Additional Diagnostic value of Mini Electrodes in an 8-mm Tip in Cavotricuspid Isthmus Ablation
Mol D1, Berger WR1, Khan M1, de Ruiter GS1, Kimman GP1,2, de Jong JS1, de Groot JR3
1
OLVG, department of Cardiology, Amsterdam, the Netherlands.2
Noord-West ziekenhuisgroep, department of Cardiology, Alkmaar, the Netherlands.3
Academic Medical Centre, Heart Centre, department of Cardiology, Amsterdam, the Netherlands..
Eight-mm ablation catheters are widely used in cavotricuspid isthmus ablation (CTI) for treatment of right sided atrial flutter. However a high success rate, these large ablation tips comes with adisadvantage of lower resolution of fractionated signals.
The aim of this study was to evaluate the additional diagnostic value of the electrograms recordedfrom mini electrodes (MEs) in an 8-mm ablation catheter tip during CTI.
CTI-ablation procedures were compared retrospectively in two groups, namely, group A: the Abbott Safire 8-mm tip with a 3D mapping system (n =37) and group B: the Boston Scientific MiFi IntellaTip XP 8-mm tip without a 3D mapping system (n=13). We analyzedacute procedural success, ablation characteristics and recurrence rate at one-year follow-up. Electrograms from MEs were analyzedright before the onset of the critical ablation application that resulted in acute CTI-block. We determined whether these ME electrograms had additional diagnostic value in addition to of the 8-mm tip derivedelectrogram.
At the onset of the critical ablation application, the MEs had an important additional value in 3 out of 13 cases as local signals were sensed on the MEs that were not recorded by the 8-mm tip electrode. In 2cases the ME did not show local electrogramsalthough the ablationwas still effective. Acute procedural and long-term success wereobserved in all patients. No differences were found in time to bidirectional block, procedure time or fluoroscopic exposure.
Our data show that signals recorded from the MEs had additional diagnostic value, but only in asmall percentage of the patients. We did not observe, although omitting 3D-mapping in the ME group, any differencebetween groups with regard to procedural or ablation characteristicsduring CTI-ablation.
Key Words : Catheter Ablation, Atrial Flutter, Cavotricuspid Isthmus, Mini Electrodes.
Correspondence to: Daniël Mol, Department of Cardiology
Oosterpark 9
1091 AC Amsterdam, the Netherlands
Right isthmus-dependent atrial flutter (AFL) is one of the most common supra-ventricular arrhythmias. The activation front during tachycardia travels through a macro-reentrantcircuit in the right atrium, encompassing the isthmus located between the tricuspid annulus and inferior vena cava (cavotricuspid isthmus, CTI)[1,2].Consequently, typical counter-clockwise AFL is characterized by a negative p-wave with a saw-tooth pattern in the inferior leads of the 12-lead ECG[3]. Due to the stability of the circuit, rate control can be challenging. Rhythm control strategies consist of pharmacologicaltreatment, electrocardioversion or radiofrequency (RF) ablation[4].
CTI-ablation is widely used and effective at restoring and maintaining sinus rhythm. The first reports describe the use of a 4-mm non-irrigated catheter to create anablation line of conduction block along the CTI[1].Anatomical variance among CTI patients in combination with a small ablation electrode size can cause lack of convective cooling. This may result in a temperature rise of the ablation tip and decreased power delivery. This, in turn, will result in a smaller lesion size and an increased risk of steam-pops. By using a larger ablation electrode size, more electrode surface is available for convective cooling, resulting in increased power deliveryand greater lesion size[5-8].Indeed, several investigators have described the superiority of an 8-mm ablation catheter compared to a 4-mm non-irrigated ablation catheter[9-11].However, this advantage comes at the cost of lower resolution of local fractionated electrograms. To overcome this issue,a new 8-mm tip ablation catheter was recently developed, equipped with mini electrodes (MEs) to optimize sensing of local electrograms. In this ablation catheter, three 1-mm electrodes are located within 2-mm of the ablation catheter tipwith a 2,5-mm spacing (Figure1). A small studyof Iwasawa et al[12]. and a case seriesof Tzeis et al[13]. showed conflicting outcomesin efficacy using MEs in an 8-mm catheter.Furthermore, it has not been established in for what percentage of patients MEs detect local electrograms, when electrograms on the conventional bipolar electrodes are absent. Therefore, the question remains as to whether the use of MEs results in increased procedural efficacy, and whether the use of MEs allowsa 3D navigation system to be omitted.
