Atypical Reasons for CRT Non-Response in a Pacing Induced Cardiomyopathy Patient
Tony Anno1, Melanie Reed1, Rangarao Tummala 2, Tisha Dooly 1, Amanda McCune1, Randall L. More 1, Wendi Davies 1, Rakesh Gopinathannair2
1Kansas City Veterans Administration Hospital, Kansas City, MO.2Kansas City Heart Rhythm Institute, Overland Park, KS.
Pacing induced cardiomyopathy is a known complication of high percent right ventricular (RV) pacing. When treated with cardiac resynchronization therapy (CRT), most patients experience recovery of Left Ventricular (LV) systolic function.A small percentage of patients do not respond due to a number of factors.This case examines the management of a 30-year-old patient with pacing induced cardiomyopathy who was found to be a CRT non responder despite optimalLV lead position and whose LV Ejection Fraction normalized followingRV lead revision.
Key Words : Cardiac Resynchronization Therapy (CRT), Left Ventricular (LV), CRT non-response.
Correspondence to: Tony Anno, DNP, APRN
Division of Cardiology
Kansas City Veterans Administration Hospital
4801 Linwood Blvd.
Kansas City, MO 64128
Cardiac Resynchronization Therapy (CRT)is standard of care for individuals suffering from dilated cardiomyopathy and heart failure with wide QRS duration.The role of right ventricular (RV) pacing alone has well -known deleterious effects on left ventricular (LV)function and volumes [1]. Pacing - induced cardiomyopathy (PCM) has been defined as LVejection fraction < 45% in a patient with high percentage RV pacing and no other cardiac explanation for the reduction in systolic function. Reported incidence has ranged from 6% to 39% [2] with vast majority of them showing excellent response to CRT upgrade [2].Leclerc et al, in 2016, conducted a study randomly assigning 263 CRT patients to Right Ventricular Septal (RVS) vs. Right Ventricular Apical (RVA) pacing [2]. The results demonstrated that RVS pacing in CRT was non-inferior to RVA pacing at 6 months in reducingleft ventricular end systolic volume (LVESV) [3]. The REVERSE trial found no difference in RV lead placement in CRT [4].While patients with reduced RV ejection fraction experience a slight improvement in response to CRT, the role of RV lead location in this scenario is not clear [5].The REVERSE trial did not look at the detrimental effects of RV free wall placement. There is currently no clear data on the impact of RV free wall lead placement on effective CRT system.Stabile et al (2015) however, did find that patient outcomes after CRT implantation were strongly affected by both electrical and direct interlead distance [6].
A 32-year-old male with marfanoidsyndrome andaortic root replacement as an adolescentdeveloped high degree Atrioventricular (AV) block at age 29 with subsequent dual chamber permanent pacemaker implantation.
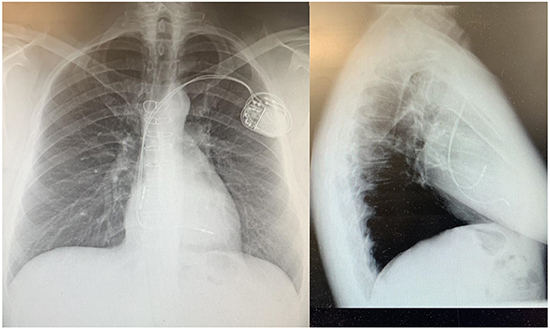
LV ejection fractionat the time of dual chamber pacemaker implantation was 56%. Echocardiogram done 9 months after pacemaker implant showed deterioration of LV ejection fraction from 56 % to 31%. Goal Directed Medical Therapy (GDMT) was initiated and titrated to the maximum dosages including Valsartan-Sacubitril, Carvedilol and Spironolactonebut LV ejection fraction did not improve and therefore the device was upgraded to a CRT-D [Figure 1]. At the time of upgrade his RV pacing lead was extracted easily, without complication, as it was no longer needed. It is not clear from the operative note what measures were taken at implant to assess RV and LV lead separation or right ventricular outflow tract placement. Miranda et al, (2012), also studied implant of the RV lead guided by maximal electrical separation (MES) comparing this to standard apical placement [7]. This study demonstrated a significant improved response to CRT compared to blind apical placement [7].
Figure 1. Chest X-ray of the initial pacemaker system with apparent RV apical lead placement.
