Baselinecharacteristicsof the 95 included patients did not show any significant differences [Table 1]. The sample was predominantly men around the age of 60. Persistent AF comprised a larger proportion of the sample (60%)than paroxysmal AF.
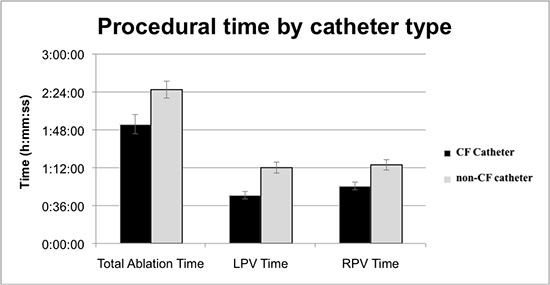
For the procedural analysis, data was complete for 86 patients. In each of the categories measured, there was a reduction in procedural time and total radiofrequency application time when a CF catheter was used [Table 2]. Theuse of a CF catheter significantly reduced the mean total ablation time by about 33 minutes (1 hour and 53 minutes compared to 2 hours and 26 minutes, p=0.011). LPV and RPV times were both significantlyshorter in the CF ablation group as well[Figure 1]. There was no difference in the ability to reinducesustained atrial fibrillation, non-sustained atrial fibrillation, or other arrhythmias between catheter types [Table 3].
Table 2. Procedural Times. Independent two samples two-tailed t-test of left, right, and total ablation time by catheter used.
|
Total Ablation Time |
LPV Time |
RPV Time |
|
Contact Force |
Non-Contact Force |
Contact Force |
Non-Contact Force |
Contact Force |
Non-Contact Force |
| N |
47 |
39 |
47 |
40 |
47 |
39 |
| Mean |
1:53:24 |
2:26:16 |
0:45:51 |
1:12:07 |
0:54:41 |
1:14:43 |
| STD |
1:03:38 |
0:51:11 |
0:24:44 |
0:33:55 |
0:25:28 |
0:31:33 |
| p-value |
0.011 |
<0.001 |
0.002 |
Table 3. Arrhythmia Inducibitily. Independent two samples two-tailed t-test of left, right, and total ablation time by catheter used.
|
Contact Force (N=46) |
Non-Contact Force (N=37) |
Chi-squared |
P value |
| Non-inducible |
21 |
13 |
0.094 |
.30 |
| AF |
6 |
8 |
|
.33 |
| Non-sustained AF |
2 |
3 |
|
.47 |
| Typical AFL |
17 |
9 |
|
.22 |
| Atypical AFL |
0 |
4 |
|
.02 |
* Inducibility testing was not performed on 1 patient in the Contact Force group and 3 patients in the non-Contact Force group. These are excluded. * Bonferroni correction method was used to correct for multiple comparison post-hoc (adjust p-value=0.05/5= 0.01). No significant differences were found.
Figure 1. Graph of total, left pulmonary vein, and right pulmonary vein ablation time by catheter used.
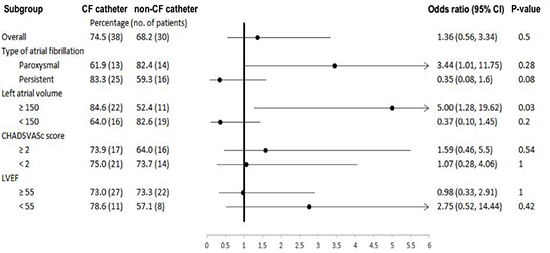
We chose 2 time points to evaluate for AF recurrence: 3 months—frequently considered the blanking period—and 12 months after ablation. No differencein the percentage of patients in sinus rhythm was detected between the CF and non-CF groups (74.5% and 68.2%, respectively; p=0.50) at the 3-month follow up period [Table 4a].The overall 12-month incidence of sinus rhythm was also not significantly different [Table 4b]; [Figure 2]).Subgroup analysis done at 12-month follow up showed that sinus rhythm was more frequent with CF compared to non-CF in patients with an LA volume greater than 150 cc compared (84.6% and 52.4%, respectively; p=0.03). There was no difference in outcomes with stratification by CHA2DS2VASC score or LVEF.
Table 4a. Clinical Outcomes. Patients in sinus rhythm after 3-months based on disease characteristics and catheter used.*
|
Contact Force |
Non-Contact Force |
P value |
| Overall patients in sinus rhythm, % (n) |
|
78.4 (40) |
68.2 (30) |
0.26 |
| Type of AF |
Paroxysmal |
71.4 (15) |
70.6 (12) |
1.00 |
|
Persistent |
83.3 (25) |
66.7 (18) |
0.22 |
| LA volume, cc |
≥ 150 |
76.9 (20) |
61.9 (13) |
0.34 |
|
< 150 |
80 (20) |
73.9 (17) |
0.74 |
| CHA2DS2VaSc score |
≥ 2 |
82.6 (19) |
64.0 (16) |
0.20 |
|
< 2 |
75.0 (21) |
73.7 (14) |
1.00 |
| LVEF, % |
≥ 55 |
78.4 (29) |
80.0 (24) |
1.00 |
|
< 55 |
78.6 (11) |
42.9 (6) |
0.12 |
* Chi-square used for overall analysis while fisher's exact test used for subgroup comparisons as some cells contained numbers <10
Table 4b. Clinical Outcomes. Patients in sinus rhythm after 12-months based on disease characteristics and catheter used.*
|
Contact Force |
Non-Contact Force |
P value |
| Overall patients in sinus rhythm, % (n) |
|
74.5 (38) |
68.2 (30) |
0.50 |
| Type of AF |
Paroxysmal |
61.9 (13) |
82.4 (14) |
0.28 |
|
Persistent |
83.3 (25) |
59.3 (16) |
0.08 |
| LA volume, cc |
≥ 150 |
84.6 (22) |
52.4 (11) |
0.03 |
|
< 150 |
64.0 (16) |
82.6 (19) |
0.20 |
| CHA2DS2VaSc score |
≥ 2 |
73.9 (17) |
64.0 (16) |
0.54 |
|
< 2 |
75.0 (21) |
73.7 (14) |
1.00 |
| LVEF, % |
≥ 55 |
73.0 (27) |
73.3 (22) |
1.00 |
|
< 55 |
78.6 (11) |
57.1 (8) |
0.42 |
*Chi-square used for overall analysis while fisher's exact test used for subgroup comparisons as some cells contained numbers <10
Figure 2. Forrest plotcomparing patients in sinus rhythm at 12 months based on catheter used and atrial fibrillation characteristics.
