Warfarin Use and Mortality, Stroke, and Bleeding Outcomes in a Cohort of Elderly Patients with non-Valvular Atrial
Fibrillation
Bradshaw Pamela J1, Hung Joseph 2, Knuiman Matthew 1, Briffa Thomas G1, Nedkoff Lee1, Katzenellebogen Judith M1, Rankin Jamie M3, Sanfilippo Frank M1
1School of Population and Global Health, The University of Western Australia, Perth, Western Australia.2School of Medicine, Sir Charles Gairdner Hospital Unit, The University of Western Australia, Perth, Western Australia .3Cardiology Department, Fiona Stanley Hospital, Murdoch, Western Australia.
To determine exposure to warfarin and the associated outcomes in a population of older patients with non-valvular atrial fibrillation (NVAF)
Cohort study of patients aged 65-89 years admitted to hospital July 2003-December 2008 with newly-diagnosed or pre-existing AF. Outcomes at three years among one-year survivors post-index admission (landmark date) were all-cause mortality, stroke/systemic thromboembolism (stroke/TE) and bleeding. Multivariate Cox models were used to identify factors associated with each outcome.
AF was the principal diagnosis for 27.5% of 17,336 index AF admissions. Of 14,634 (84.4%) patients alive at one-year 1,384 (9.5%) died in the following year. Vascular disease (42%) was the most frequent cause of death.
Warfarin use, prior to the index admission and/or the 1-year landmark, did not exceed 40%.
Compared to non-exposure or discontinuation at the index admission, initiation or persistence with warfarin prior to the landmark date was associated with reduced risk for all-cause mortality, a statistically non-significant reduction in risk for stroke/TE, and an increased risk for bleeding. Higher CHA2DS2-VASc scores were associated with increased risk for each outcome.
In a population-based cohort of hospitalised NVAF patients, the initiation and persistent use of warfarin was associated with lower all-cause mortality risk to three years, although reduction in risk for stroke/TE did not reach statistical significance. The apparent under-use of warfarin in this older, high-risk cohort reinforces the opportunity for further reduction in stroke/TE with the uptake of non-vitamin K oral anti-coagulants (NOACs) among those not prescribed, or not persistent with, warfarin.
Key Words : Atrial Fibrillation, Clinical Outcomes, Warfarin, Population Study, Linked Data, Landmark Analysis.
Correspondence to: Dr Pamela Bradshaw, School of Population and Global Health, M431, The University of Western Australia, Perth WA 6009 Australia ORCID:0000-0003-2560-2537
Atrial fibrillation (AF) is the most frequent arrhythmia among older adults, being less than 1% before the sixth decade but doubling with each subsequent decade [1]. It is associated with increased risk for thromboembolic stroke and increased mortality. In a meta-analysis of randomised trials the use of an oral anticoagulant (warfarin) for high-risk patients, when compared to no antithrombotic treatment, was estimated to reduce the risk for thromboembolic stroke by 60% and mortality by 25%. Antiplatelet medication alone also reduced the risk for stroke, but risk was reduced by a further 40% by the use of adjusted-dose warfarin [2].
While the vitamin K antagonist warfarin has been the mainstay of stroke prevention for decades, its use is declining in favour of non-vitamin K oral anticoagulants (NOACs). A recent count of prescriptions filled under the Australian Pharmaceutical Benefits Scheme (PBS) for those eligible through the Department of Veteran’s Affairs reported that NOACs were 67% of anticoagulants supplied for AF by mid-2017 [3]. Similar trends are reported from population studies in other countries [4-6]. Despite the increasing uptake of NOACs, warfarin is still a current first-line recommendation for stroke prevention [7,8], and switching from NOACs to warfarin occurs [9].
While warfarin use continues, population outcomes for patients with non-valvular AF (NVAF) remain of current interest. They provide data for future risk/benefit comparisons as the use of NOACs accelerates, and are pertinent to prescribers and patients in ageing populations.
The aim of this study was to examine the effect of exposure to warfarin on all-cause mortality, fatal and non-fatal stroke or thromboembolism (stroke/TE), and serious bleeding events in a population of older patients with AF.
Data sources and AF cohort
This analysis was a sub-study of the WAMACH study which used linked administrative data from the Hospital Morbidity Data Collection (in-patients) and Death Register from the Western Australian Data Linkage System, linked to PBS dispensing records.
