High Cerebrovascular Thromboembolic Event Rate Long after Unsuccessful Catheter Ablation for Atrial Fibrillation
Zsuzsanna Kis1, Mihran Martirosyan1, Astrid Armanda Hendriks1, Dominic Theuns1, Rohit Bhagwandien1, Sip Wijchers1, Sing-Chien Yap1, Tamas Szili-Torok1
Department of Cardiology, Erasmus MC, University Medical Center, Rotterdam, the Netherlands.
Although catheter ablation (CA) is an accepted therapeutic option for atrial fibrillation (AF), data is lacking concerning the long-term thromboembolic event (TE) and mortality rate of patients after unsuccessful CA for AF.
The aim of the current study was to detect the long-term TE and mortality rate of patients with successful CA (group A) of AF and compared those with unsuccessful ablation (group B).
Following a 4-years of follow-up (FU) 330 patients were included into the groupA, and 105 patients into the group B. Primary outcome was defined as all stroke/TIA occurrence. Secondary outcome was considered as all-cause mortality and stroke - and TIA only occurrence.
Seventeen patients developed a stroke/TIA during a median of 5.8 [5.1-7.3] years of FU. In the group A 8 (2.4%) patients developed a stroke/TIA during a FU of 2037 person-years (incidence rate 3.92 per 1000 person-years), compared to 9 patients in the group B during a FU of 726 person-years (incidence rate 12.4 per 1000 person-years). The crude HR for primary outcome was 2.84 (95% CI 1.078-7.48) in the group B compared with the group A. Cumulative TIA-alone incidence (3.97, CI 1.10-14.34, p=0.035) and the annualized TIA-alone incidence rate was significantly higher in the group B. (p=0.029). Neither the mortality rate nor the incidence rate of stroke-alone differed significantly among the groups.
The risk of all stroke/TIA and TIA-alone is higher among patients after unsuccessful CA of AF compared to those after successful ablation.
Key Words : Atrial fibrillation, Catheter ablation, Ischemic stroke, Long-term follow-up.
Correspondence to: Tamas Szili-Torok, MD., PhD
Thoraxcenter, Department of Clinical Electrophysiology, Erasmus MC
Postbus 2040, 3000 CA Rotterdam, The Netherlands
`s Gravendijkwal 230
Atrial fibrillation (AF) is associated with an increased risk of mortality and morbidity including thromboembolic events, and worsening of heart failure (HF).1,2 The AF management involves rhythm and rate control therapy. Furthermore, AF management focuses on the prevention of AF-associated complications (stroke, transient ischemic attack (TIA), HF). Pulmonary vein isolation (PVI) with catheter ablation (CA) is an increasingly sophisticated and widely available non-pharmacological method for rhythm control in AF management. 1,2 Randomized clinical trials have demonstrated the superiority of CA for AF as compared to pharmacological treatment.3-6 Despite significant improvement in CA technology the long-term outcome is still suboptimal after technically successful CA for AF.7 Moreover, no data is available about the long-term outcome including mortality, thromboembolic complication and alterations of left ventricle (LV) function of patients in whom catheter ablation as rhythm control strategy was declared unsuccessful.
The aim of this study was to provide long-term outcome of patients after failed AF ablation as compared to a control group of patients with successful CA of AF.
Data collection for this study was approved by the institutional review board and the ethical committee. All patients were eligible for PVI due to AF according to the guidelines.1,2 Informed consent was obtained from all patients for the planned CA procedures. For data collection we used the so called “ElPaDo” institutional electronic patient dossier database (ElPaDo), which contains all patient-related health issues, also provided by peripheral health institutes in a scanned letter form. Thus, all relevant health events investigated in the present study including stroke, TIA and mortality was tracked from records not only from the Cardiology department but also from the departments of different subspecialties.
Patient population and follow up
All consecutive individuals who had undergone a CA of AF between March 2001 and January 2016 were screened for this study. Only patients with no prior AF ablation history and those who completed a minimum period of 4-year of follow-up (FU) were eligible for study inclusion. All patients with the a) presence of pre-procedural intra-cavital thrombus, b) with any contraindication for anticoagulation therapy and c) those with inability to provide informed consent were excluded from the present study. Patients were enrolled into two groups.
