Meta-Analysis of Catheter Ablation versus Medical Therapy in Patients with Atrial Fibrillation Without Heart Failure
Zia Khan Muhammad1, Khan Safi U.1, Arshad Adeel2, Samsoor Zarak Muhammad3, Khan Muhammad U.1, Shahzeb Khan Muhammad4, Kaluski Edo5, Alkhouli Mohamad6
1Department of Medicine, West Virginia University, Morgantown, WV, USA.2Rochester Regional Health/Unity Hospital, Rochester, NY.3Department of Cardiovascular Medicine, West Virginia University, Morgantown, WV, USA.4Department of Medicine, John H. Stroger, Jr. Hospital of Cook County, Chicago, IL, USA.5Department of Medicine, Guthrie/Robert Packer Hospital, Sayre, PA, USA.6Department of Cardiovascular Medicine, Mayo Clinic Hospital, Rochester, MN.
Catheter ablation has shown to reduce mortality in patient with atrial fibrillation (AF) and heart failure (HF) with reduced ejection fraction. Its effect on mortality in patients without HF has not been well elucidated.
Thirteen randomized controlled trials encompassing 3856 patients were selected using PubMed, Embase and the CENTRAL till April 2019. Estimates were reported as random effects risk ratio (RR) with 95% confidence intervals (CI).
Compared with medical therapy, catheter ablation did not reduce the risk of all-cause mortality (RR, 0.86, 95% CI, 0.62-1.19, P=0.36; I2=0), stroke (RR, 0.55, 95% CI, 0.18-1.66, P=0.29; I2=0), need for cardioversion (RR, 0.84, 95% CI, 0.66-1.08, P=0.17; I2=0) or pacemaker (RR, 0.59, 95% CI, 0.34-1.01, P=0.06; I2=0). However, ablation reduced the RR of cardiac hospitalization (0.37, 95% CI, 0.18-0.77, P=0.01; I2=86), and recurrent atrial arrhythmia (0.46, 95% CI, 0.35-0.60, P<0.001; I2=87). There were non-significant differences among treatment groups with respect to major bleeding (RR, 1.89, 95% CI, 0.59-6.08, P=0.29; I2=15), and pulmonary vein stenosis (RR, 3.00, 95% CI, 0.83-10.87, P=0.09; I2=0), but had significantly higher rates of pericardial tamponade (RR, 4.46, 95 % CI, 1.70-11.72, P<0.001; I2=0).
Catheter ablation did not improve survival compared with medical therapy in patients with AF without HF. Catheter ablation reduced cardiac hospitalization and recurrent atrial arrhythmia at the expense of pericardial tamponade.
Key Words : Catheter ablation, Atrial fibrillation, Medical therapy, Meta-analysis.
Muhammad Zia Khan, MD
Department of Medicine
West Virginia University
1 Medical Center Drive
Morgantown, WV, USA
Atrial fibrillation (AF) is the most common type of cardiac rhythm disorder, associated with increased morbidity and mortality [1]–[3]. AF has an estimated prevalence of ~ 34 million people worldwide [4]. Guidelines for the management of AF recommends medical therapy (MT) (rate control or rhythm control) as an initial management, however in case of unstable, symptomatic or drug refractory conditions, catheter ablation (CA) is the recommended management [5],[6]. MT for sinus rhythm (SR) restoration has not shown significant survival advantage over a rate-control strategy [7]. Moreover, literature adds that use of antiarrhythmic drugs is associated with increased re-hospitalization. [7]–[10]. Since anti arrhythmic drugs show moderate results in maintaining SR, pro arrhythmic, and causes significant side effects, therefore, physicians need to focus on the safety profile other than efficacy while prescribing them [5]. Moreover, the selection of antiarrhythmic drug becomes limited when the comorbidity, cardiovascular risk, side effects, and preference of the patient is taken into account. Literature has shown significant efficacy of CA both as an initial and secondary approach in management to maintain SR in case of MT failure, improvement in functional status, and cardiac function [11]–[15]. Catheter ablation has shown reduction in mortality with AF and systolic heart failure (HF), however no survival benefit in patients without HF has been observed [16]. Since previous meta-analysis [16], new randomized data has provided further insight on this topic and has the potential to impact clinical outcomes [17], [18]; therefore, we sought to update the meta-analysis in subjects with AF without HF.