The WAMACH study cohort has been described in detail previously and includes patients hospitalised in Western Australia for ischaemic heart disease (IHD), heart failure (HF) or atrial fibrillation [10]. The current study cohort was restricted to age 65 years or more, as seniors gain concessional access to PBS listed drugs. The remaining cost after the lower co-payment is met by the Australian Government, giving rise to a dispensing record in the PBS data. This captures the majority of warfarin users as approximately 90% of Australians aged 65–75 years, and 95% of those aged 75 years and over, had a concession card in 2004–2005 [11].
The NVAF study cohort comprised all people aged 65-89 years admitted to a public or private hospital in WA from 1 July 2003 to 31 Dec 2008, with a principal or secondary diagnosis of atrial fibrillation/atrial flutter identified by the International Classification of Diseases (ICD) 10th revision Australian Modification (ICD-10-AM) code I48. Patients with comorbid cardiac valve disease, or with a prosthetic valve, were excluded, as were those undergoing long-term renal dialysis. Cohort entry was the first admission in which AF was recorded during the study period (the index admission). NVAF patients with an additional clinical indication for short (weeks) or longer term (12 months) OAC, i.e. joint replacement or for venous thromboembolism, were not excluded as the major aim is to assess long-term persistence/adherence to OAC in patients with a strong clinical indication (AF and high CHA2DS2-VASc score) and no contraindication, or reason for discontinuation such as major bleeding.
Linked data available for the AF cohort were all hospital admissions from 1980 to end of 2013, deaths (and cause of death) to end of 2013, and PBS medication records for the period 1 July 2002 to 30 June 2011. There was a minimum 12 months of PBS records before and after the index admission.
As observational cohort studies of therapeutics are at risk of immortal person-time bias [12], we used a landmark analysis method on patients alive at one year post-index admission (1-year landmark date).
Measure of warfarin exposure
We used the standard dispensing (supply) of 50 tablets, of any strength of warfarin, on at least one occasion in a one-year period as indicating exposure to warfarin during that period. Warfarin use at the landmark time point was identified according to supply in both the year prior to the index admission, and in the year after hospital discharge to the 1-year landmark. Warfarin exposure was thereby categorised as ‘persistent’ for patients with supply in both one-year periods, ‘discontinued’ for those with supply prior to index but not in the one year after, ‘initiated’ for those with no supply before index but with supply in the one year after, and ‘no warfarin’ if no supply in either period.
Age at the landmark date was grouped as 65-74, 75-79 and ≥80 years, approximating the cohort tertiles. AF at index admission was classified as either a ‘principal’ or a ‘secondary diagnosis’.
Comorbidities (heart failure, diabetes mellitus, hypertension, stroke/transient ischaemic attack/thromboembolism and vascular disease) identified from administrative hospital records in the prior 10-years were used to calculate the CHA2DS2-VASc risk score [13] at the 1-year landmark. A history of major bleeding in the principal diagnosis was identified, based on standardised bleeding definitions previously published [14,15], including intracranial haemorrhage (ICH) which incorporates intracerebral bleeding, subarachnoid haemorrhage, subdural and epidural bleeding, gastro-intestinal (GI) bleeding, and anaemia. Chronic kidney disease (CKD) was also identified.
Three outcomes were identified: time to death from any cause (censored at 3 years); time to a first stroke/TE (fatal or non-fatal) (censored at non-stroke death or 3 years); and time to a first serious bleeding episode requiring hospital admission, including fatal and non-fatal ICH (censored at death or 3 years). Outcome events based on hospital admissions were restricted to principal diagnosis only. The person-time incidence rate of stroke/TE and bleeding per 100 years (/100 PY) were calculated for each year from the landmark date.
The composite endpoint of stroke/TE was defined as ICD-10-AM codes I63 (ischaemic stroke), I64 (stroke, not specified as ischaemic or haemorrhagic) and I74 (arterial embolism and thrombosis) to identify fatal and non-fatal events. Combining I63 and I64 is recommended for identifying ischaemic stroke from electronic records for epidemiological studies [16], and is used in other population studies [17]. However, as nearly 90% of strokes as the ‘cause of death’ were coded as I64, a sensitivity analysis was done to determine the effect of excluding unspecified fatal and non-fatal stroke. All ICD codes are listed in Supplementary [Table 1].
Patient characteristics across warfarin exposure groups are described and compared using chi-square tests for categorical variables and ANOVA for quantitative variables. The annual sum, median, and interquartile range (IQR) of warfarin supplied (in milligrams, mg) were calculated.
Kaplan-Meier survival analysis was used to assess the associations between the outcomes and each categorical covariate, and the log-rank test used as a measure of their association with outcomes. Multivariable Cox regression models were used to compare outcomes across warfarin groups, adjusted for CHA2DS2-VASc score and other covariates (see [Table 1]).
