Atrial fibrillation, a progressively rising global health problem, is also rising in Hemophiliacs due to an increase in life expectancy in them. While treating Hemophiliacs with AF, deciding eligibility, choosing the anticoagulant based on risk-benefit ratio are tough decisions for physicians to make. This review paper aims to explore and compare existing studies, reviews and consensus papers to assess the safety of different Novel Oral Anticoagulants (NOACS) in this population.
Thorough literature search was conducted on Pubmed using Atrial Fibrillation, Hemophilia A, Oral anticoagulants, stroke prevention, Dabigatran, factor Xa inhibitors as keywords separately and in combinations. Papers in English language only from the past 5 years were selected for review. After removing duplicate results, 80 papers were selected and after applying different exclusion criteria and according to relevance, 40 papers were finalized for review.
The keywords AF, Stroke prevention, oral anticoagulants, Hemophilia a, Factor Xa inhibitors and Dabigatran gave 24899, 13619, 8964, 3503, 2850, 2799 results, respectively. Combination keywords also showed some papers and out of short-listed 80 relevant papers 35 were finalized. Reviewing and analyzing these papers revealed no clinical trials in hemophiliacs with AF in the past 5 years and 5 clinical trials comparing NOACs with Warfarin in general population. Rest were systematic reviews, consensus papers and meta-analyses on management in this group. A few compared these drugs for AF in the general population but not specifically in Hemophiliacs and others. consensus papers developed suggestions for management and showed that NOACs are superior to Warfarin but need individual evaluation in Hemophiliacs with AF.
Patients with Hemophilia can also have thrombo-embolism despite their bleeding tendency and NOACs are a better option in them because of less need for monitoring, no food interactions and fewer drug interactions. This comparative review emphasized the need for more work to develop proper guidelines for thrombo-prophylaxis management in this specific group.
Global prevalence of Atrial Fibrillation (AF) was estimated to be 33.5 million in 2010 making up 0.5 % of the world population and is constantly rising [1]. In the United States, the estimates are around 2.7 to 6.1 million and are expected to rise to 12.1 million by 2030 [2] and in Europe, the expected rise is 17.9 million by 2060 [3]. AF is more common in adults more than 65 years of age but can occur in young patients as well. In the US 9% of people older than 65 have AF and 2% of people less than 65 are affected by it [4]. Such prevalence rate and the need for long term management of stroke and the complications related to it pose a huge burden on the healthcare system. United States spends approximately 26 billion dollars annually on managing AF and its related complications [2,4] and has approximately 750,000 hospitalizations each year and estimated mortality of 130,000 deaths per year [5].
AF is one the most commonly diagnosed and persistent arrhythmia globally which predisposes patients to unexpected, sudden and often fatal thrombo-embolic neurological events, increasing the risk of ischemic stroke 5-fold [6]. Preventing these complications is important to decrease the overall disease burden and so anticoagulants are considered after risk stratification through CHADS 2 scoring [7]. Oral anticoagulants also have a risk of unexpected bleeding including severe episodes [8]. Warfarin, a Vit. K antagonist, remained the gold standard anticoagulant to prevent embolic stroke [9] but needed strict monitoring of INR to keep it in the therapeutic range (2-3) and failed to do so may lead to increased bleeding risk [9]. Dabigatran, a direct thrombin inhibitor was the first direct oral anticoagulant which needed less monitoring as compared to Warfarin. Later newer anticoagulants factor Xa inhibitors were added which also needed less monitoring as compared to Warfarin.
