The Impact of Repeated Cardioversions for Atrial Fibrillation on Stroke, Hospitalizations, and Catheter Ablation Outcomes
Victoria Jacobs 1, Heidi T. May 1, Tami L. Bair 1, Brian G. Crandall 1, Michael J. Cutler DO1, John D. Day 1, Viet Le 1, Charles Mallender1, Jeffrey S. Osborn 1, J. Peter Weiss 1, T. Jared Bunch 1,2
1Intermountain Medical Center Heart Institute, Intermountain Medical Center, Murray, Utah.2Stanford University, Department of Internal Medicine, Palo Alto, California.
Long-term outcomes after direct current cardioversion (DCCV) in patients that receive anticoagulation have demonstrated to have no adverse sequela. Less is known about the impact on atrial fibrillation (AF) outcomes and resource utilization of repeated DCCVs that are often required for long-term rhythm control.
A total of 4,135 AF patients >18 years of age that underwent DCCV with long-term system follow-up were evaluated. Patients were stratified by the number of DCCVs received: 1 (n=2,201), 2-4 (n=1,748), and ≥5 (n=186). Multivariable Cox hazard regression was used to determine the association of DCCV categories to the outcomes of death, AF hospitalization, AF ablation, DCCVs, and stroke/transient ischemic attack.
The average follow-up of the patient population was 1,633.1±1,232.9 (median: 1,438.0) days. Patients who underwent 2-4 and ≥5 DCCVs had more comorbidities, namely hypertension, hyperlipidemia and heart failure. Anticoagulation use was common at the time of DCCV in all groups (89.1%, 91.2%, 91.9%, p=0.06) and amiodarone use increased with increasing DCCV category (30.1%, 43.4%, 52.2, p<0.0001). At 5 years, patients that received more DCCVs had higher rates of repeat DCCVs, AF hospitalizations, and ablations. Stroke rates were not increased. Though not statistically significant, 5-year death was increased when comparing DCCV >5 vs. 1, (HR=1.32 [0.89-1.94], p=0.17).
This study found that the increasing number of DCCVs, despite escalation of other pharmacologic and nonpharmacologic therapies, is a long-term independent risk factor for repeat DCCVs, ablations, and AF hospitalizations among AF patients.
Key Words : Atrial fibrillation, Cardioversion, Stroke, Heart failure, Ablation.
Correspondence to: T. Jared Bunch, M.D.
Intermountain Heart Rhythm Specialists,
Intermountain Medical Center
Eccles Outpatient Care Center
5169 Cottonwood St, Suite 510
Murray, Utah, 84107
Atrial fibrillation (AF) is a rising epidemic that will affect more than 12 million people in the United States by the year 2030.[1-4] AF is the most frequent clinical sustained arrhythmia and is increasing in prevalence as a result of improvements in diagnostic approaches, people living longer, and record growth of systemic co-morbidities associated with AF.[5,6] Direct current cardioversion (DCCV) is one of the modalities used for rhythm control in patients with AF.[7] Typically DCCV is performed if an individual experiences a recent onset of AF, significant symptoms related to AF, hemodynamic instability due to AF, or a high heart rate with myocardial ischemia or hypotension.[8] Therefore, DCCV is used primarily to improve symptoms or to achieve hemodynamic stability in a patient. Recurrences of AF after DCCV are common as arrhythmia provoking substrate persists despite rhythm restoration.[9] Antiarrhythmic medications can be used prior to a DDCV to assist in achieving better success in converting to and maintaining normal sinus rhythm (NSR).[10] Approximately 88% of DCCVs are successful in the restoration of NSR, however the long-term maintenance of NSR is impermanent in many patients and can require repeated DCCVs to achieve control of their arrhythmias. The factors adversely affecting the success of DCCVs include high body mass index, presence of cardiomyopathy, chronic obstructive pulmonary disease, and longer duration of AF.[8,11] Typically, patients with an increased number of co-morbidities are less likely to convert back to AF and require subsequent DCCVs to restore NSR. In addition, these same patients are also more likely to require more than one ablation procedure to sustain NSR. The purpose of this study was to determine differences in long-term outcomes among patients undergoing repeated DCCVs and the potential benefit of additional escalation of rhythm control therapies including repeating DCCV, ablation, and antiarrhythmic drug therapies.