This meta-analysis was conducted as per the guidelines of Cochrane Collaboration [19], and it is reported in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) report [20].
DATA SOURCES AND SEARCHES
An updated literature search was conducted to select randomized controlled trials using PubMed, Embase and the CENTRAL till April 2019 using key search terms, “atrial fibrillation”, “catheter ablation”, “pulmonary vein isolation” and “antiarrhythmic drugs”. The PubMed search algorithm is reported in the [Table 1]. A gray literature [21],[22] search was carried out by searching www.clinicaltrialresults.com, www.clinicaltrials.gov, www.cardiosource.org, www.esccardio.org, and abstracts and presentations from major cardiovascular meetings. Reference lists of the relevant articles were also reviewed. All citations were downloaded into EndNote X7 (Thompson ISI ResearchSoft, Philadelphia, Pennsylvania), and duplicates were removed electronically and manually.
Table 1. Baseline characteristics of the randomized clinical trials.
| First Author/Study (Year) |
Groups(Ablation vs AAD Class) |
N |
Mean Age (yrs) |
Male (%) |
SHD (%) |
LAD (mm) |
DM (%) |
CAD (%) |
Prior Stroke (%) |
LVEF (%) |
Cross over to RFA (%) |
| Krittayaphong et al. (2003) |
Ablation |
15 |
55 |
73 |
13 |
40 |
6.7 |
NR |
NR |
64 |
NR |
| Amio |
15 |
49 |
53 |
13 |
39 |
20 |
NR |
NR |
62 |
NR |
| Wazni et al. (2005) |
Ablation |
33 |
53 |
NR |
28 |
41 |
NR |
NR |
NR |
53 |
NR |
| Class I, III |
37 |
54 |
NR |
28 |
42 |
NR |
NR |
NR |
54 |
NR |
| Oral et al. (2006) |
Ablation |
77 |
55 |
87 |
08 |
45 |
NR |
NR |
NR |
55 |
77 |
| Amio |
69 |
58 |
90 |
09 |
45 |
NR |
NR |
NR |
56 |
77 |
| APAF (2006) |
Ablation |
99 |
55 |
70 |
07 |
40 |
5.1 |
NR |
NR |
60 |
42 |
| Class I, III |
99 |
57 |
65 |
04 |
38 |
4 |
NR |
NR |
61 |
42 |
| Stabile et al. (2006) |
Ablation |
68 |
62 |
62 |
63 |
46 |
NR |
NR |
NR |
59 |
52 |
| Class I, III |
69 |
62 |
64 |
62 |
45 |
NR |
NR |
NR |
58 |
52 |
| A4 study (2008) |
Ablation |
53 |
50 |
85 |
19 |
39 |
1.9 |
5.7 |
NR |
63 |
63 |
| Class I, III |
59 |
52 |
83 |
24 |
40 |
3.4 |
10 |
NR |
66 |
63 |
| Forleo et al. (2009) |
Ablation |
35 |
63 |
57 |
46 |
44 |
NR |
20 |
NR |
55 |
NR |
| Class I, III |
35 |
65 |
66 |
54 |
45 |
NR |
20 |
NR |
53 |
NR |
| Wilber et al. (2010) |
Ablation |
106 |
55.5 |
68.9 |
9.5 |
NR |
9.5 |
NR |
1.9 |
62.3 |
NR |
| Class I, III |
61 |
56.1 |
62 |
15 |
NR |
12 |
NR |
3 |
62.7 |
NR |
| MANTRA PAF (2012) |
Ablation |
146 |
56 |
68 |
5 |
40 |
4 |
4 |
NR |
NA |
36 |
| Class I, III |
148 |
54 |
72 |
10 |
40 |
7 |
1 |
NR |
NA |
36 |
| SARA (2014) |
Ablation |
98 |
55 |
76 |
NR |
NR |
NR |
3.1 |
3.1 |
61.1 |
47.9 |
| Class I, III |
48 |
55 |
37 |
NR |
NR |
NR |
2.1 |
2.1 |
60.8 |
47.9 |
| RAAFT2 (2014) |
Ablation |
66 |
56 |
77 |
NR |
40 |
1.5 |
9.1 |
4.6 |
61.4 |
47 |
| Class I, III |
61 |
54 |
74 |
NR |
43 |
6.6 |
3.3 |
6.6 |
60.8 |
47 |
| CAPTAF (2019) |
Ablation |
79 |
55.8 |
73.4 |
1.3 |
41.7 |
3.8 |
2.5 |
5.1 |
56.2 |
10.1 |
| Class I, III |
76 |
56.3 |
81.6 |
1.3 |
41.7 |
3.9 |
3.9 |
0 |
56.1 |
10.1 |
| CABANA (2019) |
Ablation |
1108 |
68 |
62.7 |
NR |
NR |
25.3 |
18.8 |
6.1 |
- |
27.1 |
| Class I, III |
1096 |
67 |
63 |
NR |
NR |
25.7 |
19.7 |
5.3 |
- |
27.1 |
