“Clinical Impact of the Cryoballoon Temperature and Occlusion Status on the Success of Pulmonary Vein Isolation”
Takuro Nishimura1, Kaoru Okishige1, Yasuteru Yamauchi1, Hideshi Aoyagi1, Naruhiko Ito1, Yusuke Tsuchiya1, Takatoshi Shigeta1, Rena Nakamura1, Mitsutoshi Asano1, Mitsumi Yamashita1, Tomofumi Nakamura1, Hidetoshi Suzuki1, Tsukasa Shimura1, Manabu Kurabayashi1, Takehiko Keida2, Tetsuo Sasano1, Kenzo Hirao3
1Heart Center, Japan Red Cross Yokohama City Bay Hospital, Yokohama
.2Cardiology, Edogawa Hospital, Tokyo.3 Heart Rhythm Center, Tokyo Medical and Dental University, Tokyo.
Complete occlusion of the pulmonary veins (PVs) with the cryoballoon (CB) is considered to be the crucial factor for a successful PV isolation (PVI). We investigated whether a complete occlusion was indispensable for a successful CB based PVI of every PV.
Atrial fibrillation patients (n=123, 97; paroxysmal) undergoing a de novo PVI were enrolled. A total of 477 PVs were analyzed. The occlusion grade (OG) was scored as follows: OG3 (complete occlusion), OG2 (incomplete occlusion with slight leakage), OG1 (poor occlusion with massive leakage). There was no significant difference in the CB temperature (CBT) at all measured time points (from 30 to 120sec after freezing) and nadir CBT between OG2 and OG3 in all PVs except for the right inferior PV (RIPV). The RIPV isolation success rate was significantly lower for the OG2 status than OG3 (97.5 vs. 57.6%; p<0.0001). In contrast, there was not significant difference in the isolation success rate of the other three PVs between OG2 and OG3. In particular, the success rate of the right superior PV (RSPV) isolation was >95% for both OG2 and OG3. Phrenic nerve paralysis (PNP) was provoked during the RSPV isolation in two patients in whom the RSPVs were frozen during OG3
An OG3 may not always be required for a successful PVI of all PVs except the RIPV. OG2 could have comparable effects as OG3 in terms of a successful RSPV isolation. Not aiming for OG3 for the RSPV may reduce the risk of PNP.
Key Words : Pulmonary Vein Isolation, Cryoballoon, Occlusion Grade, Phrenic Nerve Paralysis.
Correspondence to: : Kaoru Okishige,
Heart Center, Japan Red Cross Yokohama City Bay Hospital 3-12-1 Shinyamashita Naka-ward Yokohama Kanagawa 231-0801, Japan
Pulmonary vein (PV) isolation (PVI) with a cryoballoon (CB) is widely utilized for treating atrial fibrillation (AF)[1]. When performing a CB based PVI, a complete occlusion of the PV ostia with the inflated CB is considered to be an indispensable factor for creating a continuous circumferential lesion with a high long-term durability for a successful PVI.
PVs often cannot be completely occluded by the CB because of the anatomical shape of the left atrium and PV ostia[2]. In order to obtain a complete occlusion of PVs, we sometimes push the CB deep into the PV ostia or apply the CB slightly inside of the PVs, which may result in increasing the incidence of phrenic nerve (PN) paralysis (PNP). On the other hand, we sometimes can obtain a lower nadir CB temperature (CBT) than we expected and an acute successful PVI in spite of leakage between the balloon surface and atrial tissue, which is an incomplete occlusion. The occlusion grade (OG) is classified according to the amount of leakage of contrast medium through the gap between the CB and PV ostium[3].
One parameter that suggests a good occlusion status is the CBT. A lower CBT indicates a better occlusion, because blood leakage hinders a sufficient temperature drop required for a successful PVI. The time to accomplish a successful PVI and the time for the CBT to reach 10°C have been reported as parameters affected by the OG4. The electrical reconnection rate of the PVs has been reported to be correlated with the completeness of the PV occlusion in the index procedure[4-7]. In all the literature investigating the relationship between the success rate of the PVI and the OG, all four PVs have been analyzed as a whole.