Several trials compared the efficacy and the safety of the new oral anticoagulants with Warfarin and proved the newer drugs to be as effective as Warfarin and superior in decreasing the intracranial bleeding episodes and needing less frequent monitoring [10]. Non-K inhibitor anti-coagulants are being compared against each other for efficacy and safety to prevent complications in AF and not much data is available about challenging scenario about the choice of an anticoagulant when the patient has a predisposition to bleeding because of hereditary and acquired bleeding disorders yet needing anticoagulation based on CHADS 2 scoring. Attaining a balance in anticoagulation and bleeding episodes is a tough target and hence safety profile of the anticoagulants is important in order to prevent the patient from an ischemic stroke while avoiding hemorrhagic stroke and other major bleeding episodes. Hemophilia A is one such hereditary condition having limited information about safety of newer anticoagulants. It is an X-linked recessive condition with low levels of clotting factor VIII predisposing a person to excessive bleeding [11]. Owing to recent advances like CFC (Coagulation Factor Concentrates), life expectancy is increased but so are the complications which arise as a person ages like AF. The prevalence of AF was found to be as high as 0.84% in a cross-sectional survey from 14 Hemophilia centers in Europe [12].This value is similar to the prevalence of AF in general population [13] and increases with increasing age as it does in general population with 0.2 % in less than 60 years old hemophilia patients and reaches up to 3.4% in hemophiliacs more than 60 years of age [12].
Comparison of efficacy and safety profile of these two groups of non-Vit K anticoagulants can help in the better assessment of the scenario and in deciding the anticoagulant to be used in patients with bleeding tendencies without disturbing the delicate balance between preventing ischemic stroke and a chance of causing hemorrhagic stroke. Dabigatran had been in use already in hemophiliacs with AF, considering antidote was available and now with FDA approving the antidote for Riavroxaban, this provides clinicians with more options of anticoagulants and this review article aims to assess their safety in the scenario.
Research was conducted to identify studies analyzing and assessing safety profile of newer anticoagulants in setting of AF with inherited bleeding disorders, specifically Hemophilia. PubMed was used as our main database to find the relevant articles. Keywords which were used for the search were Atrial fibrillation, Oral anticoagulants, Hemophilia A, Stroke prevention, Dabigatran, and factor Xa inhibitors. MeSH keywords Atrial fibrillation, Hemophilia and Dabigatran were also used for search.
Atrial fibrillation yielded 10146 research articles, Using the keyword Hemophilia A yielded 2850 research papers, Oral anticoagulants yielded research papers and Factor Xa inhibitors yielded total number of 3503. A combination of keywords Atrial fibrillation and Oral anticoagulants gave a total of 3953 research papers, Atrial fibrillation and stroke prevention yielded 3847 papers, Atrial fibrillation and Hemophilia a yielded 17 research papers. Atrial fibrillation, anti coagulation and Hemophilia a gave 10 articles and Stroke prevention with Hemophilia a gave 4 research papers. Out of these results a total of 80 articles relevant to the research question were selected. After applying inclusion and exclusion criteria, duplicate papers were removed and finally a total of 35 articles were selected for review. A few relevant research papers about mechanism of actions, published before past 5 years from references of selected papers were also included.
Inclusion/Exclusion criteria
Peer-reviewed, full-text research papers from past 5 years were included in the review. All selected articles were in English language and no global or geographical considerations were given. Any non peer- reviewed and duplicate papers were excluded from finally selected articles.
Both Intrinsic and extrinsic pathways of normal coagulation cascade involve a number of different clotting factors and have different triggers to get activated but later converge and have a common pathway. Intrinsic pathway is triggered by direct damage to the blood vessels and activates a series of coagulation factors whereas extrinsic is triggered by damage to the tissue which in turn activates Factor VII. Both pathways converge at a point where Factor X is activated which leads to the formation of Thrombin or activated Factor II and at the end fibrinogen is converted to fibrin. Certain co-factors are mandatory for the process to complete like Vit. K, Ca++, etc. Deficiency in some of these factors may be the cause of different inherited bleeding disorders making the person more prone to the bleeding episodes, and some risk factors may increase the chances of thrombo-embolism and may have serious consequences of its own therefore needing prophylaxis with anticoagulants. When these both conditions co-exist using anticoagulation needs more vigilant and conscious approach.