Population and study design
Fifty consecutive patients who underwent a CTI-ablation between 2013 and 2016 in the OLVG hospital in Amsterdam, the Netherlands were included in this analysis. The local ethics committee approved this retrospective study and issued a waiver for informed consent.
We compared two groups: group A consisted of patients undergoing CTI-ablation using the Safire F 8-mm (Abbott, Abbott Park, IL, USA) ablation catheter in combination with a 3D mapping system (n = 37); group B consisted of patients undergoing CTI-ablation using the MiFi IntellaTip XP 8-mm (Boston Scientific, Boston, MA, USA) ablation catheter without a 3D mapping system to attain an electrogram based ablation (n = 13). Patients with a prior CTI-ablation or atrial tachycardias not dependent on the CTI were excluded. Atrial size was qualitatively assessed by transthoracic echocardiogram. Ablation was performed either by using a point-by-point or focal application of about 30 seconds before dragging forward, with a maximum application duration of 240 seconds. TheRF strategy was chosen as per the operator preference. The final RF application that resulted in CTI-block was defined as the critical application. We compared the presence of interpretable intracardiac electrograms from the MEs to those intracardiac electrograms recorded from the conventional electrodes at the onset of the critical application.Interpretable cardiac recording was defined as a peak-peak amplitude of the bipolar electrogram>0.2mV at the steepest dv/dt for the conventional 8-mm tip and >0.1mVfor recordings retrieved from the MEs.In both groups we recorded procedure time, time to bidirectional block, fluoroscopic exposure, total ablation time,total number of ablation applications and the need to use a steerable sheath.
Procedural characteristics
All procedures were performed with an opioid analgesic (fentanyl) and without sedation.The femoral vein was punctured for access. A duo decapolar diagnostic catheter was placed in the right atrium around the tricuspid annulus; a quadripolar diagnostic catheter was placed in the coronary sinus. Surface ECG and intracardiac recordings were acquired with a Bard EP recording system (Boston Scientific, Boston, MA, USA).Filter settings on the ablation channel were similar for both conventional 8-mm and ME recordings. We used a30Hzlow pass filter,250Hzhigh pass filter and a 50Hz notch filter. The signals were displayed with a gain of 8. The Ensite 3D mapping system (Abbott, Abbott Park, IL, USA) was only used in group A. RF-energy was delivered using IBI-1500T11 (Abbott, Abbott Park, IL, USA); ablation generator settings were 70W and 55 degrees Celsius.Bidirectional block was assessed with bidirectional differential pacingmanoeuvres[14] and by measuring the widthof the local double potentials. Procedural success was achieved when bidirectional block was still present after a waiting period of 20 minutes after the last RF application.
Follow-up data was collectedfrom electronic patient records at one-year and by investigating all rhythm recordings performed by the referring hospitals. Recurrence was defined as registration of AFL on a 12-channel ECG, regular atrial tachycardia with a cycle length between 200-260ms in a cardiac implantable electronic device, or Holter registration. Recurrence of symptoms without documentation of arrhythmias was documented as well.
Statistical package for social science (SPSS) was used for statistical analyzes(SPSS Inc., Chicago, IL, USA). Normally distributed continuous variables are presented with a mean and a standard deviation, non-normally distributed with a median and an interquartile range, categorical variables in numbers and percentages.The parametric independent T-test and non-parametric Mann-Whitney U-test were used for statistical analysis of continuous variables, while X2 and Fisher’s exact test were used to compare numbers between groups.
