Remote Monitoring of Atrial High Rate Episodes in Pacemaker Patients. The Rapid Study Design
Vincenzo Russo1, Anna Rago1, Vincenzo Tavoletta2, Valter Bianchi2, Cristina Carella3, Giuseppe Ammirati3, Aniello Viggiano3, Stefano De Vivo2, Antonio Rapacciuolo3, Gerardo Nigro1, Antonio D’Onofrio2
1Chair of Cardiology, University of Campania "Luigi Vanvitelli," Monaldi Hospital, Naples, Italy..2Departmental Unit of Electrophysiology, Evaluation and Treatment of Arrhythmias, Monaldi Hospital, Naples, Italy..3Department of Advanced Biomedical Sciences, University of Naples Federico II, Naples, Italy..
Remote Monitoring (RM) has been introduced for several years and nowadays most pacemakers are equipped with such a technology. RM can provide early detection of high atrial rate episodes (AHREs) onset and enable prompt medical intervention. However, there are still little data on the clinical reactions triggered by the AHRE detected by RM of pacemaker recipients and on their possible benefit on patients’ outcome.
The RAPID study is a multicenter, prospective, non-interventional study designed to compare the time from onset to first physician's evaluation of AHRE episode with arrhythmic burden ≥5% (72 minutes) for pacemaker recipients without atrial fibrillation history, between patients followed with RM or conventionally with annual in-hospital visits. A total of 98 patients with implanted dual-chamber pacemaker, assigned to RM-OFF or RM-ON according to ordinary clinical site practice, will be followed for a total of 18 months. After the implant, patients will perform their first in-hospital follow-up visit at 1 month and then, in the RM-OFF group, patients will perform an in-hospital FU every 6 months, while in the active group, patients will be continuously monitored via RM until study termination. All AHREs and consequent medical interventions will be collected over the entire study period.
The ongoing RAPID study will provide additional information on the role of RM in the management of AHRE detected in pacemaker patients without documented atrial fibrillation history in ordinary clinical practice.
Key Words : Remote Monitoring, Atrial Fibrillation, Pacemaker, Atrial High Rate Episode.
Correspondence to: Vincenzo Russo ,
Monaldi Hospital, Via Leonardo Bianchi, 1, 80131 Naples, Italy
Atrial fibrillation (AF) is the most common arrhythmia in the general population and is associated with an increased risk of stroke and mortality[1-2]. Undiagnosed AF is common as it is often asymptomatic and intermittent[3]. Considering the arrhythmic risk and its consequences, the early detection of AF is of pivotal importance for the optimization of the clinical follow-up and medical therapy. Modern cardiac implantable electronic devices (CIEDs) include detailed algorithms and functions for the accurate detection of atrial high rate episodes (AHREs)[4,5].
In addition, modern CIEDs are equipped with remote monitoring (RM) technology, which provides automatic transmissions of diagnostics and technical data from the implanted devices to the attending physician[6]. RM has been shown to be a safe alternative to the conventional in-hospital visits, especially for low-risk patients, such as pacemaker recipients[7-8]. Despite the latest HRS Expert Consensus Statement which has set a class I recommendation for RM as useful tool for the early detection and quantification of AF [9], there are still few data on the clinical reactions triggered by the AHRE detected by RM of CIEDs and on their possible benefit on patients’ outcome. Therefore the role of RM for early detection of significant AHRE is still to be explored and analyzed and is extremely fascinating for its clinical implication.
Study Design and Objective
The RAPID Study is a prospective, multicenter, non-randomized, non-interventional study ongoing in three Italian sites that will enroll 98 patients with dual-chamber pacemaker. The objective of this study is to evaluate the time from onset to first physician's evaluation of AHRE with arrhythmic burden ≥5% (72 minutes) in ordinary clinical practice for pacemaker patients without documented AF history and compare it between patients followed with RM or conventionally with annual in-hospital visits. The AHRE burden threshold that constitutes a mandate for anticoagulation is still debated, even if a recent analysis demonstrated that short episodes (<24 hours) had no significant effect on the risk of ischemic stroke[10].
Secondary objectives include: time to first investigator evaluation of AHRE episodes, regardless of its duration, time to anticoagulant therapy onset, time to any medical reaction related to the treatment of new onset atrial arrhythmia, time to cerebral ischemia, and time to first hospitalization due to cardiovascular issues
[Table 1].
Table 1. Study objectives and inclusion/exclusion criteria.
| Primary objective |
-Time from onset to first physician's evaluation of AHRE episode with arrhythmic burden ≥5% (72 minutes) in pacemaker patients followed with RM or conventionally with annual in-hospital visits. |
| Secondary objective |
-Time to first investigator evaluation of AHRE episodes, regardless of its duration; |
|
-Time to anticoagulant therapy onset; |
|
-Time to any medical reaction related to the treatment of new AF onset |
|
-Time to cerebral ischemia; |
|
-Time to first hospitalization due to cardiovascular issues. |
| Inclusion criteria |
-age > 18 years; |
|
-Indication to dual-chamber permanent cardiac pacing for sick sinus node dysfunction or atrio-ventricular block. |
| Exclusion criteria |
-Ongoing atrial arrhythmia at enrollment; |
|
-Prior symptomatic or documented AF episodes: |
|
-Pacemaker replacement or upgrading of previous devices with recorded episodes of AF; |
|
-Severe valvular disease or valvular prosthesis; |
|
-Pregnancy. |
AHRE = atrial high rate episode.
