non-Recurrence |
P-value |
|
n=17 |
n=21 |
|
| Age, years |
64.4 ± 10.7 |
63.0 ± 10.7 |
0.69 |
| Gender, male |
7 |
18 |
0.006 |
| BMI, kg/m2 |
32.2 ± 6.2 |
30.7 ± 5.3 |
0.42 |
| DM, n (%) |
2 (12) |
5 (24) |
0.41 |
| HTN, n (%) |
14 (82) |
14 (67) |
0.69 |
| CAD, n |
1 (6) |
1 (5) |
0.93 |
| CVA-TIA, n (%) |
2 (12) |
2 (10) |
0.91 |
| OSA, n (%) |
4 (23) |
9 (43) |
0.09 |
| CHA2DS2VasC |
2.3 ± 1.5 |
2.0 ± 1.2 |
0.62 |
| AAD, n (%) |
8 (47) |
11 (52) |
0.74 |
| EF, % |
44.5 ± 3.6 |
42.7 ± 4.0 |
0.17 |
| LA, mm |
54.0 ± 6.3 |
52.4 ± 6.0 |
0.49 |
| PT, min |
305 ± 75 |
267 ± 63 |
0.09 |
| FT, min |
22 ± 8 |
22 ± 7 |
0.99 |
| CF, n (%) |
8 (47) |
14 (66) |
0.32 |
BMI, body mass index; DM, diabetes mellitus; HTN, hypertension; CAD, coronary artery disease; CVA-TIA, cerebrovascular accident-transient ischemic attack; SA; sleep apnea; AAD, anti-arrhythmic drug; EF, ejection fraction; LAD, left atrial diameter; PT, procedure time; FT, fluoroscopy time; CF, contact-force.
Acute procedural success was achieved in all patients. All patients were in sinus rhythm at the end of the procedure. AF terminated to SR or organized atrial tachycardia in 40 patients. SR was achieved by electrical cardioversion in the remaining 26 patients.
During a follow-up of 12 months after a single ablation procedure, there were 32 patients (48 %) with AF recurrences. Of those 32 patients, 12 patients underwent another catheter ablation, 8 patients required electrical cardioversion, and the remaining 12 patients were treated with antiarrhythmic treatment. The Kaplan-Meier curve [Figure 1]showed highly significant differences between the four groups in time to recurrence (Log Rank test = 29.9, p<0.001).
Figure 1. Kaplan-Meier Curve comparing Arrhythmia Free Survival between Groups
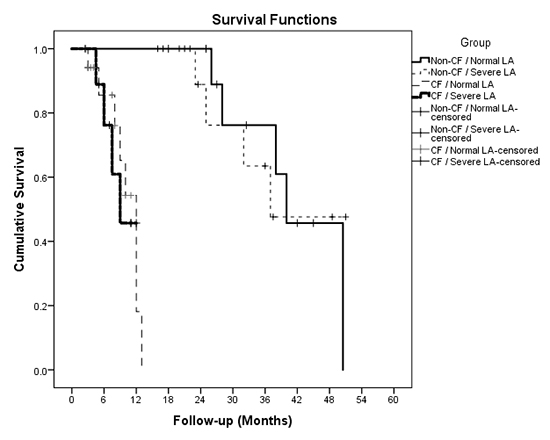
Log rank test = 29.9, p<0.001
This is the first clinical study where the impact of CF guided catheter ablation was studied in patients with persistent AF and severe LA enlargement. Our findings have demonstrated that CF guided ablation may have a significant impact on the success rate in persistent AF patients with severely enlarged LA but is associated with a lower rate of recurrence in patients with a normal LA size. Procedure duration and fluoroscopy time were shorter in patients with CF-guided ablation compared to those with non-CF catheter ablation.