Patients after “successful” CA will be referred as those in group A, while patients after “unsuccessful” CA cohort will be referred in the text as those in group B. Long-term outcome data between these groups were compared.
The group A included those with successful AF ablation. These patients were in SR throughout the follow up after single or repeated AF ablation procedures being on or off rhythm-control AAD treatment.
Unsuccessful ablation (group B) was defined as the followings: in whom normal sinus rhythm (SR) could not be maintained despite repeated CA for AF or the use of anti-arrhythmic drug (AAD) therapy. These patients remained on rate control AAD management with or without pacemaker (PM) backup or underwent a MAZE procedure otherwise a His-bundle ablation after PM implantation was performed. The strength of this database and our study is the extended follow up of four years. In many cases it required dossier analysis because 4 years follow up is far beyond our standard routine. This revealed in many cases that the first sign of recurrence was a cerebrovascular incident years after the initial procedure.
Study variables and study endpoints
We collected the following data: demographic and descriptive variables including age, gender, AF type, AF duration. Comorbid conditions were defined as hypertension (HT), diabetes mellitus (DM), hyperlipidemia, thyroid and renal function, smoking. The following echocardiographic parameters were collected and compared: left atrial (LA) size, ejection fraction (EF) and mitral insufficiency (MI). The stroke risk stratification (CHA2DS2-VASC) score were calculated from the individual stroke risk factors: congestive heart failure, hypertension, age 75 or more, diabetes mellitus, stroke or TIA, vascular disease, sex category (female) and age 65-74.9 years.
The primary study endpoint was defined as stroke or TIA and will be referred in the text as stoke/TIA after PVI. Stroke-alone, TIA-alone and all-cause mortality were considered secondary outcomes in the present study. The follow-up period started in all participants at the date of primary PVI and continued until outcome event (stoke/TIA after PVI), death, loss to follow-up or December 31, 2016, whichever came first.
Catheter ablation and periprocedural management of anticoagulation
Complete PVI was the procedural endpoint in all cases guided by 3-dimensional mapping system with a wide variety of techniques including cryoballoon (CB) in 68% and radiofrequency (RF) ablation in 22% while robotic navigated ablation was utilized in 13% of the patients. Lesions were directed only to the pulmonary veins in 54% (75/139) in the RF ablated patients. Additional lesions were targeted to fractionated electrograms in 4%, and linear lines (PVI + linear lines: 40/139 patients, PVI+CTI:18/139 patients) were utilized in 42 % mostly in persistent AF patients.
The ablation approach such as the peri-ablation antiarrhythmic drug and anticoagulation management and also the follow-up methodology was determined by the patient’s electrophysiologist following the currently available guidelines.
Continuous variables are expressed as mean SD or as median and quartiles (Q1-Q3), where appropriate. Categorical data are shown as percentages. For statistical comparison, the non-normally distributed variables were compared with the Man-Whitney test, while ordinal variables were analyzed with the chi-square- test and nominal variables with the Student T-test. These comparisons were made for all demographics, use measures, comorbidities. Multivariate analysis of predictors of stroke was by Cox-regression and included the following factors: age, presence of paroxysmal AF, LA size. A P value of 0.05 was considered statistically significant. The annualized incidence rate of stroke/TIA were estimated by dividing the number incident cases of stroke/TIA by total follow-up time. It was expressed as number per 1000 person-years of observation. Because time to stroke/TIA can be competing risk of mortality, cumulative incidence function was used to estimate the distribution of time to stroke/TIA and to secondary outcome. Statistical analysis was performed with SPSS Statistics for Windows, Version 24.0.
1002 patients who underwent PVI were screened for this study. Finally, 435 patients were enrolled into the study analysis. Three-hundred thirty patients after a successful AF ablation were included into the group A. Of the latter group, 105 patients were included into the group B after a CA for AF with a completed 4-year of follow-up.