The aim of the present study was to evaluate the occlusion status for each of the 4 PVs separately in terms of examining their relationship to the CBT and PVI success rate. We also investigated whether a complete occlusion of the PV ostium by the CB was indispensable for achieving a complete PVI.
From March 2016 to August 2016, consecutive patients who underwent catheter ablation to treat AF with a CB at our institution were enrolled. Patients were excluded if they had thrombi in the LA, uncontrolled thyroid dysfunction, contraindications for anticoagulation, or an LA anteroposterior diameter of >55 mm. A contrast enhanced cardiac computed tomographic scan was performed before the catheter ablation to assess the LA anatomy and to rule out any intra-cardiac thrombi in all patients. Transesophageal echocardiography was performed in all persistent AF patients to rule out any intra-cardiac thrombi, especially in the left atrial appendage. Anti-arrhythmic drugs were discontinued for longer than 3 half-lives (amiodarone was discontinued for >1 month) prior to the ablation, and all patients were anticoagulated for >1 month.
The study and data collection were performed in accordance with protocols that had been approved by the Human Research Ethical Committee at our institutions.
Each patient provided written informed consent prior to the ablation procedure. Patients received conscious sedation with dexmedetomidine hydrochloride, which was administered from the beginning of the procedure. The luminal esophageal temperature was measured with a thermocouple catheter inserted through a nostril into the esophagus (Esophaster, Japan-Life-Line, Tokyo or S-CATH, CIRCA, Boston Scientific, Englewood, CO) prior to the ablation procedure to avoid any esophageal thermal injury associated with the cryoenergy application. A single trans-septal puncture was performed with an RF needle (Baylis Medical, Inc, Montreal, QC) under fluoroscopic and intracardiac echocardiographic (AcuNav, Biosense Webster, Diamond Bar, CA) guidance. Thereafter, heparin was administered intravenously to maintain an activated clotting time between 300 and 350 sec during the entire ablation procedure. The arterial pressure was continuously measured directly through the sheath inserted into the femoral artery during the ablation procedure.
The CB Catheter (Arctic Front Advance, Medtronic, Minneapolis) was introduced into the LA through a steerable long guiding sheath (FlexCath Advance, Medtronic, Minneapolis). A 28-mm CB was used in all cases. A mapping catheter (Achieve, Medtronic, Minneapolis) was advanced through the central lumen of the CB toward the PV orifice and introduced into the distal portion of each PV. Then the CB was inflated and advanced to the ostium of each PV in an attempt to obtain a complete occlusion. The OG was assessed according to the grade of retention of the contrast medium injected into the PV through the central lumen of the CB. When we achieved the best OG, cryothermal energy was applied for 180 or 240 sec. A duration of 180 sec was employed in cases when the PVI was successfully accomplished within 60 sec after the start of the freezing or if the balloon temperature reached -40°C within 60 sec as shown in a past report[4]. An acute PV isolation was defined as the complete elimination of the PV potentials recorded by the Achieve catheter during the CB application. If the PV potentials could not be recorded prior to freezing, we manipulated the Achieve catheter so as to locate it at an appropriate position that enabled the recording of the PV potentials. When a successful PVI was not achieved with a single application of the CB, further CB applications (maximum of three times) or irrigated radiofrequency energy (RF) ablation was undertaken as a touch-up ablation.
An electrode catheter was advanced into the superior vena cava for right-sided phrenic nerve (PN) stimulation during the CB ablation for the right-sided PVs. The compound motor action potentials (CMAP) of the diaphragm provoked by PN pacing were continuously monitored during the CB ablation applications for each PV as previously reported[8]. The freezing energy delivery was immediately terminated if the maximum voltage of the CMAP decreased by 30% compared to that before the freezing or weakening of the diaphragmatic excursion was observed.
Occlusion Grade (OG) Evaluation
The degree of the CB occlusion obtained by an injection of 50% diluted contrast medium into the PV was evaluated as: OG3 = complete occlusion (full retention of contrast medium with no visible leakage), OG2 = incomplete occlusion with slight leakage (the shape of the PV could be discerned by the contrast medium), and OG1 = poor occlusion with massive leakage (the shape of the PV could not be confirmed due to immediate flushing of contrast from the PV).