A 2-sided p<0.05 was considered statistically significant. Estimated hazard ratios with a 95% confidence interval that does not include the value 1.0 are significant at the 5% level. SPSS Statistics for Windows (IBM Version 22.0. Armonk, NY) was used for all analyses.
The study was approved by the Human Research Ethics Committee (HREC) of the Department of Health (Western Australian 2014/11 and Federal Government) and the University of Western Australia (RA/4/1/8065), in addition to HREC approvals from all participating hospitals.
The datasets for this study, generated by the Data Linkage Branch of the Health Department of Western Australia are held at the University of Western Australia. The data are not publicly available due to confidentiality agreements between the providers and the study investigators.
Table 1. Characteristics of the NVAF study cohort and one-year survivors, stratified by warfarin use at the 1-year landmark
| At Index Admission |
Alive at One-year Landmark
Total and by warfarin use
|
|
All
17, 336 n (%)
|
Total
14 634 (84.4)
|
No warfarin
8 406 (57.4)
|
Discontinued
378 (2.6)
|
Initiated
3 009 (20.6)
|
Persistent
2 841 (19.4)
|
‘p’ value * |
| Women n (%) |
8 290 (47.8) |
7 077 (48.4) |
4 255 (50.6) |
179 (47.4) |
1 457 (48.4) |
1 186 (41.7) |
<0.001 |
| Age (years) - mean [SD] |
77.9 [6.6] |
78.4 [6.5] |
78.6 [6.8] |
79.2 [6.4] |
78.1 [6.3] |
78.0 [6.2] |
<0.001 |
| AF - principal diagnosis |
|
4 452 (30.4) |
2 075 (24.7) |
99 (26.2) |
1 110 (36.9) |
1 168 (41.4) |
<0.001 |
| CHA2DS2-VASc score at index admission Score at the 1-year landmark |
| Mean [SD] |
3.7 [1.5] |
4.0 [1.6] |
3.9 [1.7] |
4.3 [1.8] |
4.1 [1.7] |
4.0 [1.7] |
<0.001 |
| 1 n (%) |
1 108 (6.4) |
819 (5.6) |
483 (5.7) |
21 (5.6) |
135 (4.5) |
180 (6.3) |
|
| 2 |
2 837 (16.4) |
2 181 (14.9) |
1 340 (15.9) |
44 (11.6) |
378 (12.6) |
419 (14.7) |
|
| 3 |
4 088 (23.6) |
3 180 (21.7) |
1 853 (22.0) |
75 (19.8) |
628 (20.9) |
624 (22.0) |
|
| 4 |
3 962 (22.9) |
3 138 (21.4) |
1 813 (21.6) |
63 (16.7) |
661 (22.0) |
601 (21.2) |
|
| 5 |
3 031 (17.5) |
2 568 (17.5) |
1 441 (17.1) |
73 (19.3) |
571 (19.0) |
483 (17.0) |
|
| 6 |
1 641 (9.5) |
1 603 (11.0) |
849 (10.1) |
50 (13.2) |
397 (13.2) |
307 (10.8) |
|
| 7-9 |
669 (3.9) |
1 145 (7.8) |
627 (7.5) |
52 (13.8) |
239 (7.9) |
227 (8.0) |
|
| Components of CHA2DS2-VASc score at the 1-year landmark |
| Heart failure |
|
3 948 (27.0) |
2 095 (24.9) |
125 (33.1) |
893 (29.7) |
835 (29.4) |
<0.001 |
| Hypertension |
|
8 458 (57.8) |
4 742 (56.4) |
232 (61.3) |
1 843 (61.3) |
1 641 (57.8) |
<0.001 |
| Diabetes |
|
3 107 (21.2) |
1 742 (20.7) |
116 (30.7) |
596 (19.8) |
653 (23.0) |
<0.001 |
| Vascular disease |
|
6 415 (43.8) |
3 731 (44.4) |
172 (45.5) |
1 288 (42.8) |
1 224 (43.1) |
NS |
| Stroke/TIA/TE |
|
2 337 (16.0) |
1 107 (13.2) |
80 (21.2) |
668 (22.2) |
482 (17.0) |
<0.001 |
| Age 75 year or more |
|
9 867 (67.4) |
5 702 (67.9) |
274 (72.5) |
1 998 (66.4) |
1 893 (66.6) |
NS |
| History (10 years) |
| Chronic kidney disease |
1 226 (7.1) |
1 109 (7.6) |
692 (8.2) |
46 (12.2) |
187 (6.2) |
184 (6.5) |
<0.001 |
| Bleeding |
2 042 (11.8) |
1 961 (13.4) |
1 149 (13.7) |
108 (28.6) |
369 (12.3) |
335 (11.8) |
<0.001 |
SD=standard deviation, TIA=transient ischaemic attack, TE=thromboembolism * ‘p’ value for difference between the four warfarin use groups
There were 17,336 index NVAF admissions (27.5% as principal diagnosis). For patients with AF as a secondary diagnosis the most frequent principal diagnoses were IHD (13.2%) and HF (6.6%); stroke/TE was 4.4%. Other frequent conditions, pneumonia, chronic obstructive lung disease and osteoarthritis of the knee and hip were each <5%. Patients with AF as the principal diagnosis were younger (76.2, SD 6.5 vs 78.5, SD 6.5 years, p<0.001) and had significantly less comorbid diabetes, HF, IHD, CKD, or prior stroke.
