Dr. Mondragon Ignacio*, Dr. Joaquín J. Jarma*, Vecchio Nicolas*, Daquarti Gustavo*, Tomas Leandro, Caro Milagros*, Elias Vasquez*, Giniger Alberto, Rivera Santiago*, Albina Gaston*, Scazzuso Fernando*
Pulmonary vein isolation (PVI) has become the standard treatment of symptomatic atrial fibrillation. Patients remain hospitalized for at least 24 hours to detect potential complications in most centers worldwide. There is still a lack of data about the safety of same-day discharge.
The aim was to compare the safety of same-day discharge with next day discharge after overnight monitoring.The rate of new hospitalization and visits to the emergency department and the costeffectiveness of the same-day discharge approach were evaluated.
We conducted a longitudinal and prospective cohort study of all the consecutive patients undergoing scheduled pulmonary vein ablation of either paroxysmal or persistent atrial fibrillation (AF). The complications were recorded by type and time of occurrence.
Overall 58 patients were discharged within the same day and 137 patients stayed overnight after PVI. There were no significant differences in demography, comorbidities and other predictors of complications. No complications were reported after the sixth hour. We observed a significant difference in the number of visits to emergency department: 15.5% for the same-day discharge group vs. 30.7% for the overnight hospitalization group (p 0.03). Only 50% of the reasons to visit the emergency department were cardiovascular causes. No cases of pericardial tamponade were reported and none of the patients required new hospitalization up to 30 days of follow up.
Same-day discharge after PVI is feasible and cost-effective. This is the first study analyzing the experience in patients undergoing AVP,considering acare based component to this procedure. This approach would provide significant benefits for patients and health care providers.
After many years of development, pulmonary vein isolation (PVI) has become the standard treatment of symptomatic atrial fibrillation refractory to drug therapy. However, the complications and the results associated with the procedure are a matter of concern for the treating physician at the moment of the decision-making process, as PVI is probably the most complex ablation procedure. Now a days, patients remain hospitalized for at least 24 hours to detect potential complications in most centers worldwide. According to our experience, most of these complications occur and are detected during the intervention, while only a minority occur a few hours later.
Same-day discharge after PVI could have advantages in terms of costs for the health system, the patient’s experience and the institution where the procedure is performed, improving the logistics and producing a more efficient use of resources. There is still a lack of data about the safety of same-day discharge compared to overnight hospitalization.
The aim of this study was to compare the safety of same day discharge with next day discharge after overnight monitoring.
In addition, the rate of new hospitalization and visits to the emergency department and the cost effectiveness of the same day discharge approach were evaluated.
We conducted a longitudinal and prospective cohort study of all the consecutive patients undergoing scheduled PVI between June 2015 and May 2016 at the Instituto Cardiovascular de Buenos Aires (ICBA). Patients with paroxysmal or persistent atrial fibrillation (AF), either refractory or intolerant to antiarrhythmic therapy, and those with recurrent AF undergoing a new pulmonary vein ablation were included.
The information was introduced in the database of the electrophysiology laboratory of the ICBA and was prospectively retrieved.
All the patients were admitted to the coronary care unit after the procedure and were monitored until the moment of discharge.
Procedures were performed by four different operators of the electrophysiology laboratory at Instituto Cardiovascular de Buenos Aires (ICBA).
Anticoagulation therapy was managed according to expert’s recommendations: new oral anticoagulants (NOACs) were stopped 24 hours before the procedure and for those taking inhibitors of clotting factors, and medication was adjusted to achieve an international normalized ratio (INR) between 2 and 2.5. Bridging with low molecular weight heparin was not used in any case. Anticoagulation therapy was continued 6 hours after the procedure.
Under general anesthesia, three venous accesses were performed with 6F, 7F and 8F sheaths, using the Seldinger technique. A decapolar catheter was introduced in the coronary sinus. Under fluoroscopy guidance, a transseptal puncture was performed with an SL1 St. Jude introducer and a Brockenbrough needle. Transesophageal or intracardiac echocardiography was available in all the cases and was used at the preference of the operator.