The interaction between LA size and AF has been confirmed in many studies. Sustained AF results in electrical, contractile, and structural remodeling particularly in patients with persistent AF [14,15]. LA size was found to be a strong predictor of AF recurrences after successful catheter ablation [16]. Maintenance of sinus rhythm (catheter ablation or electrical cardioversion) has been shown to be worse in patients with an enlarged LA [17]. Electrical isolation of the pulmonary veins appears to be an effective treatment for paroxysmal AF [18]. Despite progress in catheter ablation technology, the recurrence rate of catheter ablation is still high and remains around 30-35 % within a year for paroxysmal AF [12]. In patients with the longstanding persistent AF success rate has been shown to be between 52-74 % after 12 months of follow up[16,19,20]. However, the patients included in these studies had a normal LA size. Our results demonstrated a 12 months’ success rate of 52 % in persistent AF patients. AF ablation in patients with enlarged LA is highly ineffective and related to a higher rate of failure to keep the patient in SR [21,22].
Catheter ablation in patents with severe LA enlargement has traditionally been challenging. Previous authors have investigated the role of catheter ablation in non-paroxysmal AF patients with severe LA enlargement, and found that radiofrequency ablation of AF is effective, and is associated with LA reverse remodeling and improvements in LVEF [6].
Patients with a larger LA required more ablation and longer durations of ablation in order to complete the ablation. Several techniques and approaches, including using a steerable sheath and better contact force were proposed to improve the outcome in patients with a severely enlarged LA. Very recently, Masuda and coworkers demonstrated the beneficial effects of using steerable sheaths in patients with severe LA enlargement with better outcomes (recurrence rate of 39 %) [23]. The steerable sheath facilitates increased catheter stability and more manipulation, and consequently more adequate lesion formation because of higher catheter-tissue contact. CF technology allows a real-time assessment of the catheter-tissue CF. Low CF during PV isolation is a predictor of acute and chronic PV reconnections, and is associated with an increased risk of AF recurrence [7-10]. In addition, ablation procedures under CF guidance improve the lower recurrence rate of the PV isolation [11]. The clinical outcome of using CF guided catheters in severely enlarged patients has not been investigated very well. In this current study, the recurrence rate of patients with severely LA enlargement undergoing catheter ablation with CF was similar to those without CF (58 % vs. 50 %). Recently, Masuda et al. found that reduced CF in patients with an enlarged LA, and this might explain why a large LA volume was associated with frequent AF recurrences after PV isolation [24]. Schluerman et al. recently studied 25 AF patients undergoing PV isolation with a steerable Agilis sheath, finding that the LA volume did not correlate with the CF [25]. One may question the lower success rate of catheter ablation in persistent AF patients with severely enlarged LA despite technological and procedural developments. This might be explained by evidence of non-PV triggers in patients with persistent AF [26]. In our study cohort, pulmonary veins were targeted in all patients. Several studies have showed that approximately 30% of AF triggers in persistent AF were found to be non-pulmonary venous (non-PV). The most common sites are the superior vena cava, ligament of Marshall, the coronary sinus, crista terminalis, left atrial posterior wall, and the left atrial appendage [27]. Our study did not investigate non-PV triggers.
The main limitation of our study is the small sample size. Therefore, we do not emphasize that CF sensed ablation is not effective in severely enlarged LA patients. In this study, we are trying to show that our small sample size did not show any signifcant results, however randomized studies with a larger cohort are needed to validate our findings. LAD may not always accurately reflect LA size because atrial dilatation can be eccentric. Therefore, it would be reasonable to measure left atrial volume and volume index in these patients. We performed 24-h ECG Holter at 3-months, 6 months and 12-months, however the recurrence rate could be underestimated because shorter rhythm monitoring particularly in asymptomatic patients. In addition, we did not assess the difference in terms of durability of PV isolation in the second session, however it is worthwhile to design new follow-up study in order to see this difference.
Although CF guided ablation is a safe approach in persistent AF patients with severe LA enlargement, it does not improve the success rate of catheter ablation. Optimum contact force parameters in persistent AF may not represent the main surrogate for successful outcome.
Conflict of interest and disclosure of funding
All authors declare that, the manuscript, as submitted or its essence in another version is not under consideration for publication elsewhere, and it will not be submitted elsewhere until a final decision is made by the editors of Journal of Arrhythmia. The authors have no commercial associations or sources of support that might pose a conflict of interest. All authors have made substantive contributions to the study, and all authors endorse the data and conclusions. Nevertheless, confirmation of informed patient consent for publication was obtained.