Mechanism of action and pharmacological properties of oral anticoagulants
Warfarin had been the main oral anticoagulant for around 50 years since 1945 and had been effective. It acts as Vit K inhibitor, so inhibits all the steps which are catalyzed by Vit. K. While using Warfarin it was very important to keep in mind the delicate balance which had to be maintained to avoid any bleeding episodes for which purpose INR monitoring was necessary and needed to be in between 2-3. INR can easily be affected by dietary and drug interactions so needed frequent monitoring. Dabigatran was introduced long after Warfarin in 2010 and has a different mechanism of action. It acted at the later stage of the coagulation cascade, as a thrombin inhibitor as shown in [Figure 2], so it affected both intrinsic and extrinsic pathway. It had an advantage of less need for monitoring of INR as compared to Warfarin. It was first among the NOAC's, the latest oral anticoagulants added to treat pro-thrombotic conditions are Factor Xa inhibitors inhibiting the activated Factor Xa both in free form and attached to the pro-thrombin complex. Considering its important site of action in the coagulation cascade it also affected both intrinsic and extrinsic pathways. It is a group of medications out of which frequently used drugs include Rivaroxaban, Apixaban etc. Rivaroxaban was approved in 2011. The problem remained that in case of any need of urgent or immediate reversal, they had no antidotes available, until an antidote for Dabigatran, Idarucizumab was approved and recently in 2018 an antidote for Rivaroxaban and Apixaban has been approved. Pharmacological properties of fXa inhibitors differed in many ways from earlier anti-coagulants as they targeted a specific factor instead of multiple factors and have a rapid onset of action and their bioavailability is also better in comparison to Warfarin [13]. Owing to this mechanism of action there is no effect of dietary intake on Vit.K inhibitors as it is on Warfarin and so a fixed dose is a convenience which a patient gets with them and along with these, they have fewer drug interactions [14]. Because their pharmacokinetics and pharmacodynamic properties depend on the dose given, they have a predictable response after a fixed dose is administered and so need lesser monitoring [15].
Figure 1. PRISMA FLOW diagram showing the process of selection of research papers.
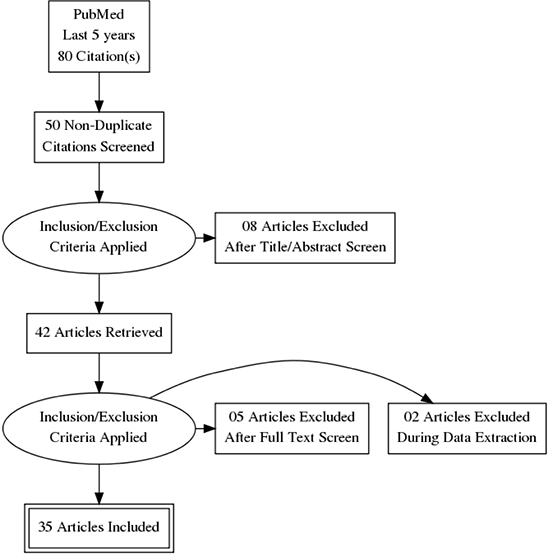
Figure 2. Site of action of Warfarin, Dabigatran and Factor Xa inhibitors.
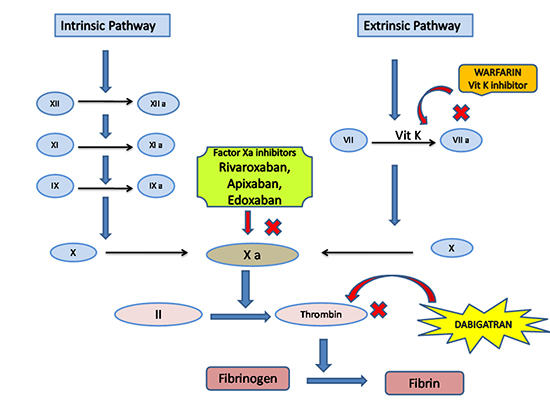
Table 3. Comparison of Pharmacological Properties of thrombin inhibitors and Factor Xa inhibitors.