The OG for each PV was evaluated just before the freezing by two fully experienced doctors. The fluoroscopic image analysis used for the OG evaluation was performed at 15 frames/sec and with a normal detailed resolution in the antero-posterior and left anterior oblique projections.
In the case of a massive leakage of contrast medium through the inferior aspect between the CB and PV, a “pull-down” maneuver was utilized to improve the OG[9,10]. In those cases, the OG after the pull-down was adopted for the analysis. The method of the “pull-down” maneuver and evaluation of the OG after that maneuver were as follows: first, we tried to advance the CB on the superior aspect of the PV and started freezing with a massive leakage at the inferior aspect of the PV. Immediately after starting the freezing, we continuously and very slowly injected contrast medium through the central lumen of the CB to prevent blood frozen in that lumen. The CB and FlexCath were pulled down in order to close the inferior gap when the CBT reached -10 °C. The OG can be evaluated by investigating the contrast medium leakage after the “pull-down” maneuver (our experience revealed that the ice cannot be formed in the central lumen until the CBT reaches approximately -10 °C).
When multiple CB applications were performed for a successful PVI, the OG for only the first freezing was analyzed to exclude any cumulative effects provoked by subsequent freezings. The OG of the second and succeeding freezings were not included in the investigation.
Cryoballoon Temperature and Time Parameters
For each PV, the CBT was recorded at 30, 40, 50, 60, 90, and 120 sec from the onset of the freezing. The nadir CBT (NCT) was also noted. Moreover, the time to reach -40 °C of the CBT, time to obtain the PVI, and balloon thawing time (BTT, time for the balloon to return to 20 °C) were also recorded.
Diagnosis of Phrenic Nerve Paralysis
A diagnosis of PNP was made if (1) paralysis of the hemidiaphragm was noted on fluoroscopy during the ablation procedure despite the high-output pacing of the PN, (2) paradoxical movement of the diaphragm during spontaneous respirations was recognized by the fluoroscopy image, and (3) an elevated position of the diaphragm was observed compared to the preoperative state with a chest X-ray on the day after the ablation procedure. Once a diagnosis was established, the patient was closely followed-up with a repeated chest X-ray every month. The normalization of the chest images was considered as a complete clinical recovery.
The patient follow-up was performed through visits in our outpatient department. The referring physician performed a 12-lead surface ECG as well as a 24-hour Holter ECG at 2, 4, 6, and 12 months after the ablation. Any documented episodes of any atrial tachyarrhythmias longer than 30 seconds were considered a recurrence. Patients who underwent a re-do session for the recurrence of any atrial tachyarrhythmias were evaluated. Anti-arrhythmic drugs were discontinued for longer than 3 half-lives (amiodarone was discontinued for >1 month) before the re-do session.
Continuous data are expressed as the mean ± SD for normally distributed variables. Error bars in all figures represent the SEM. Statistical comparisons were performed using a Student’s t-test, Mann–Whitney U-test, Fisher’s exact test, or χ2 test, as appropriate. The p-value presented is for a 2-tailed test. A p-value of <0.05 indicated statistical significance. Analyses were conducted using JMP software (version 12.2.0 Scientific Discovery. ™ From SAS).
One hundred twenty-three patients were enrolled. The number of paroxysmal and persistent AF patients was 97 (78.9%) and 26 (21.1%), respectively. The mean age was 65±12 years old and 107 (87.0%) patients were male. The baseline patient characteristics are shown in [Table 1]. In total, 477 PVs were analyzed. Acute success of the PVI was achieved in all patients. Five patients had a left common PV, which was isolated by multiple CB applications with massive leakage on the roof and carina side as reported previously[11]. We excluded those cases from the analysis of this study. In 5 cases, the best occlusion status in the right inferior PV (RIPV) was OG1 in spite of meticulous manipulation of the CB. Those RIPV isolations were performed only by radiofrequency ablation.