Patients in this study underwent their DCCV procedures at the Intermountain Medical Center Heart Institute. Intermountain Healthcare provides medical care for approximately half of Utah residents, and has integrated electronic medical records for all hospitals within the system, stored in a data warehouse. Patients were included if they were >18 years old and underwent 1 or more DCCVs. The numbers of DCCVs were categorized as: 1, 2-4, and ≥5 for comparative analysis. For example, if the first category was changed to 1-2, 80% of the population would fall into it making further comparisons limited. The lack of use of more DCCVs likely reflects multiple centers within our healthcare network that perform catheter ablation and are comfortable with the use and titration of antiarrhythmic drugs.
The population studied was primarily Caucasian (89%) with other races as follows: Hispanic 7%, Black 2%, Polynesian/Asian 1%, and Native American 1%. Baseline clinical variables were defined using International Classification of Diseases, Ninth and Tenth Revision (ICD-9 and 10) codes of inpatient and outpatient visits prior to or at the time of the first DCCV. Baseline characteristics included age, gender, hypertension, hyperlipidemia, diabetes, smoking history, prior myocardial infarction, cerebrovascular accident, heart failure, prior cerebrovascular accident, prior transient ischemic attack, prior thromboembolism, and cardiomyopathy. The use of HMG-CoA reductase inhibitors (statins), angiotensin converting enzyme inhibitors (ACE inhibitors), angiotensin receptor blockers (ARB), beta blockers, antiarrhythmic medications, aspirin, amiodarone, and all oral anticoagulants were documented.
A diagnosis of AF was determined by searching the hospital discharge summaries for ICD codes for AF (ICD-9: 427.31; ICD-10: I48.0, I48.1, I48.2, I48.91) at index and previous admissions to Intermountain Healthcare hospitals (Salt Lake City, Utah and its surrounding areas) and by searching the Intermountain electrocardiographic database. The electrocardiogram database stores electrocardiograms, ambulatory monitors, and event monitors from all Intermountain Healthcare facilities. These databases are updated daily with completion of the dictated medical reports and physician evaluation of the electrocardiograms.
Patients were followed for the 5 year and long-term outcomes of death, AF hospitalization, AF ablation, cardioversion, and cerebrovascular accident/transient ischemic accident. Patients were censored at the endpoint being evaluated, death, or last day of follow-up.AF hospitalization was defined as having a primary inpatient discharge diagnosis code of ICD-9: 427.31 or ICD-10: I48.0, I48.1, I48.2, or I48.91. Follow-up AF ablation and cardioversion were determined through procedure codes. Cerebrovascular accident/transient ischemic accident were determined using ICD-9 code 433.x1, 434.x1, and 435.x; and ICD-10: I63.x, I64. x., G45.0x, G45.1x, G45.8, G45.9x, and I167.848. Deaths were determined by telephone survey, hospital records, and Utah State Health Department records (death certificates) and were verified through Social Security death records. Patients not listed as deceased in any registry were considered to be alive.
The analysis of variance and the chi-square statistic were used to evaluate differences in baseline and clinical characteristics among the DCCV categories. The Kaplan Meier survival estimate, and the log rank test of survival were used to evaluate initial associations of DCCV categories to the endpoints. Multivariable Cox hazard regression analysis (SPSS, version 22.0) was used to evaluate study endpoints. Final models entered significant (p<0.05) and confounding (10% change in HR) covariables. Two-tailed p-values of <0.05 was designated as nominally significant.
A total of 4,135 patients were included in this study. The distribution of patients in each DCCV category were: 1 DCCV: n=2,201; 2-4 DCCVs: n=1,748, ≥5 DCCVs: n=186. [Table 1] shows the baseline characteristics of the study population stratified by categories of DCCV. Age and sex did not differ between the groups. Those who underwent more DCCVs had more comorbidities (hypertension, hyperlipidemia, heart failure (HF), and cardiomyopathy). Patients who underwent >5 DCCVs were more likely to take amiodarone (52.2%), followed by flecainide (30.6%). The majority of patients received oral anticoagulation: 1 DCCV: 89.1%, 2-4 DCCVs: 91.2% and ≥5 DCCVs: 91.9% (p=0.06).