| Characteristics |
Thrombin Inhibitors |
Factor Xa Inhibitors |
|
|
|
Dabigatran |
Rivaroxaban |
Apixaban |
Edoxaban |
| Mechanism of action |
Thrombin Inhibition |
Factor Xa inhibition |
Factor Xa inhibition |
Factor Xa inhibition |
| Available doses |
75 mg, 150 mg |
2.5 mg, 10 mg, 15 mg, 20 mg |
2.5 mg, 5 mg |
15 mg, 30 mg, 60 mg |
| Food Interaction |
None
|
None
To be taken with food only for higher doses
(20 mg)
|
None
|
None
|
| Route of Elimination |
Renal |
Renal and Hepatic |
Renal and Hepatic |
Renal and Hepatic |
| Bioavailability |
6.2 % |
80 % |
50 % |
62 % |
| Half –life
(Normal Renal function)
|
12-14 hrs |
5-9 hrs
Increase with old age
|
12hrs |
10-14 hrs |
| Renal impairment with AF
Mild ( >50ml/min)
Moderate
(15-50 ml/min)
Severe (<15 ml/min)
|
No dose adjustment
Reduce dose
(75 mg/day when below 30ml/min)
Avoid use
|
No dose adjustment
15 mg/day
Avoid use
|
No dose adjustment
Reduced dose
(2.5 mg/day)
Reduced dose
(2.5mg) if on dialysis
|
No dose adjustment
Reduced dose
(30 mg/day)
Avoid use
Below
|
| Hepatic Impairment
Mild
Severe
|
None
|
None
Avoid use
|
None
Not recommended
|
None
Not Recommended
|
When to start anticoagulation in Hemophiliacs with AF: Is CHADS2 VAS and HAS-BLED scoring enough?
Atrial fibrillation may cause intra-cardiac thrombus formation due to stasis and can cause thrombo-embolic stroke which may be life- threatening. Atrial fibrillation may be asymptomatic and this complication can be its first presentation, therefore screening and diagnosing it in time is important to prevent stroke. This is done by risk assessment for stroke through CHADS2 or CHADS VAS scoring and then prophylactic treatment is initiated in the form of oral anticoagulant based on the risk stratification and approved guidelines for general population. Hemophilia patients have now increased life expectancy owing to recent advances like the use of Recombinant FVIII in management but so are the conditions which are more prevalent in old age, this makes Atrial fibrillation to rise in hemophiliacs as well [16]. These patients already have a bleeding tendency and whether they need anticoagulation is an important question which is frequently encountered while managing such patients. Despite the defect in clotting in hemophiliacs they still have other risk factors to develop thrombotic cardiovascular diseases [17]. Another study evaluating the risk factors for cardiovascular diseases between hemophiliacs and non hemophiliac controls although showed that controls have slightly higher incidence but as result was not statistically significant so recommended that they should be evaluated on individual basis [18]. Even with the use of recombinant FVIII there is still a risk of thrombosis in mild and moderate hemophilia, severe cases are somewhat protected though may still have a chance of thrombo-embolism [19]. Reducing the risk of stroke in patients with Atrial fibrillation depends on attaining an optimal risk and benefit balance which means estimating the risk of developing stroke due to thrombo-embolism by CHADS 2 OR CHADS2 VAS and then estimating the risk of bleeding secondary to using oral anti-coagulant by HAS-BLED score [20]. But will the same risk-benefit assessment criteria and guidelines give an idea about anticoagulation in Hemophiliacs with AF as they have increased propensity to bleed. There are very few trials addressing anticoagulation for AF in this specific population or group of patients and currently, no proper guidelines for risk assessment and management are developed as yet and only few expert consensuses developed to address this knowledge gap are available and serve as a guide to physicians [21,16]. Since the bleeding risk is high,an approach is devised in the form of an algorithm [16].
Normally patients are stratified for risk according to CHADS2-VAS scoring and HAS-BLED or FVIII levels, and then a score of >3 or equal to 3 is used to start prophylactic anticoagulation. But no cut off value was available for Hemophiliacs with AF and so one such consensus was developed and it was suggested to be >2 or equal to 2 and the level of Factor VIII to be lowered from 30% to 20% [22], and it's recommended not to start anticoagulation if this level is below 20% [22]. However this threshold should still be evaluated according to the particular patient who is under consideration [20].