At one-year post-index admission 14,634 patients (84.4%) were alive. Compared to survivors, those who died within the first year were older (80.5, SD 6.1 vs 77.4, SD 6.5 years, p<0.001) and had a higher mean CHA2DS2-VASc score (4.2 vs 3.6, p<0.001) at index admission. The most frequent cause of death was ‘any vascular disease’ (37.6%) including IHD (19.1%), ischaemic stroke (8.3%) and AF (2.8%); cancer being the next most frequent (32.4%).
Patient characteristics at index admission, at the one-year landmark, and by warfarin exposure at the landmark date are presented in [Table 1]. Warfarin use at the 1-year landmark was lower for women than men. Those with a history of CKD or bleeding prior to the index admission were less likely to use warfarin, and to discontinue after admission [Table 1]. As expected, those admitted for bleeding at the index admission, or prior to the 1-year landmark, were less likely to initiate warfarin, and more likely to discontinue its use. Initiation was higher among those suffering stroke/TE at index or prior to the landmark.
Warfarin use
For those alive at the 1-year landmark, 40% were supplied with warfarin either prior to, or after, the index admission [Table 1]. Warfarin exposure exceeded 45% only for those with a CHA2DS2-VASc score ≥6, with those with a score of ‘2’ being the lowest at 38.6%.
The median total of warfarin dispensed in the 12 months pre-index was 700 mg (400-1150) for those who discontinued from the index admission and 900 mg (500-1450) for those persisting post-hospital discharge (data not shown). The totals in the year after discharge were 1150 mg (650-1650) for those initiating post-index, and 1150 mg (750-1650) for those persisting. Three patients supplied with fewer than 50 tablets (14-17 tablets) were excluded from comparisons.
Stroke/SE was the most frequent principal diagnosis at the index admission associated with a change in warfarin use. Among 30-day survivors of stroke (n=689) warfarin was initiated in 302 patients (43.8%), but not for a further 300 (43.5%). For all patients alive at the 1-year landmark initiation was higher for those CHA2DS2-VASc scores ≥3, while persistent use was around 20% across the whole range of scores.
Of the 14,634 alive at the one-year landmark 1,384 (9.5%) died in the following year; crude all-cause mortality was 9.0%, and 8.7% in the subsequent years.
Among the 3,631 deaths at three years from the one-year landmark date, the cause was coded as ‘vascular disease’ for 1,519 patients (41.8%) which included IHD (29.4%), ischaemic stroke (6.2%), and ICH (1.5%). Cancer deaths were 25%.
Unadjusted survival was greater among patients persisting with, or initiating, warfarin prior to the landmark date compared with those not exposed to warfarin, and poorer for those who had discontinued (Log Rank 83.35, df 3, p<0.001) [Figure 1]. Annualised survival, overall and according to warfarin exposure, is shown in [Table 2].
Figure 1. Kaplan-Meier survival to three years from the 1-year landmark after admission for AF (principal or secondary diagnosis) by warfarin use at the landmark date
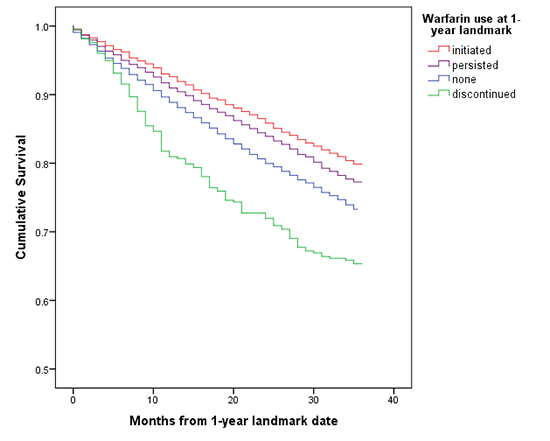
Table 2. Annual cumulative survival and incidence of stroke/systemic thromboembolism and serious bleeding events per 100 person–years from the 1-year landmark, overall and by warfarin use.