Table 1. Baseline characteristics stratified by DCCV categories.
|
1 (n=2,201) |
2-4 (n=1,748) |
≥5 (n=186) |
p-value |
| Age (years) |
67.2±11.0 |
66.9±11.1 |
66.8±11.7 |
|
| Sex (male) |
62.4% |
61.3% |
66.7% |
0.32 |
| Hypertension |
81.0% |
86.6% |
94.1% |
<0.0001 |
| Hyperlipidemia |
65.9% |
72.7% |
82.3% |
<0.0001 |
| Diabetes |
27.8% |
31.8% |
35.5% |
0.005 |
| Smoking |
65.9% |
72.7% |
82.3% |
<0.0001 |
| Prior myocardial infarction |
7.8% |
8.2% |
7.0% |
0.81 |
| Heart Failure |
51.0% |
56.3% |
65.6% |
<0.0001 |
| Cerebral Vascular Accident |
6.0% |
6.4% |
7.0% |
0.76 |
| Transient ischemic attack |
7.4% |
8.4% |
9.7% |
0.34 |
| Cardiomyopathy |
31.7% |
38.2% |
53.2% |
<0.0001 |
| CHADS2 |
|
|
|
<0.0001 |
| 0-1 |
36.7% |
30.0% |
19.9% |
|
| 2-4 |
57.8% |
63.7% |
73.1% |
|
| ≥5 |
5.5% |
6.2% |
7.0% |
|
| CHA2DS2-Vasc |
|
|
|
0.001 |
| 0-1 |
15.8% |
12.9% |
7.5% |
|
| 2-4 |
50.5% |
49.7% |
50.5% |
|
| ≥5 |
33.7% |
37.4% |
41.9% |
|
| ACE Inhibitor |
32.2% |
34.3% |
38.2% |
0.14 |
| Angiotensin receptor blocker |
19.5% |
21.2% |
25.8% |
0.08 |
| Beta blocker |
68.8% |
67.8% |
71.0% |
0.62 |
| Calcium channel blocker |
32.9% |
40.8% |
38.2% |
<0.0001 |
| Amiodarone |
30.1% |
43.4% |
52.2% |
<0.0001 |
| Dofetilide |
4.8% |
6.5% |
12.4% |
<0.0001 |
| Flecainide |
23.9% |
29.5% |
30.6% |
<0.0001 |
| Statin |
44.0% |
45.9% |
51.1% |
0.12 |
| Propafenone |
6.5% |
7.6% |
6.5% |
0.38 |
| Sotalol |
18.4% |
18.7% |
23.1% |
0.29 |
| Anticoagulant |
89.1% |
91.2% |
91.9% |
0.06 |
| ASA |
43.5% |
47.1% |
43.5% |
0.08 |
The average length of follow-up among the DCCV categories were: 1 DCCV: 1,718 ± 1,286 (median: 1,515) days, 2-4 DCCVs: 1,563 ±1,174 (median: 1,379) days, ≥5: 1,288 ±1,015 (median: 1,104) days (p<0.0001). The frequencies of 5 year and long-term outcomes are shown in [Table 2]. Data regarding the frequency of DCCVs, time to repeat DCCV, and escalation of antiarrhythmic drug therapies is shown in [Figure 1]
Figure 1. The distribution of cardioversions is shown in A, percentage use of cardioversions in the three groups studied B, time to repeat DCCV per DCCV group in C, rhythm control approaches both pharmacologic and nonpharmacologic per DCCV in D.
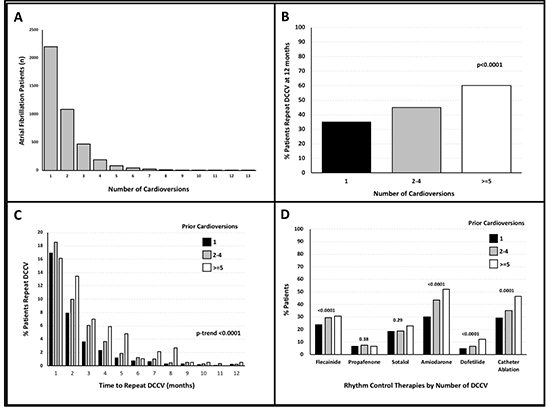
[Table 2] shows the differences in outcome incidences at 5 years. Amongst the outcomes AF-related hospitalization, need for AF ablation, and need for repeat DCCV all significantly increased with higher initial DCCV category. [Figure 2] displays 5-year Kaplan-Meier survival curves among the DCCV categories. Multivariable hazard ratios for the 5-year outcomes are shown in [Figure 3]. After adjusting for comorbidities and medications, comparisons of 2-4 DCCVs and >5 DCCVs versus 1 DCCV were associated with increased risk AF ablations and DCCVs ([Figure 3]). Only the comparison of ≥5 DCCVs versus 1 DCCV were associated with AF hospitalization risk.
