Successful Percutaneous Closure of Traumatic Right Ventricular Free Wall Rupture Using Amplatzer Vascular Plug Devices
Tawseef Dar1, Bharath Yarlagadda1, Prasad Gunasekaran1, Dhanunjaya Lakkireddy1, Mark A. Wiley1
1Cardiovascular Research Institute, University of Kansas Hospital and
Medical Center, Kansas City, KS.
Ventricular free wall rupture (VFWR) is a rare entity and is mostly related to post myocardial infarction (MI) complications usually involving left ventricle. In traumatic chest injuries, the right ventricle (RV) is more commonly involved due to its anatomic and structural vulnerability, as in our case. Survival, although rare, has almost always been secondary to urgent surgical repair, which is the current standard of care for such cases. However, extremely tenuous hemodynamic parameters preclude urgent surgical interventions in most of these cases. Surgical repair was considered to have prohibitive risk in our case also due to multiple comorbidities. Our case offers a unique perspective into the feasibility and safety of percutaneous closure of VFWR with devices such as Amplatzer Vascular Plug (AVP) II under transesophageal echocardiography (TEE) and angiographic guidance in patients who survive VFWR. The lack of randomized evidence to standardize the duration and regimen of antiplatelet therapy following placement of these devices is to be noted.
Key Words : Leak, Repair, Angiography, Sac, Chest trauma.
Correspondence to: Tawseef Dar, Cardiovascular Research Institute, University of Kansas Hospital and Medical Center, Kansas City, KS
Traumatic ventricular free wall rupture (VFWR) has a reported incidence of 0.3%-1.1 %. Most often VFWR is related to post myocardial infarction (MI) complications and usually involves left ventricle[1,2]. However autopsy results on chest trauma patients report a much higher incidence (35%-60%), indicating immediate fatality of myocardial ruptures in most cases[3]. Reported mortality rates range from 30%-80%, especially in acute traumatic cases[4],[5]. Emergent surgical intervention is an important predictor of outcome. However, extremely tenuous hemodynamic parameters preclude urgent surgical interventions. We report a case of traumatic VFWR successfully repaired percutaneously with multiple Amplatzer Vascular Plug (AVP II) devices.
An 80 year old man with prior coronary artery by-pass grafting (CABG) was admitted with a blunt cardiac injury with VFWR confined to the right ventricle (RV) apical segment and contained by an apical sac (28 mm x39 mm x 54 mm), thereby preventing tamponade [Figure 1-A and B] [Figure 2-A and B]. The defect was single (10 mm x 10 mm) and no specific fenestrations were noted. Given the presence of multiple comorbidities including pulmonary contusion, multiple spinal fractures and a prior sternotomy, surgical repair was considered to have prohibitive risk and a percutaneous closure was performed.
Figure 1 A. Transesophageal Echocardiography (TEE) images showing right ventricular rupture with a “contained sac”.1A-showing the neck of the sac measuring around 2 cm. IB-showing the Doppler flow through the defect.
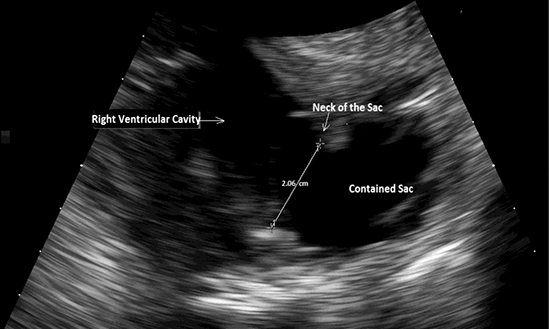
Figure 1 B.
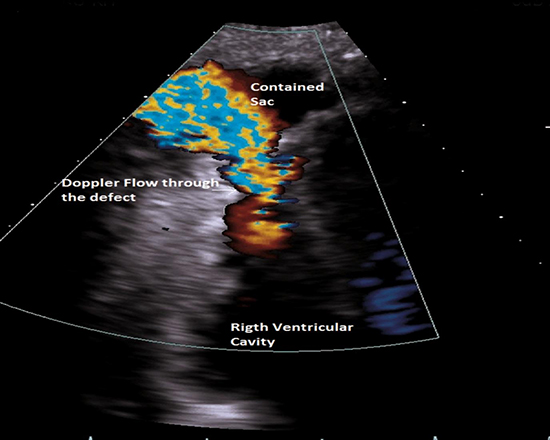
Figure 2A &2B. Coronal section and Sagittal section of Computed tomography (CT) with contrast of chest showing right ventricular free wall defect with “contained sac”. Note that there was only one defect with dimensions of 9.89 mm x 10.36 mm and the dimensions of the “contained sac” were 28.33 mm x38.94 mm x 54 mm.