The case report and literature analysis by Murray et al focused on a female patient, a hemophilia carrier, and highlighted that every case of hemophilia with Atrial fibrillation should be evaluated individually depending on their individual risk-benefit evaluation. They emphasized that as levels of Factor VIII in females may vary with time and can change the risk-benefit balance and assessment so any hemophilia A carrier with low factor VIII levels may have a decreased risk of bleeding [20] so an individual assessment will give a better idea about when to start and what to consider for anticoagulation.
During individual assessment, the primary consideration while making a decision is the bleeding phenotype of the patient, which is whether the patient bleeds spontaneously, whether bleeding occurs due to an initiating stimulus like trauma and how severely a patient bleeds [23]. Developing inhibitory antibodies in Hemophiliac is frequently encountered complication .The hemophilia patients who don't have an inhibitor generally respond well to clotting factor replacement, thus making it easier to control or prevent severe bleeding [23]. On the other hand, patients who have inhibitors have a less predictable response. it was shown by some studies that around 10% to 20% of bleeding episodes with inhibitors were not responsive at all or responded partially to a bypassing agent [24,25]. This evaluation can serve as a guide in assessing the risk-benefit ratio of a hemophiliac patient and whether the patient needs a thrombo-prophylaxis in Atrial fibrillation or not.
Regarding whether to start thrombo-prophylaxis in hemophilia, De Koning and colleagues suggested/concluded in their literature review that approximately one third patients with non-severe hemophilia had a significantly better haemostatic potential than the patients who were on Vit K inhibitors with therapeutic INR whereas patients with severe hemophilia had equally comparable haemostatic potential to the patients with therapeutic INR, which showed that a considerable number of patients with non-severe hemophilia should be considered for thrombo-prophylaxis [26].
MAINTAINING BALANCE BETWEEN ANTICOAGULATION AND BLEEDING RISKS IN BLEEDING PRONE POPULATION/ ISCHEMIC STROKE VS HEMORRHAGIC STROKE
As the main complication of inherited bleeding disorders like Hemophilia is spontaneous or post-traumatic bleeding, they are somewhat protected from thrombosis but both arterial and venous thrombosis do occur occasionally, so they may need anticoagulation as the situation arise and also consideration is needed to start prophylactic anti-coagulants as the need can be comparable to general population like in the presence of AF [23] where the complication can be more serious. But with tendency of increased bleeding and taking oral anti-coagulant can have their own risk of bleeding if INR fluctuates or if medication is affected by dietary intakes or drug-drug interactions as was the case in Warfarin where regular monitoring was needed, but with the new direct oral anticoagulants, there is an increased safety profile, as proven by many studies especially considering intra-cerebral hemorrhage [27].
In general population, all DOACS were considered safer than Warfarin and as effective as it is but there isn't much evidence as not many trials have been done specifically in hemophiliacs so a literature review and review of different consensus done earlier can help us in analyzing and comparing the effectiveness and safety of DOACS in hemophiliacs. Although Rivaroxaban and Apixaban are proven to be superior and safer to Warfarin in patients with AF, they still do have a chance of increased bleeding as in all anti-coagulants [28]. It was suggested that instead of using Warfarin, it will be safer in order to prevent a major bleeding episode by prescribing Rivaroxaban, a factor Xa inhibitor at a lower dose of 10 mg daily [22] but in such patients, anti-coagulation is to be considered if a factor VIII level is more than 20%.
In hemophiliacs, if oral anti-coagulants have to be used it is comfortable to use them when trough FVII/FIX and vWF activity levels are >30% and are maintained on that but still a final decision has to be taken after a thorough individual evaluation but in patients with severe hemophilia where the factor activity level is at times even <1%, anti-thrombotic therapy is avoided as bleeding tendency is already very high especially if no clotting factor therapy is ongoing [23]. A multicenter study involving 33 hemophilia patients from 20 European hemophilia centers showed that bleeding occurred in 1 out of 3 hemophilia patients on oral anticoagulant who was not taking prophylactic treatment with clotting factors alongside to maintain factor 8 trough level above 0.2 IU L -1, and this questions the safety of the drugs in this group despite being safe in general population and may need detailed assessment and prophylactic clotting factors before starting their use [12].