A4 Study=A Comparison of Antiarrhythmic Drug Therapy and Radio Frequency Catheter Ablation in Patients With Paroxysmal Atrial Fibrillation; AF = atrial fibrillation; Amio = amiodarone; APAF=Ablation for Paroxysmal Atrial Fibrillation; CABANA= The Catheter Ablation vs Antiarrhythmic Drug Therapy for Atrial Fibrillation Trial; CAD=coronary artery disease; CAPTAF= Catheter Ablation compared with Pharmacological Therapy for Atrial Fibrillation; class I, III = class I, III antiarrhythmic agents; DM = diabetes mellitus; LAD = left atrial diameter; LVEF = left ventricular ejection fraction; MANTRA-PAF = Medical Antiarrhythmic Treatment or Radiofrequency Ablation in Paroxysmal Atrial Fibrillation: A Randomized Prospective Multicenter Study; NA = not available; NR = not reported; RAAFT2 = Radiofrequency Ablation vs Antiarrhythmic Drugs as First-Line Treatment of Paroxysmal Atrial Fibrillation; RFA = radiofrequency ablation; SARA = Study of Ablation Versus antiarrhythmic Drugs in Persistent Atrial Fibrillation; SHD = structural heart disease
Two independent reviewers (M.Z.K. and M.Z.) analyzed the citations at the level of title and abstract, and the studies were considered on the basis of following criteria: 1) RCTs investigating CA versus MT (rhythm- or rate-control medications) in patients with AF; and 2) studies reporting at least 1 event for outcomes of interest in an adult population. Moreover, the inclusion criteria for studies was not limited to sample size, language preference, follow up duration or availability of the full text. The whole process was supervised by a third author (S.U.K.), and any discrepancies were resolved by consensus.
QUALITY ASSESSMENT AND DATA EXTRACTION
Two independent authors (M.U.K and A.A.) used a structured data collection form to abstract the data for baseline characteristics, techniques of the procedure, events, nonevents, mode of medical treatment, sample size, mean, standard deviations, crude point estimates or standard error estimates, and follow-up duration. Additionally, the continuous outcomes were extracted as per the differences between the 2 groups during the follow up in addition to any changes from baseline. For all estimates, adjusted estimates were extracted. Intention-to-treat principle was used as basis for the acquisition of data. Data adjudication was done by 1 author (S.U.K.). Methodological quality or risk bias assessment was done at study level using the Cochrane bias risk assessment tool [23] [Table 1].
The primary endpoint was all-cause mortality. The secondary endpoints were stroke, cardiac hospitalization, recurrent atrial arrhythmia, need for cardioversion or pacemaker, major bleeding, pulmonary vein stenosis and pericardial complications. The definitions of the endpoints were taken as reported in the included trials.
Estimates were assessed by using a DeSermonian and Laird random effects model. We preferred a random effects model to account for any study heterogeneity [24]. Binary outcomes were calculated as risk ratio (RR) or risk difference, and continuous estimates were expressed as mean difference (MD) with 95% confidence interval (CI). Because both the RR and risk difference represent the same data, we focused on RR estimates in this review. A p value of 0.05 was set as significant. Heterogeneity was assessed using Q statistics and quantified by I2 with values >50% consistent with a high degree of heterogeneity [25]. Publication bias was assessed using Egger’s regression test. All analyses were conducted using Comprehensive Meta-analysis software version 3.0 (Biostat, Englewood, New Jersey).