Overall, there was no observed increase in complications with the introduction of CF ablation. Pericardial effusion with or without the need for pericardiocentesis occurred in 3/45 = 7% of patients prior to the introduction of CF catheter and in 1/52 = 2% of the patients who underwent ablation with a CF catheter (p=0.24). There were no strokes, deaths, bleeding episodes requiring transfusion, esophageal injuries, or phrenic nerve injuries in either group.
The intent of this study was to quantify the impact of the introduction of CF technology at the time of transition to this technology on procedural and clinical aspects of PVI. The ablation strategy, techniques, and workflow were the same but the catheter, specifically the ability to measure CF, was different. This strategy minimized confounding by other variables (e.g. changing the ablation strategy, the ablation modality, or the primary operator).
The main findings in this study of transitioning to the use of contact force catheters for atrial fibrillation ablation are that (1) procedure times, ablation times, and time to pulmonary vein isolation is reduced when contact force catheters are used; (2) clinical outcomes are similar, and perhaps improved in patients with large LA volumes; and that (3) complications rates were not increased.
As is the case with introduction of many new technologies, a learning curve is often required to become comfortable and demonstrate proficiency, thus maximizing the benefit of the innovation. Clearly, if new technology is difficult to use or if it is associated with complications it is unlikely to succeed. With the introduction of the contact force parameter there was a novel ablation parameter to follow. At times the tactile feel of the catheter would be discordant to the measured force. That is, the feeling of “heavy” force sometimes equated to a low force readings and vice versa. Confidence in the contact force recordings and calibration sometimes meant deciding which parameter (tactile feel or recorded force) represented the optimal ablation scenario. Because of this unfamiliar dilemma due to inexperience, we were reminded of the so-called “July phenomenon” (when there is a perceived decrease in the quality of health care at the start of the North American academic year for medical training).[14] Although the July phenomenon has been largely refuted,an abundance of evidence that “surgeon volume” matters across a range of operations including electrophysiology procedures.[15,16]
We found that, somewhat paradoxically, the initial use of a new ablation catheter improved procedural time and some effectiveness endpoints immediately, without the benefitof a large volume of cases. This reassured us about any concernswe had about slowingour workflow. Measuring contact force added usable information to the ablation strategy, and it also reduced ablation times, which ultimately improved workflow. The decreased procedural duration times were apparent almost immediately with adoption the contact force technology. Prior studies have shown a decrease in procedural time, but without differentiating between LPV and RPV times.[17,18]
Our study found that patients with large LA volumes (which we defined based on a previous investigation)undergoing AF ablation with a CF catheter were more likely to remain in sinus rhythm at 12 months.[9] This difference was driven by two CF patients converting to sinus between the 3 and 12 month period and two non-CF patients who convert from sinus back to AF in the same time period.One long term study has shown PV reconnection in both CF and non-CF ablated patients owing primarily to the RPV that negated a significant difference in atrial arrhythmia free survival[19].CF ablation has been shown to improve outcomes in patients with paroxysmal AF in large studies[20-22]and subsequent research on persistent AF has shown a benefit as well.[23] Patients with exclusively persistent AF and large LA enlargement, however,have been shown not to have an increase in sinus rhythm at 12 months.[24] Our analysis did not compare these two covariates directly, and it is possible that the advantage seen in our study was due to patients with large LA volumes and specifically paroxysmal AF.
Our complication rates were low in both arms, and similar to those of other studies involving CF ablations.[23,24]Larger studies with longer follow up have seen a reduction in complications with CF ablation so it is possible that we lacked significant enough power to detect a difference in complication rate[24].
Thisstudy has several limitations.First, the sample size is small. Despite initially selecting 112 charts, only 68 patients who met inclusion criteria completed their 12-month follow up. The patients lost to follow up appear in proportion between both the CF and non-CF group, but nevertheless this may result in unintended selection bias. Second, despite outpatient telemetry monitoring and regular electrocardiography it remains possible that patients had recurrences that asymptomatic and unrecorded. Third, subgroup analysis was not performed on procedural outcomes. Certain patient characteristics may have impacted procedural times. Finally, mean times to perform each AF ablation were reported. Changes in procedural time may have occurred towards the end of the CF group as the operator became more familiar with technology.






