The Characteristics and Clinical Outcomes of Direct Oral Anticoagulantsin Patients with Atrial Fibrillation and Chronic Kidney Disease: From the Database of A Single-Center Registry
Takao Sato1, Yoshifusa Aizawa1, Hitoshi Kitazawa1, Masaaki Okabe1
1Department of Cardiology, Tachikawa General Hospital, Nagaoka, Japan.
This study aimed to evaluate the characteristics and clinical outcomes (major bleeding [MB] and thromboembolic events [TEEs]) of atrial fibrillation (AF) patients with chronic kidney disease (CKD)who receiveddirect oral anticoagulant (DOAC) therapy.
Data prospectivelycollected from a single-center registry containing 2,272 patients with DOAC prescription for AF (apixaban [n=1,014], edoxaban [n=267], rivaroxaban [n=498], and dabigatran[n=493]) were retrospectively analyzed. Patients were monitored for two years and classified into the CKD (n=1460) andnon-CKD groups(n=812). MB and TEEs were evaluated.
The mean age was 72±10 years, with the CHADS2,CHA2DS2-VASc, and HAS-BLED scores being 1.95±1.32, 3.21±1.67, and 1.89±0.96,respectively.Incidence rates of MB and TEEs were 2.3%/year and 2.1%/year, respectively. The CKD groupwasolderand had lower body weight and higher CHADS2,CHA2DS2-VASc, and HAS-BLED scoresthanthe non-CKD group.Kaplan–Meier curve analysis revealed that the incidence of MB and TEEs was higher in the CKD group. Multiple logistic regression analysis in the CKD group revealed thatage andstroke history were independent determinants of TEEs, and low body weighttended to be a determinant of MB.The inappropriate low dose use was higher for apixaban than other DOACs in the CKD group. Consequently, for apixaban, the incidence of stroke was significantly higherin the CKD group than in the non-CKD group.
Patients with CKDwere characterized by factors that predisposed them to MB and TEEs, such as older age and low body weight. In a single-center registry, only treatment with apixaban in the CKD group led to a higher incidence of TEEs.
Key Words : Direct oral anticoagulants, Appropriate dose, Atrial fibrillation, Chronic kidney disease, Major bleeding, Stroke.
Takao Sato, MD
Department of Cardiology, Tachikawa General Hospital
561-1 Jyojyomachi Aza Yauchi Nagaoka City, Japan.
Atrial fibrillation (AF) represents the most frequentlyencountered sustained arrhythmia and has a prevalence rate ranging between1.5–2% in the general population, which increases to 10% and 18% at 80 and 85 years of age, respectively1-3. Direct oral anticoagulant (DOAC) therapy obviates the need for regular laboratory monitoring of patients by international normalized ratio testing owing to a wider therapeutic window, allows once-daily (edoxaban, rivaroxaban) or twice-daily (apixaban, dabigatran) administration and is associated with minimalfood and drug interactions. Regarding safety and efficacy, DOAC therapy has been shown to be superior to vitamin K antagonists in patients with nonvalvular AF, though DOAC equally has the risk of intracranial bleeding 4-7.
Meticulous dose adjustments are not required for DOACs. Nonetheless,considering appropriate dose selection, cut-off values differ according to age, renal function, body weight, and interacting drugs. Both age and chronic kidney disease (CKD)increase the risk of stroke and bleeding during antithrombotic treatmentin patients with AF 8, which might cause the prescription of an inappropriately low dose. In our database of a single-center registry, 23% of patients with AF treated with a DOAC received an inappropriate dose 9.
In addition, patients with CKD are predisposed tocardiac rhythm disorders (e.g., AF and atrialflutter) and carry an increased burden of AF compared with those withoutCKD10. The prevalence rate ofAF remains high and has been estimated to range from 16% to 21% in patients with CKD who are not dependent on dialysis11-13.
This single-center study aimed to evaluate the current status of the characteristics and clinical outcomesof DOAC prescription,including the rate of appropriate dose use,amongpatients with AF and CKD.