The baseline demographic and clinical data of patients are listed in [Table 1]. The group B had significantly larger LA size (p=0.003), included significantly less patients with paroxysmal AF (p=0.001) and had more patients above 75 years of age (p=0.02). There was no significant difference between the study groups in age, gender and comorbid conditions such as hypertension, diabetes, hyperlipidaemia, hearth failure, COPD, renal or thyroid function.
Smoking and overweighed patients were similarly represented in the two groups. The CHA2DS2VASC score profile, furthermore the thromboembolic history, likewise the vascular and valvular heart disease rate were not different between the investigated groups.
Table 1. Patient demographic, echocardiographic data and stroke risk factors
|
Total (%) N=435 |
Pts with successful ablation (%) N=330 |
Pts with unsuccessful ablation (%) N=105 |
P-value |
| Sex (Female) |
120/435 (28) |
93/330 (28) |
27/105 (26) |
0.71 |
| Age (years) |
559 |
5610 |
569.5 |
0.937 |
| Age > 65 years |
78/435 (17.93) |
65/330 (19.67) |
13/105 (12.3) |
0.108 |
| Age > 75 years |
8/435 (1.84) |
3/330 (0.9) |
5/105 (4.76) |
0.022 |
| Paroxysmal AF |
391/435 (89.9) |
307/330 (93) |
84/105(80) |
0.001 |
| AF duration (years) |
2 [1-4] |
2 [1-4] |
2 [1-4] |
0.573 |
| LA size (mm) |
42.626,44 |
42.826.68 |
44.516.06 |
0.003 |
| Ejection fraction (%) |
63[54-71] |
63[54-71] |
64.5[53-73.25] |
0.585 |
| Mitral insufficiency |
50/435 (11.5) |
38/330 (11.5) |
12/105 (11.42) |
1 |
| Congestive heart failure |
19/435 (4.36) |
15/330 (4.54) |
4/105 (3.81) |
1 |
| Hypertension |
196/435(45) |
142/330 (43) |
54/105(51.42) |
0.14 |
| Diabetes |
28/435 (6.43) |
21/330(6.36) |
7/105 (6.66) |
1 |
| Hyperlipidemia |
82/435(18.85) |
59/330 (17.87) |
23/105 (21.9) |
0.39 |
| COPD |
10/435 (2.29) |
5/330 (1.51) |
5/105 (4.76) |
0.066 |
| Thyroid dysfunction |
36/435 (8.27) |
23/330 (6.97) |
13/105 (12.38) |
0.102 |
| Pulmonary embolism |
2/435 (0.46) |
1/330 (0.30) |
1/105 (0.95) |
0.425 |
| Stroke/TIA before enrollment |
24/435 (5.52) |
17/330 (5.15) |
7/105 (6.66) |
0.623 |
| Vascular disease |
18/435 (4.13) |
15/330(4.54) |
3/105(2.85) |
0.581 |
| Smoking |
39/435 (8.96) |
27/330 (8.18) |
12/105 (12.38) |
0.329 |
| Body mass index |
27±4.51 |
26±4.04 |
27±5.71 |
0.264 |
| GFR |
82 [70-90] |
82 [70-90] |
78 [66-90] |
ns |
| CHA2DS2VASC score |
1.231.15 |
1.22 |
1.28 |
0.637 |
| CHA2DS2VASC score 0 |
134/435 (30.8) |
102/330 (30.9) |
32/105 (30.47) |
1 |
| CHA2DS2VASC score 1 |
156/435 (35.86) |
121/330 (36.66) |
35/105 (33.33) |
0.561 |
| CHA2DS2VASC score 2 |
90/435 (20.69) |
68/330 (20.6) |
22/105 (20.9) |
1 |
| CHA2DS2VASC score 3 |
36/435 (8.27) |
25/330 (7.57) |
11/105 (10.47) |
0.415 |
| CHA2DS2VASC score 4 |
13/435 (5.28) |
10/330 (3.03) |
3/105 (2.86) |
1 |
| CHA2DS2VASC score 5 |
4/435 (0.92) |
2/330 (0.6) |
2/105 (1.9) |
0.247 |
| CHA2DS2VASC score 6 |
2/435 (0.45) |
2/330 (0.6) |
0/105 |
1 |
*Pt: patient, † LA: left atrium, ‡ TIA: transient ischemic attack, ∫CHA2DS2VASC: stroke stratification score, ǁ COPD: chronic obstructive pulmonary disease, #GFR: glomerulus filtration rate