Radiofrequency ablation was performed using Therapy Cool Path irrigated-tip ablation 8 mm catheters (St. Jude) and a multipolar diagnostic catheter (Lasso, 24 poles). For cryoballoon ablation, a second-generation Arctic Front Advance cardiac catheter was used. During the procedure, heparin sodium was administered with a target activated clotting time (ACT) between 350 and 450 seconds. An esophageal temperature probe was used to monitor esophageal temperature and possible phrenic nerve injury was monitored by means of diaphragmatic phrenic nerve pacing.
The final target was the circumferential isolation of the pulmonary veins achieved by point-by-point radiofrequency catheter ablation at each segment of the pulmonary vein antrum. For cryoballoon ablation, circumferential isolation was demonstrated by pulmonary vein occlusion using contrast venography and adequate contact between the device and the pulmonary vein, achieving a temperature below -40ºC with a 1:1 ratio in temperature trough (-30°C in 30 seconds). For both techniques, the target was to achieve dissociated pulmonary vein activity and bidirectional conduction block across the line confirmed by means of differential pacing.
Follow up: All the patients were contacted by telephone calls one week after the procedure (in case they did not visit the emergency room within the first week) and underwent 24-hour Holter monitoring at 30 days as part of the standard practice after catheter ablation. In all the cases, the patients were discharged with antiarrhythmic drugs for three months or according to the preference of the attending physician.
The cost per one bed-day in the coronary care unit was obtained from our finance department. We estimated the potential savings for those patients discharged on the same day.
Continuous variables are presented as mean ± standard deviation and non-parametric variables as median (IQR), and compared using the Student's t test or the Mann-Whitney test, as applicable. Categorical variables are expressed as percentages and compared using the chi square test. A p value < 0.05 was considered statistically significant. The statistical calculation was analyzed using SPSS 22.0 statistical package (IBM, Chicago, IL).
In case the characteristics of the patients were not homogeneous a propensity score was used. The study was conducted following the recommendations of the Declaration of Helsinki. The Argentine personal data protection law 25,326 exists to guarantee individuals’ access to their medical records, revise them and correct them within intervals no shorter than six months, unless a legitimate interest to do otherwise is shown (14th article, section 3)
A total of 205 procedures were performed. Ten patients presented complications and remained hospitalized for more than 24 hours, thus, they were excluded from the final analysis.
The final cohort was made up of 195 cases. After the procedure, 58 patients were discharged within the same day and 137 patients stayed overnight after the procedure.
There were no significant differences in comorbidities and non-clinic predictors of comorbidities between both groups [Table 1]. Mean age, body mass index and echocardiographic characteristics were also similar.
Mean CHADS score was low in the population and similar between both groups. Four operators performed the procedure and there were no differences in the decision of using a same-day discharge strategy or an overnight hospitalization approach[Table 2].
Table 1. Characteristics of the population
| Characteristics of the population |
Same-day discharge(58) |
Overnight hospitalization (137) |
p |
| Men |
84.5% (49) |
75.2% (103) |
0.15 |
| Age |
57 (49-66) |
62 (52-66) |
0.42 |
| HT |
41.4% (24) |
43.1% (59) |
0.82 |
| Dyslipidemia |
22.4% (13) |
25.5% (35) |
0.64 |
| Coronary artery disease |
5.2% (3) |
9.5% (13) |
0.42 |
| Diabetes |
10.3% (6) |
12.4% (17) |
0.81 |
| Vascular disease |
1.7% (1) |
3.6% (5) |
0.47 |
| Renal impairment |
1.7% (1) |
1.5% (2) |
0.89 |
| Sleep apnea |
3.4% (2) |
2.2% (3) |
0.63 |
| Previous AF ablation |
20% (14) |
19.6%(32) |
0.96 |
| BMI |
28(26-31) |
27 (25-31) |
0.29 |
| Left atrial area |
22 (20-25) |
24 (21-26) |
0.09 |
| EF |
60 (59-64) |
60 (50-62) |
0.18 |
| CHADS2 |
|
|
0.18 |
| 0 |
31% (18) |
31.4% (43) |
|
| 1 |
41.4% (24) |
27.7% (38) |
|
| 2 |
17.2% (10) |
24.1% (33) |
|
| >3 |
10.3% (6) |
16.7% (23) |
|
| Paroxysmal AF |
79.3% (46) |
78 (108) |
0.40 |
| Medical Operator |
|
|
0.89 |
| 1 |
55.2% (32) |
50.4% (69) |
|
| 2 |
22.4% (11) |
25.5% (35) |
|
| 3 |
12.1% (7) |
14.6% (20) |
|
| 4 |
10.3% (6) |
9.5% (13) |
|
Table 2. Admissions and complications after discharge.