Table 1. Baseline patient characteristics and the ablation procedure.
| Patients (n) |
123 |
| Age (years) |
65±12 |
| Male gender |
107 (87.0%) |
| Body mass index (kg/m2) |
24±4 |
| Echocardiogram |
|
| Left ventricular ejection fraction (%) |
64±10 |
| Left atrial diameter (mm) |
42±7 |
| Comorbidities |
|
| Hypertension |
50 (40.7%) |
| Diabetes |
16 (13.0%) |
| Previous cerebral ischemia |
8 (6.5%) |
| Heart Failure |
10 (8.1%) |
| Age >75 years |
33 (26.8%) |
| CHADS2 score |
1.0±1.0 |
| CHADS2-VASc score |
1.9±1.5 |
| Atrial fibrillation |
|
| Paroxysmal AF |
97 (78.9%) |
| Persistent AF |
26 (21.1%) |
The OG and Acute PVI Success Rate
The acute PVI success rate by the initial CB freezing was the lowest for the RIPV (57.6%). The left superior PV (LSPV), right superior PV (RSPV), and left inferior PV (LIPV) were successfully isolated in 81.4%, 91.1%, and 76.3%, respectively. Although an OG3 was obtained in more than 50% of the LSPVs, RSPVs, and LIPVs, in contrast, an OG3 was achieved in only 33.9% of the RIPVs. Moreover, the mean OG was lowest for the RIPV (2.7, 2.5, 2.4, and 1.9 for the LSPV, RSPV, LIPV, and RIPV, respectively [p<0.0001]). Radiofrequency touch up ablation to complete the PVI was required most often for the RIPV (1.7%, 0%, 5.9%, and 20.3% for the LSPV, RSPV, LIPV, and RIPV, respectively [p< 0.0001]). The χ2 was 53.9 for the OG, p<0.0001, with a high count of OG1 in the RIPV contributing the most (20.3) to the χ2 value, then a low count of OG3 in the RIPV (11.9). The χ2 was 47.3 for a touch up necessity, p<0.0001, with a high count of a touch up necessity in the RIPV contributing the most (30.3) to the χ2 value[Table 2].
Table 2. Acute PVI success rate and OG during the initial CB application.
|
Acute PVI success rate |
OG (%) |
Mean OG |
|
Touch up cases (%) |
|
| LSPV (n=118) |
81.4% (96/118) |
3: 88 (74.6) |
2.7 |
p < 0.0001 |
2 (1.7) |
p < 0.0001 |
|
|
2: 21 (17.8) |
|
|
|
|
|
|
1: 9 (7.6) |
|
|
|
|
| RSPV (n=123) |
91.1% (112/123) |
3: 82 (66.7) |
2.5 |
|
0 (0) |
|
|
|
2: 25 (20.3) |
|
|
|
|
|
|
1: 16 (13.0) |
|
|
|
|
| LIPV (n=118) |
76.3% (90/118) |
3: 67 (56.8) |
2.4 |
|
7 (5.9) |
|
|
|
2: 27 (22.9) |
|
|
|
|
|
|
1: 24 (20.3) |
|
|
|
|
| RIPV (n=118) |
57.6% (68/118) |
3: 40 (33.9) |
1.9 |
|
24 (20.3) |
|
|
|
2: 33 (28.0) |
|
|
|
|
|
|
1: 45 (38.1) |
|
|
|
|
CB Temperature and the PVI Success Rate Between OG2 and OG3
We compared the various parameters between OG2 and OG3. The number of PVs frozen by OG1 was 9/118 (7.6%), 16/123 (13.0%), 24/118 (20.3%), and 45/118 (38.1%) for the LSPV, RSPV, LIPV, and RIPV, respectively [Table 2]. We did not analyze OG1 because the acute PVI success rate of the PVs frozen with OG1 was low for all PVs (LSPV: 44.4%, RSPV: 62.5%, LIPV: 33.3%, and RIPV: 24.4%, average for all PVs: 36.4%).
There was no significant difference in the CBT for the PVs at all time points measured between OG2 and OG3 except for the RIPV. In the RIPV, significant differences in the CBT were observed between OG2 and OG3 at all points after 30 sec [Figure 1].