Lower doses of Rivaroxaban were proven to be safer than Warfarin as they were associated with lower risk of ischemic stroke and systemic embolism in one of the studies conducted in Asian NVAF patients [29]. Newer anti-coagulant agents reduced the risk of Intra-cranial hemorrhage by half approximately having a risk ratio of 0.44, 95% CI in a study [30].
BEST DRUG IN MAINTAINING OPTIMAL BALANCE
While choosing an anticoagulant for patients who have a high risk of bleeding and inherited bleeding disorders, among all available oral anticoagulant options, considerations should be given to the bleeding risk with each medicine, its reversibility and half-life. Agents with shorter half-life are preferred in patients with bleeding disorders as they are easy to reverse. Warfarin and Dabigatran were frequently used because of the availability of available antidotes [23]. Factor Xa inhibitors were not used in this category of patients as they had no available antidote but recently with approval of antidote of Rivaroxaban and increased safety of FXa inhibitors as compared to Warfarin, they also should be an agent of choice. The issue which arises here now is which agent to choose among Dabigatran and Factor Xa inhibitors.
Considering the high-risk Warfarin has, NOACs are definitely a safer option; Vit K antagonists have more adverse events because of their narrow therapeutic margin and many drug and food interactions. It is considered a leading cause of ER presentations/hospitalizations in the elderly due to its adverse effects [31]. Not many clinical trials are done to assess the safety and efficacy in hemophiliacs with AF, so by comparing the clinical trials in other high risk population and assessing which medications are safer than Warfarin and relative to each other and comparing reviews, consensus and meta-analysis about such scenario, we can indirectly compare the safety and efficacy of such medication. Rivaroxaban was found to be superior to Warfarin in many high risk populations in a review by Diener et al, by comparing the results of ROCKET_AF trial and were found to be consistent in these populations [32]. The EXPAND study conducted in Japan showed low dose of Rivaroxaban in non valvular Atrial fibrillation to have lesser incidence of stroke, and serious bleeding than it's higher dose and Warfarin [33].
The elderly population is a high risk population, whose thrombo-embolic risk is higher than general population using CHADS VASc score which makes age an important factor in scoring, but anticoagulation is not commonly used as needed and anti-platelet agents without anticoagulants are not of much benefit in the elderly but are more prone to cause major bleeding episode [34]. This high-risk group tests the ability of the medication's safety considering the different co-morbidities, the poly-pharmacy in them and the interactions those medications may have as AF is common in the ageing population. With the increased life expectancy in hemophiliacs and the increasing AF in this population, consideration of the medicine which is safe in the ageing population can be considered in this population as well. NOAC's are considered a safer option in the elderly population because of their short half-life and predictable pharmacokinetics and less need for monitoring as Warfarin and the trials showing the decreased chances of intracranial hemorrhage. A meta-analysis by Ruff et al showed these results about their safety and efficacy in 29000 patients over the age 75 [35].
Renal impairment is a condition which is not uncommon in patients with AF, in ageing population and patients with hemophilia. NOAC's have renal route of excretion and so is one of the main limitations when they need to be prescribed to CRF population. Consideration of GFR is important while deciding the oral anticoagulant which needs to be greater than 30 ml/min for prescribing NOACs. An expert Consensus document preferred using Anti Xa inhibitors instead of Vit K Inhibitors with GFR rate ranging from 15-30 ml/min, they were found to have an upper hand in terms of safety in patients with renal impairment as compared to Vit K inhibitors [36]. 20 mg rivaroxaban is superior in efficacy to Warfarin but even low dose of Rivaroxaban at 15 mg was also proven equally efficacious in another study done in Japanese population [29] which can be used in patients with compromised renal functions or even in Hemophiliacs or with both.