| Results |
Same-day discharge(58) |
Overnight hospitalization (137) |
p |
| ER admission |
15.5% (9) |
30.7% (42) |
0.03 |
| Time to ER admission |
72 (36-120) |
48 (36-96) |
0.44 |
| AF |
5.2% (3) |
8.8% (11) |
0.55 |
| Vascular complications |
3.4% (2) |
3.6% (5) |
0.94 |
| Pericarditis |
0% (0) |
1.5% (2) |
1.00 |
Mean skin-to-skin time was 91.5 minutes and mean fluoroscopy time was 10.4 minutes. Mean ablation time with radiofrequency was 9.9 minutes for the same day discharge group and 11.7 minutes for the overnight hospitalization group.
Mean ablation time using cryoballoon was 227.21 seconds per vein (224.8 seconds in the same-day discharge group vs. 227.1 seconds in the overnight hospitalization group). Mean temperature reached was -44.9°C (-45.9°C in the same-day discharge group vs. -44.6°C in the overnight hospitalization group) and 3.9 pulmonary veins were treated in each procedure. Eighty patients underwent cryoballoon ablation, 20 (25%) of which were discharged on the same day, while 115 patients underwent radiofrequency catheter ablation and 32 (28%) were discharged on the same day. There were no significant differences between both techniques. Transesophageal echocardiography to guide transseptal puncture was used in 27.5% of the procedures (21% same-day discharge vs. 35% in the overnight).
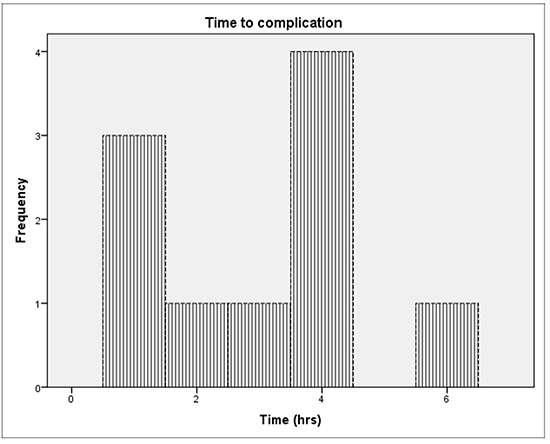
Only 10 complications were observed during the period evaluated and motivated longer hospital stay. For practical reasons, the moment complications developed was prospectively assessed. Patients who suffered adverse events were not included in the final analysis. Of the 10 complications, two were pericardial effusions requiring drainage, five vascular complications (hematomas > 5 cm and one of them was a fistula requiring surgical correction), two patients developed phrenic nerve injury and one presented with pericardial syndrome. Most complications were detected during the procedure and none presented after the sixth hour. The results are presented in [Figure 1].
Figure 1. : Distribution of complications by hour
All the patients initially included were followed-up at 30 days. We observed a significant difference in the number of visits to emergency department: 15.5% for the same-day discharge group vs. 30.7% for the overnight hospitalization group (p 0.03).
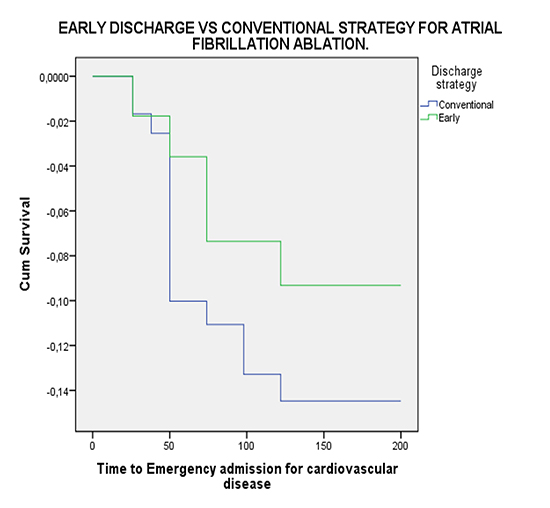
In [Figure 2], the Kaplan-Meier curves show that patients in the overnight hospitalization group visited the emergency department earlier than those in the same-day discharge group.