Sixty-eight (296/435) percent of general patient cohort had a CB ablation as first procedure, the remaining 22% underwent CA with a radiofrequency RF CA [Table 4]. A higher rate of CB usage was represented in the group A (p=0.004), while in the group A CA was utilized more frequently during the index procedure (p=0.004). There was no significant difference in the radiation and procedure time among the examined groups. Redo ablation overall was performed in 45% of the patients, more often in the group B (58%) compared to the control group (41%) (p=0.003). The mean number of CA for AF per patients was 0.760.74 in the group B (in 42 patients 2 attempts, in 19 patients 3 attempts), while 0.490.66 in the successful group (group A) (in 108 patients 2 attempts, in 24 patients 3 attempts, in 2 patients 4 attempts) (p=0.001). In addition, 23 patients (22%) underwent a His-ablation, while in 29 patients (28%) a MAZE procedure was implemented in the group B. In the group B 39 patients (37%) underwent a PM or CRT implantation after PVI, compared to one patient in the group A (p<0,005).
Of the 435 patients in the general patient cohort, 17 (4%) patients developed stroke/TIA during a mean of 5.8 [5.1-7.3] years of FU. The stroke/TIA incidence rate was 6.15 per 1000 person-years during 2763 person-years of FU in the whole patient population. In the group A 8 (2.4%) patients developed stroke/TIA during 2037 person-year of follow-up (incidence rate 3.92 per 1000 person-years), while in the group B 9 patients developed stroke/TIA during 726 person-year of follow-up (incidence rate 12.4 per 1000 person-years).
The cumulative incidence of stoke/TIA was higher in the group B than in the group A. The crude HR for primary outcome was 2.84 (95% CI 1.078-7.48) in the group B compared with the group A [Table 4].
After adjusting the results for age (per ten years), left atrial size and presence of paroxysmal AF the hazard ratio (HR) was 3.44 (95% CI 1.24-9.54) in the group B. No significant interaction was found between unsuccessful ablation and left atrial size, type of AF (p for interaction =0.38), and age (p for interaction =0.07). Those who had unsuccessful ablation had a 3,4 times higher risk of stroke/TIA during the follow-up period as compared to the control group [Table 5]. The mean time to stroke/TIA occurrence was 5.13 ± 3 vs 4.22 ± 3.1 year in the successful and unsuccessful group. (p=0.55) One out of 17 patients who suffered stroke/TIA during the follow-up was off anticoagulation therapy with CHA2DS2VASC score of 0, and 1 patient with CHA2DS2VASC score of 1 treated with aspirin also suffered a stroke/TIA. All further 15 patients except one had a therapeutic INR level at the time of cerebrovascular event.
Cumulative TIA-alone incidence (3.97, CI 1.10-14.34, p=0.035) such as the annualized TIA-alone incidence rate was significantly higher (6/105 patients) in the group B (8.26 incidence rate per 1000 person-years) as compared to the (4/330 patients) group A (1.96 incidence rate per 1000 person-years) (p=0.029) ([Table 3], [Figure 1]) The mean time to stroke-alone occurrence was 4.48±2.8 year in the group A, and 6.96±2.8 year in the group B (p=0.31). TIA-alone developed after PVI with a mean of 5.81±3.3 vs. 2.84±2.4 year in the successful and unsuccessful group (p=0.144) [Table 2] Neither the mortality rate nor the incidence rate of stroke-alone differed significantly among the groups (Table 3,4,5). One patient died from stroke, while a further one from intracranial bleeding. The residual 14 patients died because of cancerous disease.