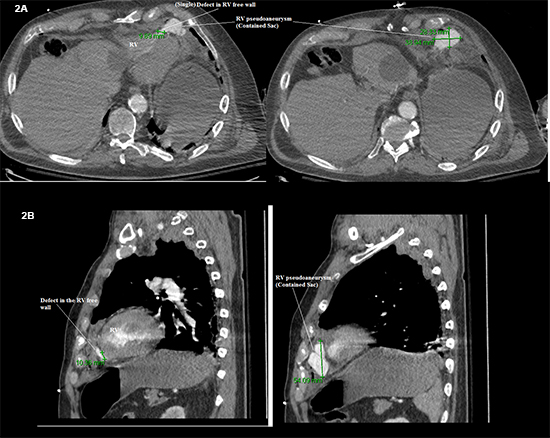
RV-Right ventricle
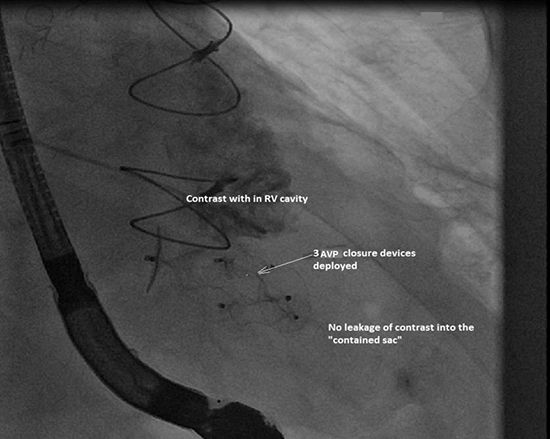
Bilateral common femoral venous accesses (14-French (F) on the right for device delivery and 6F on the left for pigtail catheter for RV angiography and angiographic visualization of the defect) were obtained[Figure 3A-I and II]. Intra-procedurally, a ventricular septal defect closure device was found to be disproportionately small compared to the defect. A 10-F Amplatzer delivery system was advanced into the right atrium over a 0.035 J wire. We then advanced a 0.035 wire into the right ventricle over which a 5F angled Glide catheter was advanced. A 0.035 Storq wire was used to access the RV apex and subsequently track the delivery system over the latter. A 22 mm AVP II device was deployed. This appeared to occlude the defect to a significant extent with moderate residual leak. We redirected the 5F angled Glide wire micro catheter system over a 0.035 Storq wire and successfully delivered a 12 mm AVP II device followed by a third 14 mm AVP II device adjacent to the initial device. Following device deployment, there was near complete resolution of the leak into the apical sac as noted based on transesophageal echo (TEE) and RV angiography using the pigtail catheter [Figure 3B]. Immediate post-procedural TEE and 1-day post procedural echo confirmed successful closure and the absence of more than a trivial leak into the apical sac. The patient remained hemodynamically stable throughout the procedure. Considering the high bleeding risk of our patient with multiple injuries, aspirin 81 mg daily was preferred for antiplatelet therapy. Seven days after successful closure of the pseudoaneurysm, the patient developed fatal respiratory failure from significant pulmonary contusions, multiple rib fractures while on aspirin mono therapy. Aspirin was discontinued 3 days after the procedure in view of worsening respiratory failure due to concerns of expansion of pulmonary contusions. However, 2-D echocardiography performed 1-day prior to death demonstrated normal biventricular function and no evidence of thrombus formation at the site of AVP deployment after aspirin discontinuation. Color Doppler confirmed the absence of significant residual flow or enlargement of the pseudoaneurysm.
Figure 3A(I) Illustrating the angiographic visualization of the right ventricle and the “contained sac”. 3A (I and II)-showing contrast leakage from right ventricular cavity through the defect into the “contained sac”. 3B-showing 3 AVP (amplatzer vascular plug) II closure devices deployed with no leakage of contrast into the “contained sac”.
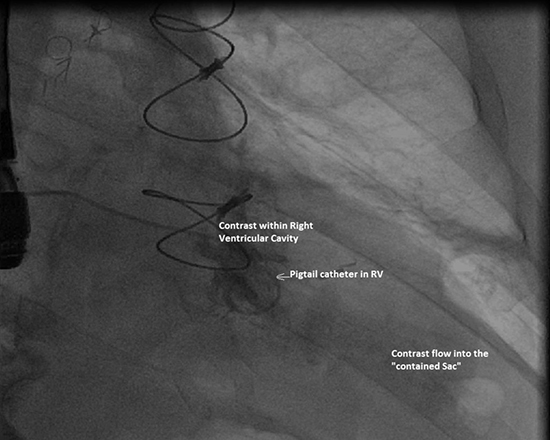
Figure 3A(II).
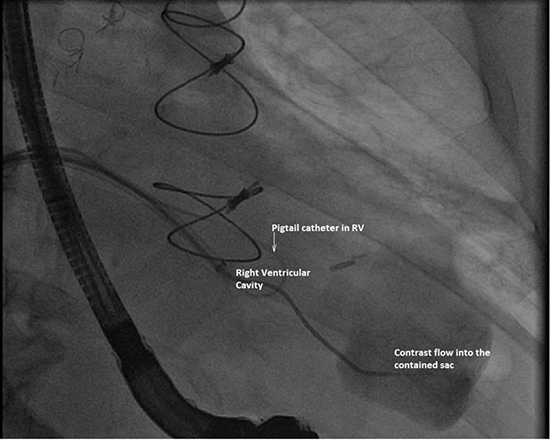
Figure 3 B.
In traumatic chest injuries, the RV is more commonly involved due to its anatomic and structural vulnerability[4]. VFWR results in severe hemorrhage into the pericardial space leading to cardiac tamponade. Survival, although rare, has almost always been secondary to urgent surgical repair. Previously, patients who survived were reported as having subacute ruptures rather than acute[6]. Percutaneous closure using an AVP II device, is a well-known technique with high success rates (>95%) and is an alternative to surgical repair[7].
Our case offers a unique perspective into the feasibility and safety of percutaneous closure of VFWR with percutaneous closure devices such as AVP II under TEE and angiographic guidance in patients who survive VFWR (mostly a fatal condition otherwise) and are not candidates for surgical repair. The lack of randomized evidence to standardize the duration and regimen of antiplatelet therapy following placement of these devices is to be noted.