[Table 3] displays mortality trends by AAD therapy. Across all 3 DCCV groups there was not an observed increase risk in those patients treated with AADs. In those patients with ≥5 DCCV there was a notable difference in mortality by AAD therapy, although the numbers in each group limited the significance. In regard to AF ablation, there was not a mortality difference noted in the different DCCV groups. However, in patient groups with 1 and 2-4 DCCVs, AF ablation positively impacted subsequent AF hospitalization risk [Table 4].
Table 2. Frequency of 5-year outcomes among DCCV categories.
|
1 |
2-4 |
≥5 |
p-value |
| Death |
17.9% |
19.7% |
25.4% |
0.21 |
| AF hospitalization |
18.0% |
21.3% |
26.8% |
0.05 |
| AF ablation |
29.1% |
35.0% |
46.5% |
0.001 |
| Cardioversion |
40.7% |
49.8% |
64.8% |
<0.0001 |
| CVA/TIA |
7.2% |
6.3% |
9.9% |
0.43 |
Figure 2. Kaplan-Meier survival curves for 5 year A. death, B. AF hospitalizations, C. repeat cardioversion, D. Cerebrovascular accident/transient ischemic accident among DCCV categories.
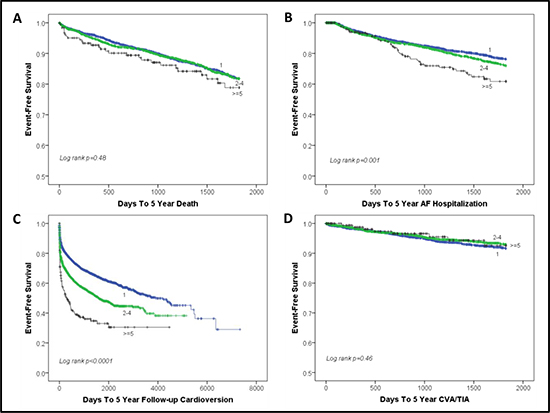
Figure 3. Overall representation of the multivariate adjusted hazard ratios results of: death, cerebrovascular accident/transient ischemic accident, cardioversion, AF and AF ablation.

Table 3. Antiarrhythmic drug use and 5-year mortality risk compared by DCCV use
|
No Antiarrhythmic Drug |
Antiarrhythmic Drug |
p-value |
| 1 DCCV |
17.8% (67/377) |
17.9% (149/833) |
0.96 |
| 2-4 DCCV |
24.5% (36/147) |
18.7% (137/731) |
0.11 |
| ≥5 DCCV |
16.7% (2/12) |
27.1% (16/59) |
0.72 |
Table 4. AF ablation and risk of 5-year AF-related hospitalization compared by DCCV use
|
No ablation |
Ablation |
p-value |
| 1 DCCV |
19.3% (190/987) |
12.6% (28/223) |
0.02 |
| 2-4 DCCV |
22.9% (153/668) |
16.2% (34/210) |
0.04 |
| >=5 DCCV |
25.0% (12/48) |
30.4% (7/23) |
0.63 |
This study has several important associative findings. First, DCCV is an independent predictor of repeat DCCVs, ablations and AF hospitalizations. Second, patients who have undergone repeat DCCVs are less likely to maintain NSR despite escalating use of ablation and antiarrhythmic drug therapies. Third, changes in addressing multiple co-morbidities of AF patients may potentially decrease the need for multiple DCCVs and ablations.
AF in most patients is a progressive chronic disease associated with electrical and structural remodeling of the atrium.[12] These proarrhythmic substrate changes can influence the utility of rhythm control approaches. It is unclear the value adds and impact of augmenting both pharmacologic and nonpharmacologic therapies in an effort to restore sinus rhythm. DCCV is an upfront and immediate therapy to restore NSR and if often use with other pharmacologic and nonpharmacologic rhythm control approaches. In this study, DCCV is also a strong risk marker of a patient that will likely require escalation in other rhythm control approaches in the future and experience higher rates of AF-related comorbidities such as heart failure and death.