Investigational centers were selected on the pre-disclosed practice to provide or not pacemaker recipients with RM in order to balance the study arms. Approvals of the local Ethics Committees were obtained for all participating sites. The study started in December 2015 and is expected to last at least 5 years.
Inclusion/Exclusion Criteria
Patients will be enrolled consecutively after providing written consent and fulfilling all the inclusion/exclusion criteria listed in [Table 1]. Inclusion criteria include age > 18 years, and indication to dual-chamber permanent cardiac pacing for sick sinus node dysfunction or atrio-ventricular block according to the current guidelines[11].
Patients will be excluded in case of ongoing atrial arrhythmia at enrollment, prior symptomatic or documented atrial arrhythmia episodes, pacemaker replacement or upgrading of previous devices with recorded episodes of AHRE, severe valvular disease or valvular prosthesis, and pregnancy.
Implantation and Follow-up
Patients will be screened before undergoing PM implant and will perform an echocardiogram within 3 months prior to implant procedure; patients will participate after having signed the written informed consent before hospital discharge or, alternatively, within 90 days after PM implant, and will receive RM (RM-ON) or not (RM-OFF) according to site standard practice.
Patients in the RM-OFF group will be followed up at 1 month, 6 months (optional), 12 and 18 months with in-hospital visits, while patients in RM-ON group will be visited in-hospital at least at 1 and 18 months. Additionally, patients with RM will be followed remotely and unscheduled in-hospital visits may be triggered by RM alerts. The physician’s reaction time to remote notifications was not specified and patients were informed that the data would be evaluated only during office hours on weekdays, as ordinary clinical practice. [Figure 1] summarizes the study flow chart.
Figure 1. Study Flowchart
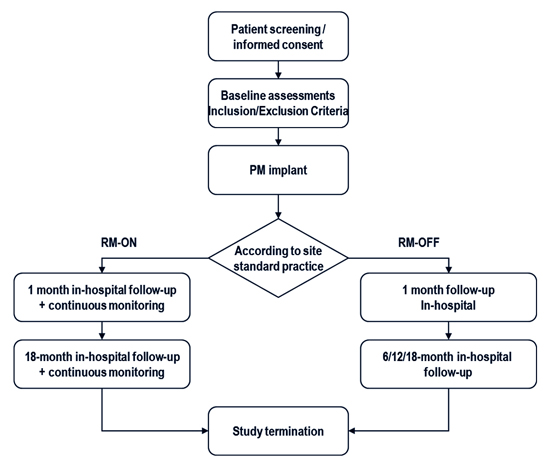
At every FU visit, all the device diagnostic data and AHRE recordings will be collected in electronic case report forms (eCRFs). In addition, any medical interventions triggered by AHRE episodes, as any adverse event, for both groups will be reported in specific forms. Regular study termination will be at the 18-month follow-up, while premature termination may be due to withdrawal of consent, explantation of device, lost to follow-up or death of patient.
AHRE recordings and study endpoints events will be adjudicated by an expert physician blinded to patient’s group.
Pacemaker AHRE detection is based on the high atrial rate criterion that will be programmed with a threshold rate of 190 beats/min. AHRE burden, defined as the total time spent in atrial arrhythmias in a single day, is automatically provided by the device, and intracardiac electrogram recordings (IEGM) are stored in the device memory for all AHRE episodes exceeding a duration of 30 seconds. Other settings will be left to the investigator’s discretion.
In the RM-ON group, patients will be provided with RM technology able of daily transmissions (Home Monitoring, Biotronik SE and Co, Germany). Implants, through wide range radiofrequency telemetry, send messages to a patient unit that forwards data to a central server using GSM networks. Physicians have access to this information on protected websites and automatic notifications are triggered by selectable events. The RM notifications for AHRE detection will be set as follows: AHRE burden>5% per 24 hours and long atrial arrhythmic episode>6 hours.
Statistical Consideration and Analysis plan
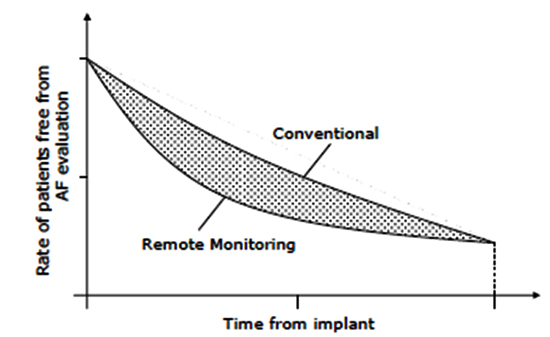
Standard descriptive analysis will be used for study results and the difference between the areas under the Kaplan-Meier curves will provide an estimate of the expected delay between the episode onset and physician's evaluation for the two groups [Figure 2].