| Year |
Overall |
No warfarin |
Discontinued |
Initiated |
Persisted |
| Number of patients surviving
Kaplan-Meier probability of unadjusted cumulative survival to 3 years |
| 1 |
13 247
0.90
|
7 534
0.90
|
309
0.82
|
2 786
0.93
|
2 606
0.92
|
| 2 |
12 052
0.82
|
6 776
0.81
|
279
0.72
|
2 602
0.86
|
2 399
0.84
|
| 3 |
11 003
0.75
|
6 159
0.73
|
247
0.65
|
2 402
0.80
|
2 195
0.77
|
| Number of stroke/systemic thromboembolism events (person-years observed)
Incidence rate per 100 person-years (95% CI) |
| 1 |
293 (13 937) 2.1 (1.8-2.4) |
187 (7 956) 2.4 |
9 (349)
2.6
|
42 (2 905)
1.4
|
55 (2 723)
2.0
|
| 2 |
199 (12 340) 1.6 (1.3-1.9) |
106 (7 148) 1.5 |
9 (290)
3.1
|
52 (2 698)
1.9
|
32 (2 500)
1.3
|
| 3 |
200 (11 525) 1.7 (1.4-2.1) |
114 (6 472) 1.8 |
6 (257)
2.3
|
46 (2 497)
1.8
|
34 (2 295)
1.5
|
| Total |
692 (37 802)
1.8 (1.7-1.9)
|
407 (21 576)
1.9 (1.7-2.1)
|
24 (896)
2.7 (-1.7-7.1)
|
140 (8 100)
1.7 (1.2-2.2)
|
121 (7 518)
1.6 (1.1-2.1)
|
| Number of serious bleeding events (person-years observed)
Incidence rate per 100 person-years (95% CI) |
| 1 |
234 (13 847) 1.7 (1.4-2.0) |
110 (7 918) 1.4 |
4 (348)
1.1
|
63 (2 878)
2.2
|
57 (2 700)
2.1
|
| 2 |
200 (12 554) 1.6 (1.3-1.9) |
105 (7 105) 1.5 |
7 (288)
2.4
|
45 (2 678)
1.7
|
43 (2 481)
1.7
|
| 3 |
174 (10 886) 1.5 (1.2-2.0) |
80 (6 181)
1.2
|
3 (244)
1.2
|
46 (2 313)
1.8
|
45 (2 149)
2.0
|
| Total |
608 (37 287)
1.6 (1.5-1.7)
|
295 (21 204)
1.4 (1.2-1.6)
|
14 (880)
1.6 (-2.9-6.1)
|
154 (7 869)
2.0 (1.4-2.5)
|
145 (7 330)
2.0 (1.4-2.5)
|
Multivariate associations with survival to three years from the one-year landmark
Warfarin exposure group, a CHA2DS2-VASc score ≥3, age, male sex, comorbidity and previous events were all independently associated with 3-year all-cause mortality in 1-year survivors of AF [Table 3].
Table 3. Independent predictors of 3-year all-cause mortality among 14, 631 survivors with NVAF at the 1-year landmark
| Factor |
Hazard ratio (95% CI) |
P value |
| Warfarin use vs none
Discontinued
Initiated
Persisted
|
1.22 (1.02-1.45)
0.74 (0.68-0.82)
0.87 (0.80-0.95)
|
0.03
<0.001
<0.01
|
| CHA2DS2_vasc score vs 1
2
3
4
5
6
7-9
|
1.14 (0.88-1.50)
1.49 (1.15-1.94)
1.73 (1.33-2.25)
2.02 (1.55-2.63)
2.48 (1.89-3.26)
3.07 (2.32-4.04)
|
NS
<0.01
<0.001
<0.001
<0.001
<0.001
|
| AF- principal vs secondary diagnosis |
0.69 (0.64-0.76) |
<0.001 |
| History bleeding |
1.28 (1.18-1.40) |
<0.001 |
| History of CKD |
1.39 (1.25-1.54) |
<0.001 |
| Sex (female) |
0.69 (0.65-0.74) |
<0.001 |
| Age vs <75 years
75 -79
80 years or more
|
1.48 (1.31-1.66)
2.81 (1.25-3.12)
|
<0.001
<0.001
|
CKD=chronic kidney disease
Stroke/TE was the principal diagnosis at the index admission for 727 patients (4.2%) among whom 38 (5.2%) died within 30-days. There were an additional 294 fatal and non-fatal strokes prior to the 1-year landmark.