Figure 1. Comparison of CBT between OG2 and OG3 along the time series
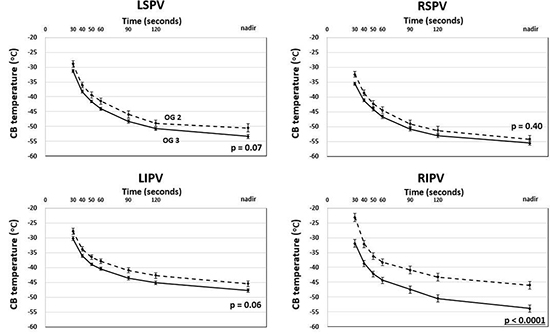
The broken lines and solid lines show the CBTs for OG2 and OG3, respectively, over time from the start of the freeze
The time to reach -40 °C of the CBT from the onset of the freezing (68±33 vs. 51±29 sec; p=0.034) and BTT (34±16 vs. 51±23 sec; p=0.0003) was significantly different only for the RIPV between OG2 and OG3 [Figure 2A,B].
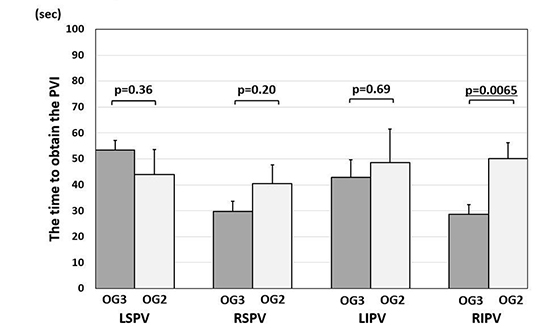
An average time to obtain a PVI of within 60 sec even with OG2 was observed in all 4 PVs. Significant differences in the time to obtain a PVI were also observed only for the RIPV between OG2 and OG3 (50±18 vs. 28±17 sec; p=0.0065) [Figure 2C].
Figure 2A Comparison of the time to reach -40°C of CBT between OG2 and OG3
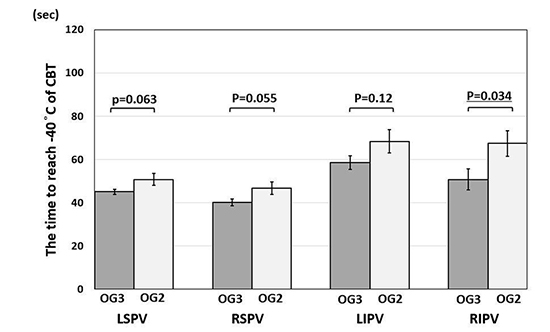
Figure 2B Comparison of the balloon thawing time between OG2 and OG3
Figure 2C Comparison of the time to obtain the PVI between OG2 and OG3
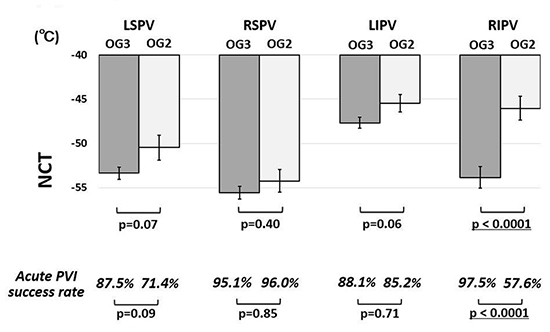
When comparing the NCT between OG2 and OG3, there was a significant difference in only the RIPV (-54±8 vs. -46±7 °C; p<0.0001). Regarding the other three PVs, the NCTs in OG3 tended to be lower than those in OG2, but there were no significant differences [Figure 3].
The PVI success rate with the initial CB freeze was significantly lower with OG2 than OG3 only for the RIPV (57.6 vs. 97.5%, respectively; p<0.0001). In the other three PVs, the PVI success rate for OG3 tended to be higher than that for OG2, but there were not significant differences. Particularly, the success rates of the RSPV isolation were very close between OG2 and OG3 (95.1 and 96.0 %, respectively) [Figure 3]
Figure 3 Nadir CB temperature and acute PVI success rate between OG2 and OG3
Transient right-sided PNP occurred in three cases (2.4%) during the right-sided PVI (RSPV: 2 patients, RIPV: 1 patient). All three PNP cases occurred during freezing during OG3. The paralyses that occurred during the RSPV freezing resolved after 1 day and 1 month, respectively. That which occurred during the RIPV freezing resolved within a day. A pseudo-aneurysm of the femoral artery occurred in one case (0.8%). No further complications or safety problems occurred.