Central to these data and findings is the question of what drives AF recurrences beyond the local changes in the atrium of electrical and structural remodeling. If local atrial changes defined outcomes alone, then systemic outcomes such as death would not necessarily be impacted, and rhythm control approaches should result in better outcomes.[13] However, rhythm control approaches in general have consistently failed to lower risk of stroke and mortality. Clinical risk factors of recurrences are prevalent in AF patients such as aging, hypertension, coronary artery disease, obesity, metabolic syndrome, diabetes, cardiomyopathy, sleep apnea and these also contribute to AF-related comorbidities.[14] Within our population despite similar ages, the prevalence of many of these risk factors increased incrementally with the number of DCCVs performed. In support of systemic disease provocation of arrhythmia recurrence and worsening outcomes is that many biomarkers of inflammation, vascular, and cardiovascular disease are elevated in patients with AF recurrences. Amongst these biomarkers, C-Reactive Protein (CRP), natriuretic peptides, troponin, and pro-atrial natriuretic peptide (ANP) and pro-Brain natriuretic peptide (BNP) are all associated with AF recurrences.[15-17]
Next, current pharmacologic therapies are often poorly tolerated, lack efficacy (40-70%), and many are associated with significant side effects that can contribute to morbidity and mortality.[18] In this trial, use of class 1c agents and transition to a ratio of more class 3 agents is observed as DCCV use increased. Despite use of more potent antiarrhythmic drug therapies, AF recurrences were common and reflect the limitations with antiarrhythmic drug therapies as well as systemic disease state and atrium substrate changes that make the disease less amendable to pharmacologic rhythm control therapies.
Finally, although long-term outcomes in patients that underwent an ablation are generally favorable, those with recurrences have worse outcomes such as stroke, dementia, heart failure, and death.[19] In post-ablation patients the recurrence of arrhythmia is also a risk factor of adverse outcomes. Similar findings of improved outcomes are observed in patients that maintain sinus rhythm over time in the AFFIRM trial compared to those that do not independent of treatment strategy. [20] In the AF-Congestive heart failure(CHF) trial the presence of sinus rhythm trended towards lower rates of worsening heart failure (p=0.059), but not mortality.[21] In these studies, with and without ablation, sinus rhythm is a marker of a patient that is more likely to do well. As such, the need for DCCV a reflection of symptomatic AF recurrences is a marker of a worse substrate and risk. In this study, this morbidity and mortality risk persisted despite currently available therapies aimed to restore sinus rhythm (ablation and antiarrhythmic drugs).
This study has some limitations to consider. It is observational and can only provide insight and associations, but not causality. Treatment was defined by the patient’s physician and there may be some variability on treatment preferences, such as the use antiarrhythmic or performing additional DCCVs. Finally, some characteristics and outcomes were determined by ICD-9 and ICD-10 codes. Events may have occurred outside of our medical system and therefore unaccounted for in our data. However, Intermountain Healthcare is the majority provider within the state of Utah and nearby regions with an integrated system of hospitals and clinics, which improves longitudinal follow-up within the system.
Victoria Jacobs: none
Heidi T. May: none
Tami L. Bair: none
Brian G. Crandall: none
Michael J. Cutler: none
John D. Day MD: honorarium/consulting: Abbott Medical, Boston Scientific, Medtronic
Viet Le: None
Charles Mallender:
Jeffrey S. Osborn: honorarium/consulting: Abbott Medical, Boston Scientific, Medtronic, Spectranetics
Peter Weiss: honorarium/consulting: Talon Medical, Stereotaxis
T. Jared Bunch: research grants (no personal compensation): Boehringer Ingelheim, Boston Scientific
DCCV is a long-term independent risk factor for; AF recurrence, catheter ablations and subsequent DCCVs in AF patients. DCCV is also a predictor for an increased incidence in the number of AF related hospitalizations, ablation and subsequent cardioversion needs. The risk association with DCCV was apparent despite increasing use of ablation and antiarrhythmic drug therapies.