There were 694 new stroke/TE events in the 3-year follow-up post-landmark date, of which 224 (32.3%) were ischaemic stroke deaths, and 199 (89%) coded as I64. The incidence rate of stroke/TE events by warfarin exposure is shown in [Table 2].
Univariate associations with stroke/TE
Survival to stroke/TE was poorer for those who discontinued warfarin, compared with those not exposed, initiating or persisting, but the difference was not statistically significant (Log Rank 6.17, df 3, p=0.10) [Figure 2]. Women, those with higher CHA2DS2-VASc scores, aged ≥80 years, with a history of bleeding or CKD, and with AF as a secondary diagnosis were at higher risk for stroke/TE.
Multivariate associations with stroke/TE
Figure 2. Kaplan-Meier time to a first fatal or non-fatal stroke/systemic thromboembolism in the 3-year follow-up from the landmark date by warfarin use at landmark
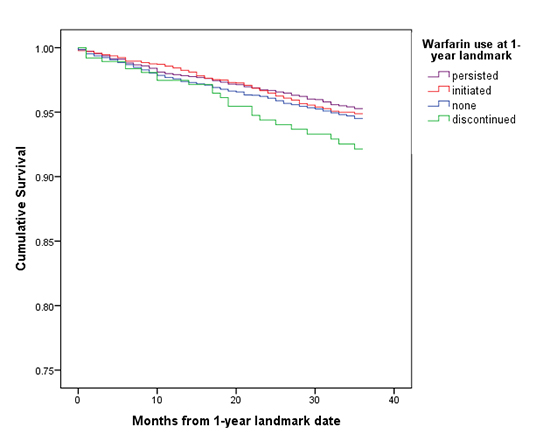
CHA2DS2-VASc scores ≥5 were independently associated with the risk for stroke/TE, with the adjusted hazard more than doubling [Table 4]. In a sensitivity analysis the associations with the outcome were unchanged by exclusion of 281 events coded as ‘unspecified’ strokes.
Table 4. Independent predictors of a first fatal or non-fatal stroke/systemic thromboembolism event in the 3-year follow-up for one-year survivors with NVAF
| Factor |
Hazard ratio (95% CI) |
P value |
| Warfarin use vs none
Discontinued
Initiated
Persisted
|
1.22 (0.81-1.85)
0.89 (0.74-1.09)
0.87 (0.71-1.07)
|
0.34
0.26
0.19
|
| CHA2DS2_vasc score vs 1
2
3
4
5
6
7-9
|
0.87 (0.48-1.58)
1.27 (0.71-2.25)
1.37 (0.77-2.45)
2.02 (1.13-3.62)
2.32 (1.28-4.23)
3.96 (2.17-7.23)
|
0.65
0.42
0.28
0.02
<0.01
<0.001
|
| AF -principal vs secondary diagnosis |
0.93 (0.78-1.12) |
0.45 |
| History bleeding |
1.15 (0.94-1.24) |
0.18 |
| History of CKD |
0.98 (0.75-1.28) |
0.88 |
| Sex |
1.0 (0.85-1.17) |
0.96 |
| Age vs <75 years
75-79
80 or more years
|
1.57 (1.21-2.03)
2.22 (1.74-2.81)
|
<0.01
<0.001
|
There were 2,042 patients (11.8%) with an admission for major bleeding in the 10 years prior to the index admission. Of the 249 patients with a principal diagnosis of bleeding at index admission, the majority were neurological events coded as ICH (n=74, 29.7%), 12 (4.8%) were sub-arachnoid and 33 (13.3%) epidural haemorrhages. A further 88 (35.3%) admissions were for gastro-intestinal bleeding, and 19 (7.6%) had respiratory tract bleeding.
There were 13 deaths (5.2%) within 30 days of admission, and an additional 48 deaths (20.3%) among 236 survivors of a serious bleed within the first year. There were 35 new bleeding events prior to the 1-year landmark.
Of those alive at the landmark date, 608 were hospitalised with a first or new major bleed within three years. The majority were gastrointestinal bleeds (n=410, 67.4%), with 124 ICH 124 (20.4%) and 61 coded as epidural haemorrhages (10%). Of the 22 deaths coded as intracerebral haemorrhages, 21 occurred in hospital. The incidence rate of bleeding events by warfarin exposure is shown in [Table 2].