Repeat echocardiogramobtained 4 months after upgrade demonstrated an LV ejection fraction of 30%. Pacing and sensing thresholds were demonstrated at acceptable levels. The patientwas havingworsening heart failure symptoms witha deterioration now inNYHA functional class III-IV. Echocardiography revealed lack of septal activation with despite Bi-Ventricular pacing. It was suspected that his lack of septal activation was due tofreewall placement of the RV lead.CT scan obtained supported free wall placement [Figure 1].Given this scenario, a revision of the RVlead was completed 17 months after the initial CRT lead system placement.During the RV lead revision, the LV lead wasinadvertently repositioned and so it was also revised at this time[Figure 2]. The LV lead is in a more lateral position, however it is not significantly different from the initial CRT implant thus unlikely to provide a significant difference in systolic function. Three months after the lead revisionsa repeat echocardiogram showed normalization of LV ejection fractionand septal wall activation [Figure 3]. The patient experienced a reduction in congestive symptoms and hisfunctional class improved to NYHA Functional Class I and he was able to resume normal activities.
Figure 2. PA and Lateral Chest X-Ray and CT of the Chest following CRT-D upgrade of dual chamber pacemaker. Please note the anterior free wall location of the RV lead and minimal lead separation.
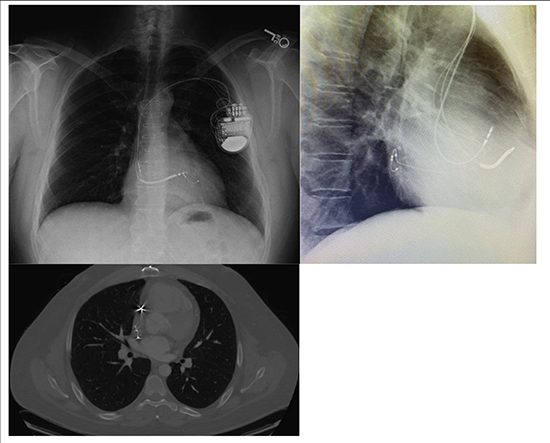
Figure 3. Post Redo CRT CXR with LV lead in a more lateral position and the RV lead in the apical position.
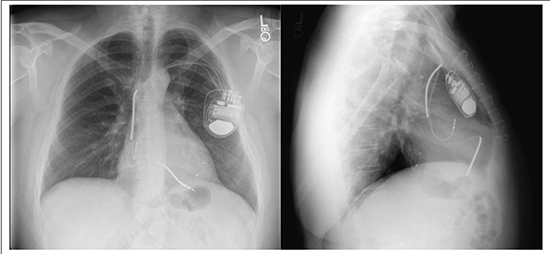
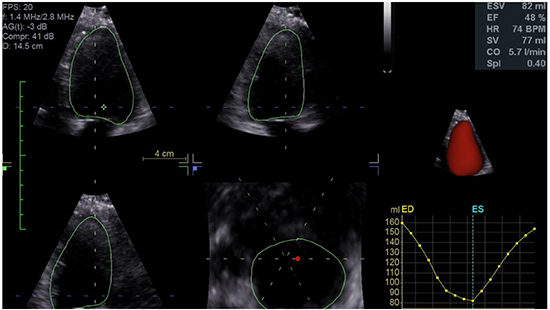
Figure 4. Echocardiogram 3 months after CRT redo reflecting normalized LV function.
Non response to CRT therapy is mostly due to LV lead placement or the lack of ventricular synchrony. The REVERSE trial found no difference between septal or apical placement of RV lead in CRT response [4]. In our case, RV free wall lead placement at time of CRT-D upgrade resulted in inability to activate the septal wall, resulting in worsening LV ejection fraction, development of clinical heart failure and decline of functional status, with two acute hospital admissions requiring diuresis. Echocardiogram following initial CRT upgrade revealed mechanical dyssynchrony with akinesias of the entire septal wall. MRI did not indicate an infiltrative process and no perfusion defects were identified on nuclear stress testing. Revision of RV lead to a more apical location resulted in normal septal activation. Improvement in symptoms were immediately seen,with change in functional status to NYHA Class I within the first month after lead revision. Ventricular synchrony was restored resulting in near normal systolic function. Our report thus suggests that RV lead placement on the free wall, in some patients, can result in lack of septal activation and non-response to CRT. Further studies are needed to elucidate this in detail.
We report a case study where RV free wall lead location resulted in septal akinesis and non-response to CRT in a patient with pacing induced cardiomyopathy. Ventricular function was restored to near normal with RV lead revision.