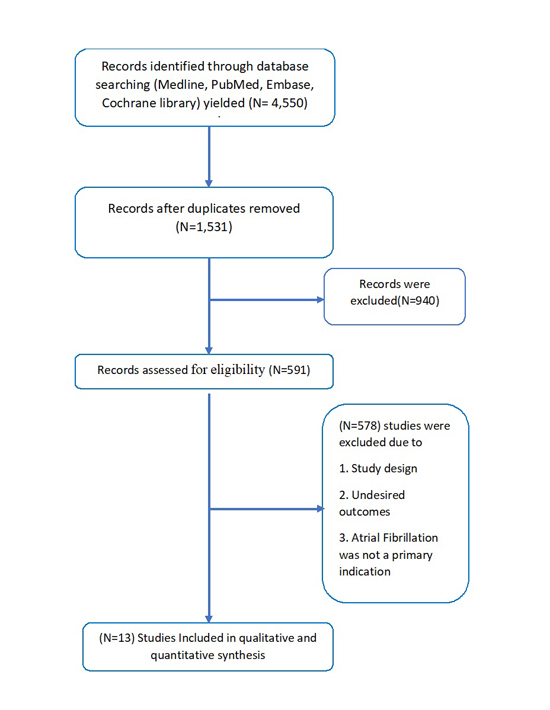
The initial search yielded 4,550 records, of which 3,019 citations were removed as duplicates; of the remaining 1,531 articles, 940 studies were excluded if the title and/or abstract suggested that the studies were not relevant. A total of 591 records were assessed for eligibility, of which 578 studies were excluded because of their study design or undesired outcomes or when AF was not a primary indication. Ultimately, 13 RCTs (3856) met the inclusion criteria [Figure 1]. Baseline characteristics of the trials are shown in [Table 1] [18],[19],[26]–[36].
Figure 1. Flow Chart of our study
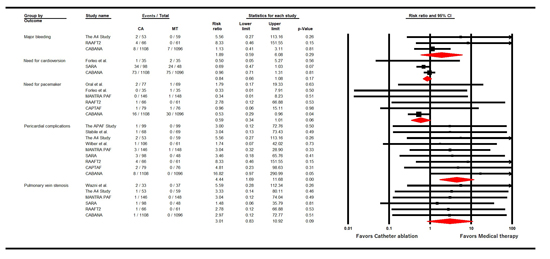
In 13 trials (3856 patients), the pooled mean age of patients was 56.8±4.8 years, 69% were males and 8.8% had coronary artery disease. The mean left ventricular ejection fraction (LVEF) was 59.1±3.8%, 67% patients had paroxysmal AF and 33% had persistent AF. The average follow-up duration was 19 months. Compared with medical therapy, ablation did not reduce the RR of all-cause mortality (0.86 [95% CI, 0.62-1.19], P=0.36; I2=0; [Figure 2]) and stroke (0.55 [95% CI, 0.18-1.66], P=0.29; I2=0). However, ablation reduced the RR of cardiac hospitalization (0.37 [95% CI, 0.18-0.77], P=0.01; I2=86), and recurrent atrial arrhythmia (0.46 [95% CI, 0.35-0.60], P<0.001; I2=87). There were non-significant differences among treatment groups with respect to safety outcomes [Figure 3] such as major bleeding (1.89 [95% CI, 0.59-6.08], P=0.29; I2=15), need for cardioversion (0.84 [95% CI, 0.66-1.08], P=0.17; I2=0) or pacemaker (0.59 [95% CI, 0.34-1.01], P=0.06; I2=0) and pulmonary vein stenosis (3.01 [95% CI, 0.83-10.92], P=0.09; I2=0). However, pericardial complications were more common among the ablation group (4.44 [95% CI, 1.69-11.68], P<0.001; I2=0). Egger’s regression test did not detect publication bias for primary endpoint (P=0.94).