Twenty (16.3%) patients received a re-do session, which was performed on average 10.5 months after the initial ablation session. The presence or absence of PV reconnections was investigated in 79 PVs of the 20 patients (in one case, the RIPV was isolated only by an RF catheter in the initial session and was excluded from the analysis). PV reconnections were observed in fifteen PVs (19%): LSPV 3/20 (15%), RSPV 1/20 (5%), LIPV 2/20 (10%), and RIPV 9/19 (47.4%).
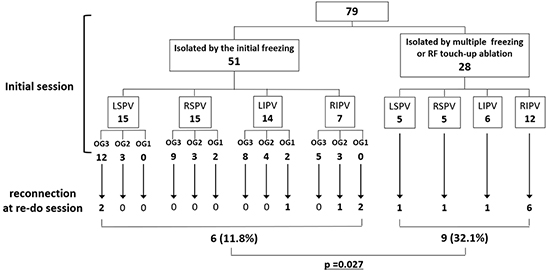
Fifty-one out of 79 (64.6%) PVs had been isolated by a single freezing application during the first session. Among those 51 PVs, 6 (7.6%) had reconnected by the time of the re-do session (two were LSPVs frozen with an OG3, one was an LIPV frozen with an OG1, and three were RIPVs frozen with an OG1 or OG2 in the initial session). The remaining 28 (35.4%) PVs were isolated by multiple freezings or RF touch-up ablation during the first session. OG3 was never obtained during any PVIs even with multiple freezings. Three RIPVs and 1 LIPV were finally isolated by a RF touch-up ablation. A reconnection was observed in 9 (1.1%) PVs (1 LSPV, 1 LIPV, 1 RSPV, and 6 RIPVs) during the re-do sessions. The PV reconnection rate of the two groups significantly differed (p=0.027) [Figure 4]
Figure 4 Summary of PVs that could be observed at the re-do session
There have been some papers on the OG of CBs. However, all four PVs were analyzed together in the previous reports. To the best of our knowledge, this is the first report of the relationship between the OG and PVI success rate, investigating each PV separately. The major findings obtained from the present study were: (1) the time course of the temperature drop did not differ between OG2 and OG3 for all PVs except the RIPV, (2) the time to reach -40°C, time to the PVI, BBT, and NCT were comparable between OG2 and OG3 for all PVs except the RIPV, (3) an OG3 was not deemed to be indispensable for all PVs except the RIPV in terms of an acute success of the PVI and long-term PVI maintenance, and (4) when the PVI of the RSPV was performed with an OG2, PNP was never provoked.
Many previous reports have stated that it is difficult to obtain a complete occlusion of the RIPV[2,6,12,13]. In a PVI based on the CB, we usually position the CB so that the CB can evenly adhere to the PV orifice. Fürnkranz et al. reported that when CB freezing is performed for the inferior PVs, a central alignment of the CB at the PV ostium is often not possible because the sheath/balloon system must be deflected in order to reach the target structure[14]. In particular, positioning the CB concentrically at the RIPV orifice is more difficult relative to the other PVs because the orifice of the RIPV is close to a portion of the atrial septal puncture.
Although the CBT was recorded 30 ~ 120 sec from the start of the freezing, the CBTs of the three PVs except for the RIPV from 30 seconds did not significantly differ between OG2 and OG3. It was suggested that the ice ball formation could have been accomplished within 30 sec, and eliminated the leak through the gap. Gaps between the PV orifice and CB may be filled with an ice ball formation on the CB surface even if there is a slight leakage of the blood. Gaps may also be sealed, because the CB diameter increases from 26.5 to 28 mm and the internal pressure of the CB also increases from 2.5 to 15 psi during inflation[15]. We believe that it was the reason why there was no significant difference in the PVI success rate between OG2 and OG3 for LSPV, LIPV and RSPV. We speculated that gaps may be too large to be filled by an ice ball formation or a further increase in the diameter of the CB after freezing in the case of the RIPV.