We included 50 patients with a typical AFL (n=37 in group A vs.n=13 in group B) of whom84% were male.Mean age was 63.3 ±8.6 years. Right atrium dilatation was present in 41.5% of the patients (n=11 vs.n=6 patients p=0.678). Counter-clockwise activation was observed in 46 patients (n=35 vs.n=11 p=0.069) whereas clockwise activation was also observed in 7 of these patients (n=5 in group A and n=2 in group B). Baseline patient characteristics are summarized in [Table 1]. Twenty-one patients (56.8%) in group A and 5 patients (38.5%) in group B had a history of atrial fibrillation (p=0.265).In group A 3 patients (8.1%) used flecaïnide compared to 5 (38.5%) in group B (p=0.010). [Figure 1A]
shows a graphic of the localization of MEs on the ablation catheter and [Figure 1B] shows the conventional ablation catheter.
Figure 1. 8-mm ablation catheter with 1-mm mini electrodes within a 2-mm distance from the ablation tip and a 2,5-mm spacing. B, conventional 8-mm ablation catheter with a 2-5-2 electrode spacing.
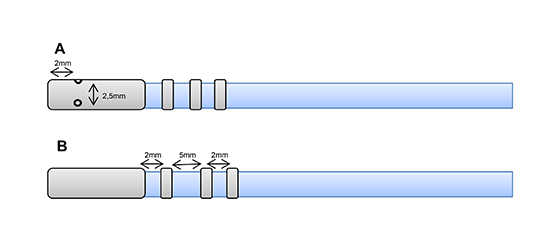
Table 1. Baseline characteristics
| Baseline characteristics |
Abbott Safire N=37 |
Boston Scientific MiFi N=13 |
P value |
|
Male
|
31 (83.8)
|
11 (84.6)
|
0.944
|
|
Age
|
63.3 ±8
|
64 ±11.7
|
0.924
|
|
Body mass index
|
25.7 [22.2-30.3]
|
28.4 [24.2- 32.9]
|
0.201
|
|
Structural heart disease
|
20 (54.1)
|
10 (76.9)
|
0.148
|
|
Ejection fraction
|
53.7 ±12.4
|
51.4 ±10.2
|
0.639
|
|
Right atrium dilatation
|
11 (39.3)
|
6 (46.2)
|
0.678
|
|
Left atrium dilatation
|
17 (60.7)
|
7 (66.7)
|
0.722
|
|
Counterclockwise flutter
|
35 (100)
|
11 (84.6)
|
0.069
|
|
Clockwise flutter
|
5 (14.3)
|
2 (15.4)
|
0.622
|
| Paroxysmal atrial flutter (<7days) |
21 (65.6)
|
8 (61.5)
|
0.948
|
| Persistent atrial flutter |
11 (34.4)
|
4 (33.3)
|
0.948
|
|
Atrial fibrillation
|
21 (56.8)
|
5 (38.5)
|
0.256
|
|
CHA2DS2 VASc
|
2 (1-2)
|
3 (0.5-3)
|
0.482
|
|
Congestive heart failure
|
4 (10.8)
|
2 (15.4)
|
0.497
|
|
Hypertension
|
17 (45.9)
|
8 (61.5)
|
0.333
|
|
Diabetes
|
8 (21.6)
|
2 (15.4)
|
0.629
|
|
Stroke
|
2 (5.4)
|
1 (7.7)
|
0.604
|
|
Vascular disease
|
8 (21.6)
|
3 (23.1)
|
0.913
|
|
Beta blockers
|
27 (73)
|
8 (61.5)
|
0.439
|
|
Flecainide
|
3 (8.1)
|
5 (38.5)
|
0.010
|
Congestive heart failure, hypertension, age (75), diabetes, stroke, vascular disease, age (65), sex (CHA2DS2 VASc). Mean ±SD, numbers (%), median [25-75 percentiles].