Figure 1. Cumulative incidence for the distribution of time to the primary outcome: stroke/TIA (a) and TIA-only (b) in the successful and unsuccessful ablation group. Green line represents the unsuccessful group, blue lines represents the successful group.
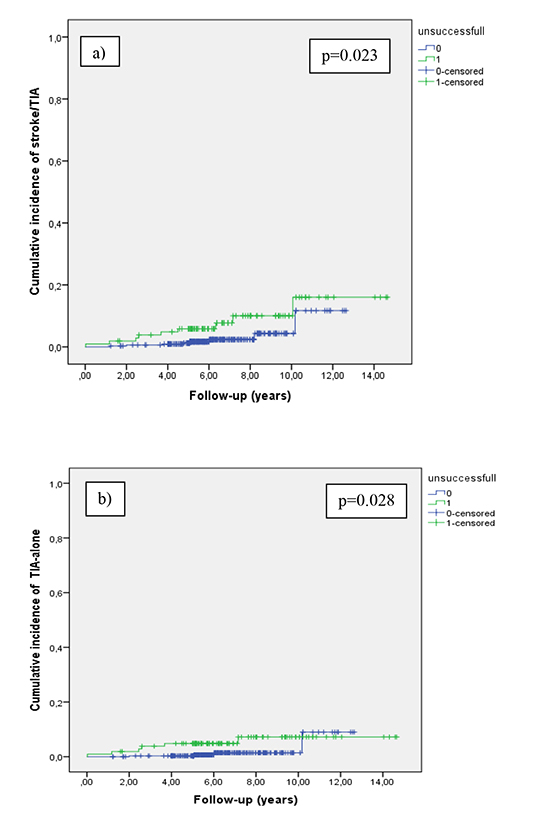
Table 2. Primary, secondary outcome data
|
Total (%)
N=435 |
Pts with successful ablation (%)
N=330 |
Pts with unsuccessful ablation (%)
N=105 |
P-value |
| Primary outcome
-Stoke/TIA after PVI |
17/435 (3.91) |
8/330 (2.42) |
9/105 (8.57) |
0.008 |
| Secondary outcome |
| -Stroke alone after PVI |
7/435 (1.61) |
4/330 (1.21) |
3/105 (2.86) |
0.367 |
| -TIA alone after PVI |
10/435 (2.29) |
4/330 (1.21) |
6/105 (5.71) |
0.015 |
| -All cause-mortality |
16/435 (3.67) |
12/330 (3.64) |
4/105 (3.81) |
1 |
| Event rate |
33/435 (7.35) |
20/330(6.06) |
13/105 (12.38) |
0.033 |
| Intracranial bleeding after PVI |
2/435 (0.45) |
0 |
2/105 (1.9) |
|
| Follow-up period (years) |
5.8 [5.1-7.3] |
5.7 [5.08-6.99] |
6.25 [5.15-8.89] |
0.011 |
| Stroke/TIA occurrence after PVI (year) |
4.65±3.04 |
5.13±3.03 |
4.22±3.16 |
0.556 |
| Stroke occurrence after PVI (year) |
5.54±2.94 |
4.48±2.89 |
6.96±2.83 |
0.310 |
| TIA occurrence after PVI year (year) |
4.03±3.08 |
5.81±3.37 |
2.84±2.46 |
0.144 |
*TIA: transient ischemic attack, †PVI: pulmonary vein isolation
Table 3. Incidence density rates for association between successful and unsuccessful catheter ablation for AF and primary and secondary outcomes
| Study outcome |
Study group |
No. of events |
Follow-up duration (person-years) |
Incidence rate (95% CI) Per 1000 person-years |
P value |
| Primary outcome:
-Stroke/TIA |
Successful
Unsuccessful |
8
9 |
2037
726 |
3.92 (1.82-7.45)
12.4 (0.60-2.275) |
0.021 |
| Secondary outcome: |
| -Stroke alone |
Successful
Unsuccessful |
4
3 |
2037
726 |
1.96 (0.52-5.02)
4.13 (1.05-11.25) |
0.35 |
| -TIA alone |
Successful
Unsuccessful |
4
6 |
2037
726 |
1.96 (0.52-5.02)
8.26 (3.01-17.99) |
0.029 |
| -Mortality |
Successful
Unsuccessful |
12
4 |
2037
726 |
5.89 (3.04-10.29)
5.51 (1.48-14.11) |
0.944 |
*TIA: transient ischemic attack, †CI: confidence interval
To the best of our knowledge, this is the first study comparing the long-term outcome data including stroke/TIA, stroke-alone, TIA-alone, all-cause mortality of patients after failed CA of AF to a control group of those with successful AF ablation. The major finding of this study is that those who had unsuccessful ablation faced a significantly higher rate of stroke/TIA or TIA-alone in comparison to the control group during a 5.8-year of FU. However, we did not find significant difference between the groups in mortality rate.