With the RSPV, an NCT between OG2 and OG3 was almost comparable with a p value of 0.4 and had also a similar acute PVI success rate. Sorgente et al.2 calculated the ovality index of the PV ostia (the ratio between the maximal and minimal ostium diameters) from contrast CT. They reported that there was a significant difference in the ovality index between the left- and right-sided PVs (p<0.001) (1.49±0.20 for the LSPV, 1.54±0.16 for the LIPV, 1.14±0.13 for the RSPV, and 1.16±0.13 for the RIPV, respectively). Because the ovality index of the RSPV was low, they speculated that if there was a gap between the RSPV and CB, it would have been relatively even around the CB.
It has been reported that a longer time to the PVI and failure to achieve -40 °C within 60 sec independently predicts a late PV reconnection[16]. In this study, when the RSPV was occluded with an OG2, the CBT reached -40 °C at an average of 47 sec, and a successful PVI was achieved within 60 sec. The BTT was also similar between OG3 and OG2 (p=0.86). Based on these results, we could expect that an RSPV frozen with an OG2 could have a long-term durability of the PVI equivalent to that of being frozen at an OG34. In fact, 20 patients in whom we performed a re-do ablation, it demonstrated that the PV reconnection rate was low even in PVs that were successfully isolated with a single freezing with an OG2. In other words, the same long-term durability was obtained between the OG2 and OG3. In contrast, the reconnection rate was high in the PVs isolated by multiple freezings, and most of them happened with RIPVs. Regarding the RIPV, a satisfactory long-term durability could not be obtained with the RIPVs despite multiple freezings and devised manipulation of the CB.
When ablating the RSPV with the CB, our results suggested that sufficient injurious effects of the CB could be obtained even with an OG2, and there was less need to manipulate the CB for the purpose of obtaining an OG3. It has been reported that pushing the CB aiming for a complete occlusion can lead to an extension of the anterior surface of the RSPV by 6.3 mm[17]. This RSPV distortion would shorten the distance between the PN and CB, which might result in PN injury. In this study, two of the patients suffering from PNP during the RSPV ablation had been frozen with an OG3. It may be expected that performing the CB ablation with an OG2 rather than an OG3 could reduce the incidence of right-sided PNP. Casado-Arroyo et al. reported the less vigorous wedging maneuver during RSPV freezing was useful to avoid the incidence of PNP15. They recommend the following. First, the inflated CB was positioned with a complete occlusion of the RSPV, then the CB was retrieved to a more proximal position until a small leak was observed. After that, the cryoenergy application was started and the “CB was advanced” aiming for a complete occlusion. The RSPV could be occluded at a more proximal position than the first occlusion because the balloon volume and internal pressure increased during the freezing status as compared to that during the inflated status. However, the final step “advancing the CB” might retain a risk of RSPV distortion and shortening the distance between the CB and PN. Saitoh et al. reported the risk of PNP could be evaluated by the spatial relationship between the CB and cardiac shadow on the fluoroscopic image during the RSPV freezing[18]. Martins et al. analyzed the measured distance between the vertical projection of the distal tip of the SVC catheter stimulating the PN to the distal segment of the CB in the AP view, and related it to the incidence of PNP1. If the risk of PNP is expected to be high before the cryoenergy application starts, aiming for a complete occlusion of the RSPV by pushing the CB might not be necessary.
Several limitations to this study should be acknowledged. 1) The OG is a subjective evaluation value. Although we proposed objective criteria for the OG from fluoroscopic imaging, there was the possibility that the interpretation could differ among physicians and medical facilities. 2) These data were an analysis dealing with only anatomically normal PVs and left common PVs, and extremely large PVs were not evaluated. 3) We evaluated the OG only with fluoroscopic imaging. A recent method for assessing the PV occlusion state is with echocardiography and CB pressure wave analyses[19-21]. If those devices had been used in the present study, we might have been able to observe how the PV orifice was occluded, for example, whether the OG2 was occluded by an ice ball formation or not. 4) We evaluated the durability of the PVI only in cases that suffered from AF recurrences. In the future, verification by a large-scale study is desired.
There were no significant differences in the CBT and acute PVI success rate between OG2 and OG3 for the LSPV, LIPV, and RSPV. OG3 should be obtained for a successful RIPV isolation. On the other hand, OG3 was not deemed to be indispensable for a successful PVI especially for the RSPV. An intentional complete occlusion by pushing the CB for the RSPV might not be necessary for preventing the incidence of PNP.