In a retrospective study by Villines et al, patients with Dabigatran were compared to Rivaroxaban and to Apixaban separately but the sample size of Apixaban was not statistically significant but for comparison of Dabigatran and Rivaroxaban showed that Dabigatran was associated with less major bleeding events than Rivaroxaban although the rates of thrombo-embolic rate were not different in both of them. So in terms of efficacy both were comparable but in safety from a major bleed Rivaroxaban was found to be superior in this study [37].
The results of one of the studies in which patients with NVAF of >65 years were selected which were recently started on these medications, showed that there was no difference in thrombo-embolic stroke in patients on Rivaroxaban or Dabigatran but an increase in Intra cranial hemorrhage and major bleeding episode risk in the cohort taking Rivaroxaban compared to the one taking Dabigatran [38]. The results of both of these studies were somewhat similar to the results of a few other recent studies like a meta-analysis of different studies by Li et al which also showed that Rivaroxaban, a thrombin inhibitor and Apixaban, a factor Xa inhibitor were comparable in efficacy with Rivaroxaban, another factor Xa inhibitor, but both were better in safety as they were associated with lesser episodes of major bleeding than Rivroxaban [39]. A meta-analyses of 7 studies by Providencia et al concluded that none among both groups Factor Xa and thrombin inhibitors are better in all parameters, one group may be better than other in one thing and may be inferior in other one [40] and hence decision should be taken on individual patient's risk-benefit ratio which is even more important in Hemophiliacs. In those cases where Vit K inhibitors cannot be prescribed, Apixaban was found to be safer alternative [34]. A Consensus report by Gremmel et al also recommended to assess each patient individually for the need of anticoagulation, as except for severe Hemophilia, others may not be protected enough against thrombo-embolism [41], so the decision of specific drug also needs to take in account the specific conditions and co-morbidities of patient. Considering all these limitations, the option of Left Atrial Appendage closure can also be considered and needs to be studied in this group as it may help us to avoid the oral anticoagulants altogether in this group while still preventing thrombosis. A meta-analysis of PROTECT AF and Prevail trial showed similar chances of having ischemic stroke but decreased chances of hemorrhagic stroke as compared to Warfarin [42].
NOAC's although considered a better option in general public have not been studied for efficacy and safety in Hemophiliacs with AF. Hemophilia patients despite having a bleeding risk and decreased tendency for thrombosis may still have thrombosis in pro-thrombotic conditions like Atrial fibrillation. This makes it clear that these patients also have the need for prophylactic anticoagulation as the complication is more serious, but the unreliability of risk assessment scores in this group of patients also needs to be considered. Warfarin was in use for decades for prophylaxis and had been effective in preventing thrombo-embolic stroke but needed frequent monitoring of INR and had frequent drug and food interactions which may make it difficult for these patients. NOACs having different site of action are not dependant on food intake, and the need of less monitoring of INR make it a better option in hemophiliacs with AF having a predictable response, but they may still need clotting factors alongside to prevent major bleeding event, depending on individual assessment. As these conclusions are drawn from research about thrombo-prophylaxis on various other vulnerable groups, more studies are needed to extrapolate these effects in this group. Among NOACs, as shown in different trials / meta-analysis, Dabigatran and Apixaban were shown to be better than Rivaroxaban in having fewer episodes of major intra-cranial bleeding episodes but have the same efficacy in preventing strokes. In case of co-existing CRF since all NOACs have renal route of excretion as well need dose adjustment and need to be decided based on eGFR. Apixaban was the one which could be prescribed in GFR even between 15- 30. There still is a huge gap in knowledge and there is need for more clinical trials in this specific population as not much is available and there is a need to develop proper guidelines about using oral anti-coagulants in Atrial fibrillation with Hemophilia and Inherited coagulation disorders. Considering all these limitations, options like Left Atrial Appendage (LAA) occlusion device therapy may be considered and studied further in this group as a treatment option to avoid long term anti-coagulation in this vulnerable population having high risk of bleeding.