Between the reasons to visit the emergency department, atrial fibrillation and vascular complications were the most common reasons (7% and 3.5%, respectively), without significant differences between both groups. No cases of pericardial tamponade were reported and none of the patients required new hospitalization
Figure 2. Kaplan-Meier curve showing time to consultation
Patients in the overnight hospitalization group remained hospitalized for an average of 25.03 h versus 10.9 h in the same-day discharge group. Considering that the daily cost of coronary care unit stay is U.S is $864, this represents a cost of $43,214.1 every 50 patients in the overnight hospitalization group and of $17,678.5 in the same day discharge group. The cost was determined by the total ward budget plus an allowance for supporting medical staff and nurses.
This study demonstrates the feasibility of same-day discharge after PVI. This approach shows to be safe and does not require new hospitalizations compared with overnight discharge.Most importantly, in our experience,hospitalization for 24 hours after PVI does not detect more complications than discharge on the sameday. Pulmonary vein isolation has been performed for 20 years and is considered as one of the most complex interventions requiring highly trained professionals within the specialty.
Patients remain hospitalized for at least 24 hours following the procedure worldwide but there is no reliable evidence supporting this approach [1]. This is due to the low number of studies evaluating the appropriate timing of hospital discharge in this population, making it necessary to use the experience of other areas of interventional cardiology. A meta-analysis reported that same-day discharge after uncomplicated percutaneous coronary intervention seemed to be a safe approach in selected patients.
Information about the number of hours necessary to detect complications after an electrophysiology procedure other than PVI is not abundant [2]. Most studies focus on patients undergoing various types of catheter ablation procedures, most of which do not require the use of transseptal puncture. A single-center study conducted by Faizel Osman in the U. K. in 2015 demonstrated that single-day discharge after conventional catheter ablation was a safe approach. The benefit observed was significant in terms of reduction of costs and logistic constrains to manage patients per bed. In our study, we found similar results using a more complex practice and with higher number of complications. We did not find differences in the rate of complications between both strategies, with no impact on new hospitalizations or visits to the emergency department. In our study, we have tried to answer if same-day discharge after a procedure requiring transseptal puncture is a safe strategy [3].
In the worldwide survey published in 2010, the rate of events was similar to that of the international registries in 2010. Our patients did not present severe complications such as stroke or death. In this study, the rate of these complications was 0.7%% and 0.2%, respectively. The power of our population was not strong enough to detect similar events.
As an added value, we have made efforts to determine the moment that complications occur during post-procedural monitoring. Of importance, no events occurred after the sixth hour. The predictors of complications are well-known, [4] such as age, peripheral vascular disease, diabetes and chronic obstructive pulmonary disease. Our population was relatively young and with low rate of complications.
Transseptal puncture is probably a critical moment of the procedure and, since it was developed, it has been performed under fluoroscopy guidance with adequate safety. However, imaging provides a significant support to reduce complications. High-resolution computed tomography angiography provides information about the composition of interatrial septum, left atrial volume and type of left atrial appendage. Transesophageal and intracardiac echocardiography have proved to be extremely useful[5]. The importance of real-time images to monitor potential complications has been demonstrated by many studies. Transesophageal echocardiography is important for repositioning the transseptal needle in 16% of patients and to avoid transseptal-puncture related complications[6,7].
As with all observational prospective trials, our study may include biases and the results may not be extrapolated to other populations. A selection bias undoubtedly exists. While the most important variables in assessing susceptibility to complications showed no differences between both groups, it is undeniable that certain factors that occur during the procedure may not be evident. It is also important to mention that due to the low incidence of serious adverse events, the number needed to show a significant difference in a randomized trial is too high and may be not feasible.
A high number of procedures are carried out at the institution each year, as reflected by the number of cases presented in the study. In addition, the study was conducted at an institution specialized in cardiovascular diseases. Both conditions could affect the external validity of the results obtained.
Same-day discharge after PVI might be safe and cost-effective. This is the first study analyzing the experience in patients undergoing complex ablation with transseptal puncture. In this trial we register that complications presented during the procedure or a few hours after may reduce the time of hospitalization. This approach would provide significant benefits for patients and health care providers. Although, a larger and/or randomized trial is needed to confirm the findings of this study.