CTI ablation was associated with acute procedural success of100% inboth groups. There was no difference in any of the predefined ablation or procedural characteristics, as summarized in [Table 2]. In particular, there was no difference with respect to the total procedure duration, fluoroscopic time or time to bidirectional block. A steerable sheath was used in 2 patients in each group (p=0.275).Long-term outcomes arepresented in [Table 2].There was no recurrence of documented atrial flutter in any patient at one-year follow-up.Seventeen patients (34%) had symptoms of palpitations after CTI-ablation (n=13 (35%) vs.n=4 (31%)p=0.775). Whereas, 19 patients (39%) had documentation of a different atrial arrhythmia (n=14(38%) vs.n=5 (38%)p=0.968).[Figure 2]
shows a typical example of local electrograms from the MEs versus those derived from the conventional electrode at the onset of the critical RF application. Interpretable local electrograms were present on the MEs, but absent on the ablation catheter in 3 out of 13 patients. Local electrograms were detectable with both modalities in 8 out of 13 patients. Finally, there were no local electrograms detectable with the MEs in 2 out of 13 patients. Hence, an additional diagnostic advantage was demonstrated in only 3 out of 13 (23%) of the patients. Notably, there was no difference in any of the ablation characteristics in these patients with detectable electrograms on the MEs and the absence of the electrograms on the conventional electrode, also not with respect to the more frequent use of flecainide in the ME group. The recording in [Figure 3A]
demonstrates a case where double potentials across the ablation line were recorded on the MEs but not on the conventional catheter tip. [Figure 3B] presents an example of a site of re-conduction after multiple ablation applications. Here also, small local electrograms were only observed in the MEs (box). In these cases, we were able to identify these electrograms recordedfrom the MEs but not from the conventional catheter tip.
Figure 3. : A, double potentials measured across the ablation line. Note, local signals were only observed on the ME (box). Whereas, no signals were observed on the conventional electrogram (MAP 1-2, arrow). B, intra cardiac electrogram of an area of re-conduction after multiple ablation applications. Small fractionated signals were only observed on the ME (box). Whereas, no signals were observed in de conventional electrogram (MAP 1-2, arrow).
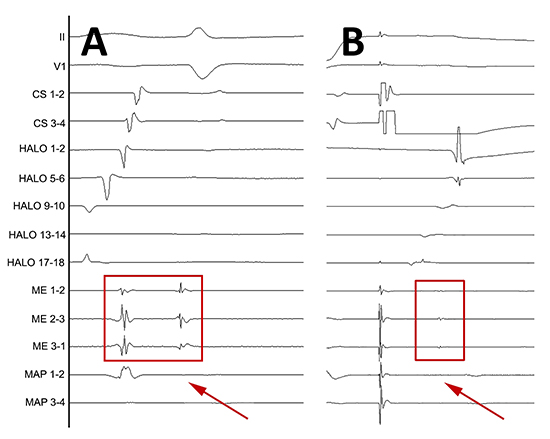
Figure 2. Intra cardiac electrogram before critical ablation point measured on mini electrodes (ME 1-2,2-3,3-4) and between the 8-mm electrode and the second electrode (MAP 1-2, boxes).