Figure 2. Difference between the areas under the Kaplan-Meier curves will return an estimate of the expected delay between the episode onset and physician's evaluation for the two groups.
As the primary endpoint is the time to the first ≥5% in 24 hours (72 minutes) AHRE investigator evaluation, it is expected that its distribution will be skewed and approximately exponential. However, no assumptions have been made on the actual distribution of times, preferring a non-parametric approach (Wilcoxon-Mann –Whitney test). The null hypothesis is that the probability of obtaining a larger value from the RM-OFF group rather than from the RM-ON is 50%. In order to estimate the required sample size to obtain a target statistical power of 80% with an alpha error of 0.05, some assumptions on this probability under alternative hypothesis have been made. Such assumptions depend on the rate of symptomatic atrial arrhythmia episodes and the overall FU duration. Based on available literature[12], the cumulative proportion of patients with AF episode has been considered around 30% at 18 months in an unselected pacemaker cohort; 27% of them with mild or severe associated symptoms and 9% with severe symptoms. It has been assumed that the probability of extracting a longer delay in the RM-OFF group decreased on increasing the rate of symptoms. With these assumptions, the recruitment of 98 patients is needed to reach the required power; such a calculation includes a 10% loss rate.
CIEDs enable continuous monitoring of heart rhythm and have an excellent sensitivity and specificity for AF diagnosis[13]. This increased ability to detect AHREs and the recent evidences of association between such events and stroke risk pose new challenges to clinicians[4],[14].
Diagnostic data stored in device memory may become meaningful if they are promptly available to the physician, allowing early detection and possibly preventing severe adverse arrhythmia-related events. In the TRUST study (The Lumos-T Safety Reduces Routine Office Device Follow-up) AF detection was 34.5 days earlier with RM vs standard follow-up (5.5 vs 40 days)[15]. Recently, the SETAM (Strategy of Early Detection of Atrial Arrhythmias with Home Monitoring) study confirmed that remotely monitored patients were diagnosed earlier than for AF, and interestingly found also a reduction of 4 hours/day (18%) in the AF burden when RM was active[16].
Despite these promising results, the evidence of stroke risk reduction with the use of RM is still awaited. The recent IMPACT study (Combined Use of BIOTRONIK Home Monitoring and Predefined Anticoagulation to Reduce Stroke Risk), which randomized 2718 patients with dual-chamber and biventricular defibrillators to start and stop anticoagulation based on RM or conventional in-hospital follow-up (FU), failed to show the superiority of RM[16]. However, the median time from AF occurrence to anticoagulation onset was significantly shorter in the RM group than in the control group (3 days Vs. 54 days, p<0.001)[17].
An absence of temporal relationship between arrhythmic event and stroke onset has also been found, atrial arrhythmia may contribute to clot formation in the left atrium but that clot need not embolize during the arrhythmic episode; thus, the atrial arrhythmia may be a risk marker of more severe atrial disease/dysfunction/thrombogenesis potential and/or may be a direct cause. In addition, patients with device-detected AHREs appeared to be at lower risk for stroke compared to patients with overt AF. In patients with CHADS2 score >2, the annualized thromboembolic event rate associated with subclinical AHREs was 2.4% in TRENDS[14] and 2.1% in ASSERT[4], far below from the 4-4.5% annual rate expected in “clinical” AF patients with similar risk profile. As a result the net clinical benefit of anticoagulation may be reduced.
The identification of patients who may benefit from anticoagulation is challenging and combining AHRE burden with CHA2DS2-VASC score has been suggested as an appropriate approach to stratify stroke risk. Patients with low CHA2DS2-VASC may benefit from anticoagulation if a single AHRE episode exceeds 24 hours; while for patients with a score >2 the anticoagulation could be appropriate start for AHRE lasting > 6 minutes[18,19].
Of note, initiation of anticoagulation was commonly adopted in the recent trials using insertable cardiac monitors, providing a promising methodology for atrial arrhythmias screening in patients without indication to permanent cardiac pacing[20]-[22].
Several studies such as the ongoing ARTESiA (Apixaban for the Reduction of Thrombo-Embolism in Patients With Device-Detected Sub-Clinical Atrial Fibrillation) and NOAH-AFNET 6 (Non-vitamin K antagonist Oral anticoagulants in patients with Atrial High rate episodes) will help to elucidate the use of oral anticoagulation in patients with device-detected AHRE[23,24].
In this complicated scenario the role of RM for early detection of significant atrial arrhythmia is still to be explored and analyzed and it is extremely fascinating for its clinical implication since it may provide additional time to consider how to manage AHRE patients.
An accurate comparison of the delay of significant AHRE detection with standard in-hospital visit with respect to RM should be the first step towards a definite assessment of clinical impact of RM in stroke prevention.
In conclusion, the ongoing RAPID study will provide additional information on the role of RM in the management of AHRE detected in pacemaker patients without documented atrial arrhythmia history in ordinary clinical practice.