Comparison to previous studies
Several previous studies investigated the outcome of AF ablation therapy (irrespective of success) compared to antiarrhythmic (regardless of rate of rhythm control) AF management. 8-12 These studies showed that CA for AF was associated with a reduced risk of stroke and mortality in comparison to medical treatment. It was established in the propensity score-matched population-based study by Saliba et al. that even in predominantly high-risk AF patients (with high CHA2DS2VASC score) the ablation therapy significantly lowered the risk of stroke/TIA than did the medical therapy.10 Bunch et al. also provided data on lowered long-term risk of cerebrovascular event in the ablated group compared to non-ablated group.13 The nationwide cohort study by Chang et.al also revealed a reduced incidence of stroke but not of death in comparison between ablation and non-ablation AF management therapy.8 The above mentioned studies investigated mixed patient cohorts to compare the outcome data of ablated vs. non-ablated patients. While, Kochhäuser et al. investigated only those who were free of AF 12 months after PVI.14 They reported that 4 out of 398 patients (1%) suffered from stroke during a median FU of 529 days. Most of the published literature evaluating stroke risk following PVI provides outcome data only with short or mid-term FU. However, it is crucial to highlight that these may underestimate the prevalence of thromboembolic events (TE) after PVI, as we showed that stoke after PVI occurred with a mean of 5.542.94 years, while TIA with a mean of 4.033.06 years.
It is also essential to emphasize that there is a progressive and significant decline in freedom from AF between 1, 3 and 5-year after successful PVI in patients with PAF.7 Although, the rate of decline in freedom from arrhythmia after PVI was reported to be the highest during the first 12 months. Over time a constant decrease in arrhythmia free survival could be detected with a surprisingly high rate of late AF recurrences.7 Subsequently, not only the stroke/TIA occurrence but also the number of patients with failed AF ablation is increasing by time. This phenomenon might derive from the progression of AF and/or from deterioration of co-morbidities, however we cannot exclude the possible role of that patients followed only in tertiary centers remain under less expertized control.
Only few studies reported on thromboembolic event after PVI over 5-years of FU. The study by Tran et al. with 9.1 year of FU following CA of AF reported 7 TE out of 164 pts, with event ratio of 0.41 per 100 patient year.15 Ghanbari et al. evaluated the stroke risk after PVI between patients who remained in sinus rhythm with those who did not with 10-year of FU.16 There were 71 TE and cardiovascular events in 3058 patients (2,3%). They found that prevalence of TE event was similar among patients with persistent (49/1888, 2.6%) and paroxysmal AF (22/1770, 1.9%) (p=0.57). Contrary to this, in our present study the presence of all stroke/TIA with a mean of 5.8 years of FU was 8/330 (2.42%) in the group B vs. 9/105 (8.57%) in the group A (p=0.008).