Univariate associations with major bleeding
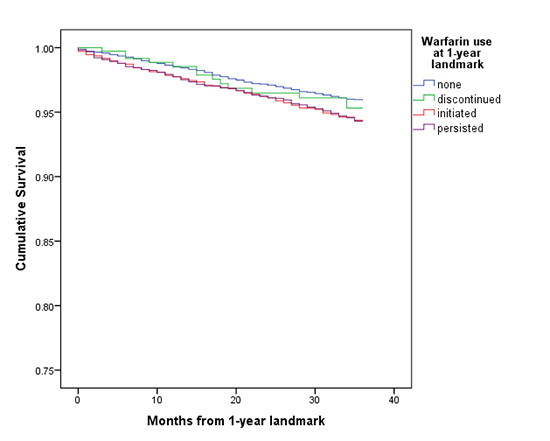
The risk for bleeding in the 3-year follow-up was significantly greater for men, those aged ≥80 years, with a prior bleeding event, and with a CHA2DS2-VASc score ≥4. Initiation of and persistence with warfarin were also associated with increased risk (Log Rank 18.01, df 3, p<0.001) [Figure 3].
Figure 3. Kaplan-Meier time to admission for major bleeding within three years of the 1-year landmark date by warfarin use
Multivariate associations with major bleeding
After adjustment, the independent risk for a serious bleeding event was higher for males, those aged ≥80 years, or with a history of bleeding, and for those both initiating and persisting with warfarin use [Table 5].
Table 5. Independent predictors of a first admission for major bleeding in the 3-year follow-up among 1-year survivors with NVAF
| Factor |
Hazard ratio (95% CI) |
P value |
| Warfarin use vs none
Discontinued
Initiated
Persisted
|
1.00 (0.458-1.72)
1.39 (1.14-1.17)
1.42 (1.16-1.74)
|
1.00
<0.01
<0.01
|
| CHA2DS2_vasc score vs 1
2
3
4
5
6
7-9
|
1.32 (0.79-2.20)
1.78 (1.09-2.92)
2.06 (1.25-3.39)
2.27 (1.36-3.78)
1.95 (1.12-3.38)
2.82 (1.61-4.94)
|
0.28
0.02
<0.01
<0.01
0.02
<0.01
|
| AF-principal vs secondary diagnosis |
1.02 (0.85-1.22) |
0.83 |
| History bleeding |
1.65 (1.35-2.02) |
<0.001 |
| History of CKD |
1.12 (0.84-1.50) |
0.42 |
| Sex (female) |
0.72 (0.60-0.85) |
<0.01 |
| Age vs <75 years
75-79
80 or more years
|
0.89 (0.70-1.13)
1.35 (1.10-1.66)
|
0.34
<0.01
|
* Diagnoses at discharge from index admission
This study has provided a real-world indication of outcomes from exposure to warfarin in an older population, with new or comorbid AF diagnosis identified in a hospital admission. Current warfarin use one year after the index admission was independently associated with lower risk for all-cause mortality to three years, compared with non-exposure, and with increased risk for those discontinuing warfarin. The reduction in mortality for those exposed was not matched by a statistically significant reduction in the risk of stroke/TE. The hazard ratios, while lower than for non-users, were not statistically significant, and neither was the apparent increased hazard for those discontinuing warfarin. The initiation or ongoing exposure to warfarin was independently associated with increased risk for serious bleeding, compared with non-use.
Other factors may be responsible for the different risk for death and stroke for those exposed to warfarin. The selection for warfarin treatment of ‘healthy users’, with less life-limiting comorbidity such as renal failure, may have contributed to the mortality benefit. In addition, the rate of stroke/TE events was low in the unexposed and exposed groups (less than 2.0/100 PY, not including those discontinuing). The lack of statistical significance for stroke/TE risk may be due to insufficient power from the low number of stroke events. Other explanations include less than optimal management of warfarin leading to reduction in benefit, and inadequate measurement of exposure. Patients may have changed their status during follow-up, initiating or discontinuing warfarin during this time.
The low stroke/TE rate, although not age-standardised, was consistent with rates reported for Australia, Europe and other developed economies [18,19,20], but resulted in too few events for reliable estimates of rates within levels of the CHA2DS2-VASc risk score. For patients not exposed to warfarin, the overall incidence rate was lower than reported from a large study of patients in England (3.8/100 PY), with data from both primary and secondary care, while the rate for those exposed was the same (1.7/100 PY) [21]. In that population a net clinical benefit in stroke reduction from exposure to warfarin, defined using similar criteria as ours, was seen for CHA2DS2-VASc score ≥2 for men and ≥3 for women. The low stroke/TE rate among unexposed patients in our cohort may be related to the inclusion of both incident and prevalent cases. In addition, the use of antiplatelet medication in the unexposed group was not known, though nearly half had comorbid vascular disease. Major bleeding among those exposed to warfarin did not exceed the pooled estimate of 2.51/100 PY from the warfarin arms of 51 studies [22].