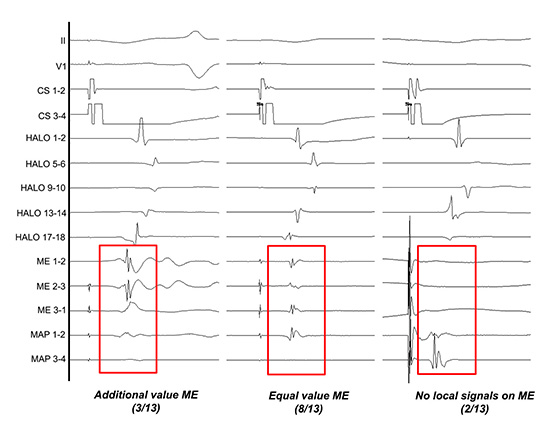
Table 2. Procedural characteristics and follow-up
| Procedural characteristics and follow-up |
Abbott Safire
N=37
|
Boston Scientific MiFi N=13
|
P value
|
|
Ablation:
|
|
|
|
| Number of RF-applications |
6 [3.5-10]
|
8 [2.5-14]
|
0.838
|
| Average duration per application (sec) |
70.2 ±33.7
|
60.5 ±22.6
|
0.343
|
| Average temperature (Celsius) |
49.5 ±1.9
|
52.53 ±3.5
|
0.059
|
| Average impedance (ohm) |
74.5 ±5.6
|
74.2 ±6.1
|
0.912
|
| Average power (Watts) |
46.4 ±11.6
|
45.24 ±12.9
|
0.365
|
| Total ablation time (sec) |
456 [263-661.8]
|
364 [181-821]
|
0.550
|
|
Procedure:
|
|
|
|
| Concomitant PVI |
0 |
1 (7.7) |
0.260 |
|
Cross-over
|
0 (0)
|
0 (0)
|
-
|
|
Steerable sheath
|
2 (5.4)
|
2 (15.4)
|
0.275
|
| Time to bi-directional block (min) |
23 [12.5-37.5]
|
16 [3-23]
|
0.217
|
|
Fluoroscopic time (min)
|
13 [8-17]
|
18 [7-22]
|
0.631
|
|
Procedure time (min)
|
65 [53-80.5]
|
50 [34.75-73.25]
|
0.133
|
|
Follow-up:
|
|
|
|
| Recurrence of atrial flutter at one-year |
0 (0)
|
0(0)
|
|
|
Recurrence of symptoms
|
13 (35.1)
|
4 (30.8)
|
0.774
|
| Occurrence of other atrial arrhythmia |
14 (37.8)
|
5 (38.5)
|
0.960
|
Pulmonary veins isolation (PVI). Mean ±SD, numbers (%), median [25-75 percentiles].
This study is the first reporting follow-up data on atrial flutter ablation using an 8-mm ablation catheter with MEs. MEs detected local electrograms more accurately than the conventional large ablation electrodes in 3 out of 13 (23%) patients. Using MEs without a 3D mapping system resulted in similar procedure time, fluoroscopic exposure and RF time to achieve bidirectional block.
MEs in a conventional ablation catheter is a relatively novel catheter design and evidence supporting the efficacy of MEs in an 8-mm ablation catheter during CTI-ablation is lacking.In a small case series published byTzeis et al., which included 6 patients,bi-directional block was achieved in allpatients, and procedural characteristics were comparable with the conventional 8-mm ablation catheter[13].Iwasawa et al. performed a small prospective studyin which they compared an 8-mmcatheter with MEswith the conventional 8-mm and cryo ablation catheter. A high cross-overrate was observed in the MEs group (14 out of 25 patients, 56%),whereasno cross-overs occurred in the conventional group (0 out of 30, 0%). Also, there were 3(out of 30)cross-over patients (10%) in whoma cryo ablation catheter was used. Thehigh cross-over rate was explained by a decreased power delivery during temperature-controlled ablation due to an isolated temperature sensor[12].In our study,we observed a 100% procedural success rate in 13 patients treated with the ablation catheter with MEs. However, the additional diagnostic value of the MEs was seen in 23%, equal value in 62% and absence of ME electrograms in 15% of the patients in group B. We speculate that the lackof additional diagnostic valueresults is partly due to theoblique positioning of the large electrode,resulting in floating MEswithout tissue contact while the large ablation tip had sufficient tissue contact.Of note, one could argue that a point-by-point ablation strategy would be most appropriate when investigating MEs. However, our study describes the use of MEs in a real-world clinical setting rather than in a randomized trial environment. The finding of a higher temperature in the MEs group in a previous study is in contrast with our findings[12].However, there was a trend towards higher ablation temperature in our MEs group (49.5 ±1.9 vs. 52.5 ±3.5p=.059),but this did not influence the power delivery (46.4 ±11.6 vs. 45.2 ±12.9p=.365) or the ability to create bidirectional block.