Furthermore, TIA prevalence was significantly higher in the group A with 6/105 (5.71%) patients as compared to 4/330 (1.21%) patients in the group B (p=0.015)
Postprocedural anticoagulation and thromboembolic stroke risk
Current guidelines recommend that the decision on the-long term post-ablation anticoagulation therapy should be based on the individual stroke risk profile evaluation rather than on the success or failure of ablation. 1,2,17 In present study no significant difference was identified between the stroke profile (CHA2DS2VASC score) of the investigated groups, however significantly higher risk of stroke/TIA was observed in the group A. Because of the observational nature of present study, the cause-effect relationship concept cannot be proven that unsuccessful catheter ablation would increase the postablation risk of stroke. The crucial question whether AF ablation affects the long-term stroke risk should be answered by randomized, controlled clinical trials. Advocating long-term anticoagulation stroke prevention strategies based not only on stroke risk profile but also on the outcome of AF ablation therapy can be discussed, however in the present study majority of the cerebrovascular events occurred with therapeutic INR level in the present study. Based on this observation, further randomized studies are needed to answer whether LAA closure procedures compared to oral anticoagulation management could lower the stroke prevalence in patients after failed AF ablation.
Despite significant technological advances in atrial fibrillation ablation, while being superior to medical therapy, its long-term success still remains lower than ablation for other arrhythmias. Further attempts should be made to improve the long-term success of patient who undergo AF ablation. Nevertheless, it would be of a great interest to apply a more effectual follow-up methodology for those with unsuccessful CA for AF and to follow the effect of the AF ablation therapy over the life course rather than using a short time horizon. The late occurrence of TE events after ablation procedure still remain a key clinical phenomenon especially among those after failed rhythm control strategy. Taking into consideration that in the present study the majority of TE events occurred with therapeutic INR level, the role of novel anticoagulants in preventing these complications late after ablation remains to be investigated. We may assume that in patient with previous stroke/TIA and failed ablation therapy there should be a lower threshold preserved to make the indication for a LAA closure procedure. Furthermore, better understanding of stroke mechanism is necessary.
Table 4. Crude hazard ratio for the association between successful and unsuccessful catheter ablation and primary and secondary outcomes
| Study outcome |
Study group |
Crude HR(95% CI) |
P value |
| Primary outcome:
-Stroke/TIA |
Successful
Unsuccessful |
Reference
2.84 (1.07-7.489) |
0.035 |
| Secondary outcome: |
|
|
|
| -Stroke alone |
Successful
Unsuccessful |
Reference
1.75 (0.38-8.09) |
0.471 |
| -TIA alone |
Successful
Unsuccessful |
Reference
3.97 (1.10-14.34) |
0.035 |
| -Mortality |
Successful
Unsuccessful |
Reference
0.74 (0.23-2.31) |
0.611 |
*CI: confidence interval, †HR: hazard ratio, ‡TIA: transient ischemic attack
Table 5. Adjusted HR for the association between successful and unsuccessful catheter ablation and primary and secondary outcome
| Study outcome |
Adjusted HR (95% CI) |
P value |
| Primary outcome: |
| -Stroke/TIA |
3.44 (1.24-9.54) |
0.018 |
| Secondary outcome: |
| -Stroke alone |
1.86 (0.399-8.67) |
0.429 |
| -TIA alone |
5.79 (1.38-24.25) |
0.016 |
| -Mortality |
0.99 (0.28-3.42) |
0.994 |
*adjusted for left atrial size, age (per ten years) and presence of paroxysmal atrial fibrillation
Our study has several limitations. This is a single-center retrospective study from a large consecutive population that underwent CA for AF. The only inclusion criteria for this AF ablation population was to have a completed long-term follow-up period of 4 years. All other procedural and follow-up methodologies were included, as we used follow-up data provided by peripheral health centers as well. Additionally, no data was available in the large population concerning anticoagulation strategy, compliance to anticoagulation treatment, or physician attitude to follow the anticoagulation management guidelines.
In conclusion, the present study reports on a higher stroke/TIA and TIA-alone incidence with a long-term follow-up in patients with a failed CA for AF as compared to those with successful AF ablation. The use of novel anticoagulants in preventing these complications late after ablation is required to be investigated. We may conclude that in patients with previous stroke/TIA and/or with failed ablation therapy a lower threshold for LAA closure procedure should be practiced. Furthermore, better understanding of atrial fibrillation and stroke mechanism are pivotal. Finally, randomized, controlled trials are warranted to confirm our findings.