Current warfarin use never exceeded 40% overall in our cohort of older patients. Under 2012 European and US guidelines, none of our cohort patients were ‘low risk’; all having CHA2DS2-VASc score scores for which oral anti-coagulation would be considered or recommended (men ≥1, women ≥2), unless contraindicated [8,19] and this recommendation remains current [7]. While over 13% had a history of bleeding in the 10 years prior to the 1-year landmark date, use in others would be absolutely or relatively contraindicated. We did not have the clinical data to assess the proportion of patients for whom warfarin may have been contraindicated due to bleeding risk (as estimated by an algorithm such as the HAS-BLED score). We had insufficient clinical data to estimate bleeding risk. In addition we could not identify those with cognitive impairment or frailty; groups of patients who are less likely to be prescribed OAC, despite being at higher predicted risk for stroke and death. [23]
While variation in the selection of patients for warfarin is widespread, with reported contraindications ranging from under 20% to over 50% [24], the low exposure to warfarin in our cohort of both prevalent and incident AF is consistent with other real-world studies. These have reported initial warfarin use below 60% overall, and below 70% among moderate/high risk patients [25,26]. Furthermore, there is considerable drop-off within a few years of starting, with rates in Australia and elsewhere falling below 30% [27,28].
Until/unless treatments to successfully control AF are developed OAC, including warfarin, remain central to AF management. Ongoing research into early detection of AF, strategies to promote appropriate use of, and persistence with, OAC and the outcomes of these strategies is necessary [29].
Strengths and limitations
This use of linked state-wide morbidity and mortality data and the national pharmaceutical database, allowed a large-scale population-level study with reliable and complete outcome data. Good ascertainment of stroke/TE and serious bleeding events is probable as most cases would require hospital admission. While clinical detail is reduced when using administrative data, it is sufficient for the calculation of the CHA2DS2-VASc score [30], an important predictor of stroke risk [15].
The externally coded cause of death uses coding conventions which may attribute death to underlying (antecedent or contributing) conditions or to the immediate ‘cause’. The attribution of stroke as cause of death out of hospital to ICD-10-AM I64 (not specified as haemorrhage or infarction) is a worldwide limitation for studies of stroke [31,32,33].
As the cohort was identified from hospital admissions, the patients may not be representative of the wider population with AF. They are likely to have poorer health and suffer more comorbidity. The proportion of patients with comorbid cardiovascular disease exceeded 40%. We could not quantify the use of anti-platelets (including aspirin) in these patients, a factor in apparent ‘under-use’ of OAC [34]. Use of antiplatelet and OAC drugs among those not in the cohort (not hospitalised for any reason during the study period) may well have differed from those studied.
Exposure to warfarin is difficult to quantify with accuracy from pharmacy data alone, as dose may vary with age, sex and comorbidity [35]. Regimens such as different dosing on alternate days, and varying strength of tablets, make calculation of measures such as a ‘defined daily dose’ impractical. Without INR data, more reliable measures such as ‘time within the therapeutic range’ cannot be assessed [36].
Access to other clinical databases, such as laboratory results, will further strengthen large-scale cohort studies using linked data, with the potential to provide detailed information about the changing use of oral anticoagulants and the resulting outcomes in AF and other thromboembolic conditions.
We thank the following institutions for providing the data used in this study. The Australian Department of Health for the cross-jurisdictional linked PBS data. Staff at the WA Data Linkage Branch and data custodians of the WA Department of Health Inpatient Data Collections and Registrar General for access to and provision of the State linked data. The Victorian Department of Justice and Regulation for the cause of death data held in the National Coronial Information System.
In this real-world cohort of older patients hospitalised with newly diagnosed or comorbid AF, the use of warfarin in a period predating the widespread availability of NOACs was lower than recommended in treatment guidelines. Initiation and persistent use of warfarin was associated with a lower mortality risk, with an apparent reduction in the risk of stroke/TE which did not reach statistical significance. The probable under-use of warfarin presents the opportunity for further reduction in stroke/TE, facilitated by the uptake of NOACs among those not prescribed, or not persistent with, warfarin.