In our experience, a small learning curve exists when using the MiFi Intellatip XP 8-mm ablation catheter. Reduction of ME electrogram amplitude can be misinterpreted asa marker of ablation lesion completion. Once ablation was started, ME electrograms rapidly disappeared. These findings are in concert with a previous study which described a rapid decrease of ME amplitude within 7.3 ±3.9s[15].Meanwhile, based on maximum ME amplitude attenuation, a transmural lesion was formed after 25.9 ±8.1s in canine atria[16].Dragging the ablation catheter further after reduction of amplitude in the ME electrograms tended to create superficial transient lesions that needed additional ablation.
Multi-electrode diagnostic catheters with small electrode sizes and spacing are being employed for high and ultra-high resolution 3D maps of scar and densescar, revealing areas of slow conduction[17].Voltage maps are more accurate when 1-mm electrodes with small inter-electrode spacing are used. Due to better sensing abilities, a 64% increase in amplitude was observed. This may result in a reduction inthe total amount of dense scar in a 3D mapping system of one-third at a cut-off value of <0.05mV and even two-thirds at a cut-off value of <0.25mV. Remarkably, this difference was not found in healthy atria where the electrogram amplitude is generally high[18]. Furthermore, smaller electrodes allow better annotation of fragmented electrograms during tachycardia and are associated with lower pacing thresholds during entrainment pacing[18,19].A lower pacing output reduces the amount of saturation of the amplifier, making electrograms during entrainment pacing better interpretable[20] .Regarding the voltage cut-off values, decreasing these values will improve the visualization of channels within the scar. For these reasons it appears rational to use closely space electrodes when searching for small channels, such as MEs. Also, the closer spacing and dimensions of the MEs allowed us to use stricter cut-off criteria for interpretable electrograms than in the conventional 8-mm tip recordings. Which value we should use to define scar is asubject of on-going discussion, and it remains unclear whether consensus voltage cut-off values are relevant to the CTI-ablation. Taken together, mapping techniques for visualization of small local electrograms are improving.Recording and localizing these specific electrograms using an 8- or 4-mm ablation catheter can be challenging, and MEs couldbe helpful in these cases.As displayed in two examples inFigures 3, electrograms may be present on MEswhile not discernible on the conventional catheter tip, and can indeed be helpful in the assessment of the width of double potentialsand the detection of reconnection. Indeed, also other manufacturers are now introducing similar technology to better identify small or fractionated local electrograms[21].
This study is a single-centre retrospective study with a small sample size. The study is underpoweredfor outcome analysis, mainly because an optimal success rate was achieved in both arms. Either point-by-point ablation or dragging with intermittent focal ablation was used depending on the preference of the operator and not systematically applied. Indeed, point-by-point ablation should have preference when searching for conduction gaps. However, our study describes the use of ME technology in a real-world clinical setting, and the proportion detectable and non-detectable MEs should be interpreted in that setting.Follow-up data was collected retrospectively, but all available rhythm recordings from referring hospitals were included in the analysis. However, despite these limitations, we were able to assess the absence of increased procedural or long-term efficacy of the CTI-ablation procedure.
In conclusion, the data show that MEs have added value to detect local electrograms in a fraction of patients. Our data did not show a trend towards reduced effectiveness but suggest that MEs may allow omitting a 3D mapping system. Identifying local electrograms with MEs can potentially be helpful in specific cases where one is searching for small, local fractionated electrograms.