Figure 2. Forest Plot Showing Results of Catheter Ablation versus Medical Therapy in Patients with Atrial Fibrillation Without Heart Failure
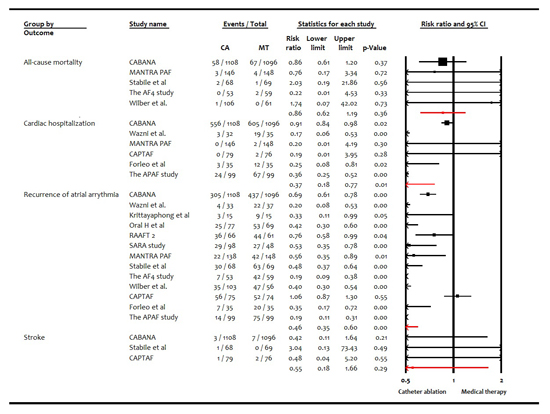
Figure 3. Forest Plot showing safety analysis between Catheter Ablation versus Medical Therapy in Patients with Atrial Fibrillation Without Heart Failure
In this meta-analysis, ablation did not reduce the risk of total mortality, stroke, need for cardioversion or pacemaker compared with medical therapy in patients with AF without HF. However, ablation was associated with 63% RR reduction of for cardiac hospitalization and 54% for recurrent atrial arrhythmia. Previous meta-analysis [13]-[16] addressed a mix of both HF and non-HF population, however those studies were limited by low power for hard outcomes and brief follow-ups of non-HF trials. Whereas, current meta-analysis was updated with the CABANA (Catheter Ablation Vs Antiarrhythmic Drug Therapy for Atrial Fibrillation) trial, the largest and longest follow-up study powered to assess effect of catheter ablation on mortality in subjects with AF without HF [17], and the CAPTAF (Catheter Ablation compared with Pharmacological Therapy for Atrial Fibrillation) trial [18] to confirm catheter ablation’s lack of benefit on hard clinical endpoints in this subset of patients. Ablation was not significantly associated with stroke prevention but most of the patients with stroke risk factors were on anticoagulation even after ablation, therefore, making it difficult to assess actual stroke risk change with ablation. It remains uncertain whether after ablation anticoagulation can be safely discontinued. Ongoing the OCEAN (Optimal Anticoagulation for Higher Risk Patients Post Catheter Ablation for Atrial Fibrillation) trial (NCT02168829) will shed further light on this issue. Our analysis showed ablation had statistically significance reduction for cardiac hospitalization, the persistent benefits of having reduced risk for cardiac hospitalization and recurrent atrial arrhythmia with ablation are reassuring and carry significant implications for quality of life and health care expenditures. Finally, although, ablation was generally safe in terms of major bleeding or pulmonary vein stenosis, the benefits of reduced hospitalization and recurrent arrythmias were somewhat counterbalanced by higher rates of pericardial complications like cardiac tamponade, although infrequent, can be serious complications with significant mortality and morbidity [36].
Considerable limitations of this meta-analysis include variations in ablation strategies, duration of treatment, post ablation antiarrhythmic therapy, methods of AF surveillance, CHA2D-VAS2c scores and follow-up durations. In addition to lack of blinding, protocol adherence and cross over were not random across most of the trials, therefore a high degree of selection bias was noticed. All-cause mortality was not adequately powered in any of the included individual trials. We refrained from assessment of Quality of Life due to paucity of data and heterogeneity in measurement scales. The safety endpoints were not powered and lacked precision. Moreover, this analysis is mainly driven by the CABANA trial as it had the highest number of participants.
Although among patients with AF without HF, ablation was associated with lower rates of cardiac hospitalization and recurrent atrial arrhythmia compared with medical therapy, subjects receiving ablation did not experience mortality benefit. Therefore, perceived advantages of ablation in “healthy” subjects with AF must be closely weighed against potential complications and health care use costs [37].
- Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001 May 9;285(18):2370-2375.
- Chugh SS, Havmoeller R, Narayanan K, Singh D, Rienstra M, Benjamin EJ, Gillum RF, Kim YH, McAnulty Jr JH, Zheng ZJ, Forouzanfar MH. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014 Feb 25;129(8):837-847.
- Dries D, Exner D, Gersh B, Domanski M, Waclawiw M, Stevenson L. Atrial fibrillation is associated with an increased risk for mortality and heart failure progression in patients with asymptomatic and symptomatic left ventricular systolic dysfunction: a retrospective analysis of the SOLVD trials. JACC. 1998 Sep 1;32(3):695-703.
- Chugh Sumeet S, Havmoeller R, Narayanan K et al. Worldwide Epidemiology of Atrial Fibrillation. Circulation 2014;129:837-847.
- Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur J Cardiothorac Surg 2016;50:e1–88.
- January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2014;64:e1–76.
- Roy D, Talajic M, Nattel S, Wyse DG, Dorian P, Lee KL, Bourassa MG, Arnold JM, Buxton AE, Camm AJ, Connolly SJ. Rhythm control versus rate control for atrial fibrillation and heart failure. N Engl J Med. 2008 Jun 19;358(25):2667-2677.
- Chatterjee S, Sardar P, Lichstein E, Mukherjee D, Aikat S. Pharmacologic rate versus rhythm‐control strategies in atrial fibrillation: an updated comprehensive review and meta‐analysis. Pacing Clin. Electrophysiol. 2013 Jan;36(1):122-133.
- de Denus S, Sanoski CA, Carlsson J, Opolski G, Spinler SA. Rate vs rhythm control in patients with atrial fibrillation: a meta-analysis. Archives of Internal Medicine. 2005 Feb 14;165(3):258-262.
- Wyse DG. Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) Investigators: A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002;347:1825-1833.
- Khan AR, Khan S, Sheikh MA, Khuder S, Grubb B, Moukarbel GV. Catheter ablation and antiarrhythmic drug therapy as first-or second-line therapy in the management of atrial fibrillation: systematic review and meta-analysis. Circulation: Arrhythmia and Electrophysiology. 2014 Oct;7(5):853-860.
- Shi LZ, Heng R, Liu SM, Leng FY. Effect of catheter ablation versus antiarrhythmic drugs on atrial fibrillation: A meta-analysis of randomized controlled trials. Experimental and therapeutic medicine. 2015 Aug 1;10(2):816-822.
- Zhu M, Zhou X, Cai H, Wang Z, Xu H, Chen S, Chen J, Xu X, Xu H, Mao W. Catheter ablation versus medical rate control for persistent atrial fibrillation in patients with heart failure: a PRISMA-compliant systematic review and meta-analysis of randomized controlled trials. Medicine (Baltimore). 2016 Jul;95(30):e4377. doi: 10.1097/MD.0000000000004377.
- Zhang B, Shen D, Feng S, Zhen Y, Zhang G. Efficacy and safety of catheter ablation vs. rate control of atrial fibrillation in systolic left ventricular dysfunction. Herz. 2016 Jun 1;41(4):342-350.
- Al Halabi S, Qintar M, Hussein A, Alraies MC, Jones DG, Wong T, MacDonald MR, Petrie MC, Cantillon D, Tarakji KG, Kanj M. Catheter ablation for atrial fibrillation in heart failure patients: A meta-analysis of randomized, controlled trials. JACC: Clinical Electrophysiology. 2015 Jun 1;1(3):200-209.
- Khan SU, Rahman H, Talluri S, Kaluski E. The Clinical Benefits and Mortality Reduction Associated With Catheter Ablation in Subjects With Atrial Fibrillation: A Systematic Review and Meta-Analysis. JACC Clinical electrophysiology 2018;4:626-635.
- Packer DL, Mark DB, Robb RA et al. Effect of Catheter Ablation vs Antiarrhythmic Drug Therapy on Mortality, Stroke, Bleeding, and Cardiac Arrest Among Patients With Atrial Fibrillation: The CABANA Randomized Clinical Trial. JAMA. 2019 Apr 2;321(13):1261-1274. doi: 10.1001/jama.2019.0693.
- Blomstrom-Lundqvist C, Gizurarson S, Schwieler J et al. Effect of Catheter Ablation vs Antiarrhythmic Medication on Quality of Life in Patients With Atrial Fibrillation: The CAPTAF Randomized Clinical Trial. JAMA 2019;321:1059-1068.
- Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0: updated March 2011. London, United Kingdom: Cochrane Collaboration; 2011. Available at: http://handbook-5-1.cochrane.org/. Accessed March 6, 2019.
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, Devereaux PJ, Kleijnen J, Moher D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS medicine. 2009 Jul 21;6(7):e1000100.
- Hopewell S, McDonald S, Clarke MJ, Egger M. Grey literature in meta‐analyses of randomized trials of health care interventions. Cochrane Database of Systematic Reviews. 2007(2).
- Benzies KM, Premji S, Hayden KA, Serrett K. State‐of‐the‐evidence reviews: advantages and challenges of including grey literature. Worldviews on Evidence‐Based Nursing. 2006 Jun;3(2):55-61.
- Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, Savović J, Schulz KF, Weeks L, Sterne JA. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. Bmj. 2011 Oct 18;343:d5928.
- DerSimonian R, Kacker R. Random-effects model for meta-analysis of clinical trials: an update. Contemporary clinical trials. 2007 Feb 1;28(2):105-14.
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003 Sep 4;327(7414):557-60.
- Krittayaphong R, Raungrattanaamporn O, Bhuripanyo K, Sriratanasathavorn C, Pooranawattanakul S, Punlee K, Kangkagate C. A randomized clinical trial of the efficacy of radiofrequency catheter ablation and amiodarone in the treatment of symptomatic atrial fibrillation. J Med Assoc Thai. 2003 May;86 Suppl 1:S8-16..
- Wazni OM, Marrouche NF, Martin DO, Verma A, Bhargava M, Saliba W, Bash D, Schweikert R, Brachmann J, Gunther J, Gutleben K. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation: a randomized trial. JAMA. 2005 Jun 1;293(21):2634-2640.
- Oral H, Pappone C, Chugh A, Good E, Bogun F, Pelosi Jr F, Bates ER, Lehmann MH, Vicedomini G, Augello G, Agricola E. Circumferential pulmonary-vein ablation for chronic atrial fibrillation. N Engl J Med 2006 Mar 2;354(9):934-941.
- Pappone C, Augello G, Sala S, Gugliotta F, Vicedomini G, Gulletta S, Paglino G, Mazzone P, Sora N, Greiss I, Santagostino A. A randomized trial of circumferential pulmonary vein ablation versus antiarrhythmic drug therapy in paroxysmal atrial fibrillation: the APAF Study. JACC. 2006 Dec 5;48(11):2340-2347.
- Stabile G, Bertaglia E, Senatore G, et al. Catheter ablation treatment in patients with drug refractory atrial fibrillation: a prospective, multicentre, randomized, controlled study (Catheter Ablation For The Cure Of Atrial Fibrillation Study). Eur Heart J 2006;27:216–221.
- Jaïs P, Cauchemez B, Macle L, Daoud E, Khairy P, Subbiah R, Hocini M, Extramiana F, Sacher F, Bordachar P, Klein G. Catheter ablation versus antiarrhythmic drugs for atrial fibrillation: the A4 study. Circulation. 2008 Dec 9;118(24):2498-2505.
- Forleo GB, Mantica M, De Luca L, Leo R, Santini L, Panigada S, De Sanctis V, Pappalardo A, Laurenzi F, Avella A, Casella M. Catheter ablation of atrial fibrillation in patients with diabetes mellitus type 2: results from a randomized study comparing pulmonary vein isolation versus antiarrhythmic drug therapy. J. Cardiovasc. ElectrophysioL. 2009 Jan;20(1):22-28.
- Wilber DJ, Pappone C, Neuzil P, De Paola A, Marchlinski F, Natale A, Macle L, Daoud EG, Calkins H, Hall B, Reddy V. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010 Jan 27;303(4):333-340.
- Cosedis Nielsen J, Johannessen A, Raatikainen P, et al. Radiofrequency ablation as initial therapy in paroxysmal atrial fibrillation. N Engl J Med 2012;367:1587–1595.
- Mont L, Bisbal F, Hernandez-Madrid A, Perez-Castellano N, Viñolas X, Arenal A, Arribas F, Fernández-Lozano I, Bodegas A, Cobos A, Matía R. Catheter ablation vs. antiarrhythmic drug treatment of persistent atrial fibrillation: a multicentre, randomized, controlled trial (SARA study). Eur. Heart J. 2013 Oct 17;35(8):501-507.
- Morillo CA, Verma A, Connolly SJ, Kuck KH, Nair GM, Champagne J, Sterns LD, Beresh H, Healey JS, Natale A. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of paroxysmal atrial fibrillation (RAAFT-2): a randomized trial. JAMA. 2014 Feb 19;311(7):692-700.
- Kistler PM, Voskoboinik A. Catheter Ablation: First-Line Therapy for Atrial Fibrillation in Systolic Heart Failure? JACC Clinical electrophysiology 2018;4:636-637.