Study population and data collection
In total,2,272 consecutive patients who were prescribedDOACs for AF (including paroxysmal AF)between September 2011 and January 2016 at Tachikawa General Hospital, Nagaoka, Japan, were retrospectively analyzed. All patients in the DOAC database were included in the analysis. However, patients with (1) valvular disease requiring surgery, (2) prosthetic mechanical heart valve, and (3) mitral stenosis were excluded from the study.
Data on patients’ baseline characteristics including age, sex, body weight, and renal function (creatinine clearance and creatinine levels); history, including comorbidities; and clinical outcomes during 2-year follow-up after DOAC prescription were collected. Furthermore, CHADS2 score, CHA2DS2-VASc score, and HAS-BLED score were determined 14-16. The institutional database used in this study was approved by our local ethics committee, and informed consent was obtained from all patients.
Four DOACs (apixaban [n=1,014], edoxaban [n=267], rivaroxaban [n=498], and dabigatran [n=493]) were prescribed for AF at the discretion of the physician. The prescription dose was basically in accordance with themanufacturer’s label recommendations in Japan, including thereduced dose recommendations.For apixaban, a reduced dose is recommended for patients with at least two of the following characteristics: age ≥80 years, weight ≤60kg, or serum creatinine level ≥1.5mg/dL.For edoxaban, a reduced dose is recommended for patients with moderate or severe renal impairment (creatinine clearance of 15–49 mL/min), patients weighing ≤60 kg, and patients being concomitantly treated with interacting drugs (e.g., verapamil). For rivaroxaban, a reduced dose is recommended for patients with moderate renal impairment (creatinine clearance of 15–49mL/min). For dabigatran, a reduced dose is consideredfor elderly patients aged ≥70 years, patients with moderate renal impairment (creatinine clearance of 30–49mL/min), patients concomitantly treated with interacting drugs (e.g., verapamil), and patients at a high risk ofbleeding. However, an inappropriately high or low dose may similarly be prescribed based on the doctor's discretion. Hence, in this study, classifications of DOAC prescriptions, including an appropriate dose and an inappropriate high or low dose, were considered based on the manufacturer’s label recommendations in Japan, as mentioned earlier.
In this study, patients were classified into the following two groups according to a cut-off value of 50 mL/min for creatinine clearance at registration: non-CKD group (n=1460) and CKD group (n=812). A comparison of baseline characteristics, the ratio of the appropriate dose useto the inappropriate dose use, including an inappropriate low dose, andclinical outcomesbetween the two groupswere determinedfor all four DOACs and each type ofDOAC. In this study, if the types of DOAC were changed or the DOAC was discontinued, the patients were excluded from the cohorts but included in the data analysis.
The primary outcome was stroke, including transient ischemic attacks (TIA) and hemorrhagic stroke and systemic embolism.The main safety outcome was major bleeding, defined using the Randomized Evaluation of Long-Term Anticoagulant Therapy criteria 5, 10.Furthermore, the rate of any cause of death was determined.
Normally distributed continuous data are presented as means ± standard deviations, whereas categorical data are expressed as counts with percentages. Non-parametric data, such as CHADS2 score, CHA2DS2-VASc score, and HAS-BLED score, are presented as median value (interquartile range). For all four DOACs, baseline characteristics were compared usinganalysis of variance (followed by multiple comparisons using Dunn’s method)for parametric data and the chi-squared test for categorical data.For each type of DOACs, baseline characteristics of the non-CKD and CKD groupswere compared using Student’s t-testand Fisher’s exact test for continuous-and categorical data, respectively. Furthermore, multivariate logistic regression was performed to determine the predictors for major bleeding and stroke in both non-CKD and CKD groups. Finally, we compared the clinical outcomes between the non-CKD andCKD groups using Kaplan–Meier event rate curves.A two-sided p-value <0.05 was considered statistically significant for all analyses.
In this study, the mean age of patients was 72±10 years, with CHADS>2, CHA2DS2-VASc, and HAS-BLED scoresof 1.95±1.32, 3.21±1.67, and 1.89±0.96, respectively. The mean follow-up time was 1.6 years. Overall, the incidence rates of major bleeding and thromboembolic events were 2.3 and 2.1 per 100patient-years, respectively.
Table 1. The comparison between CKD group and non-CKD group
|
All |
CKD |
Non-CKD group |
P value CKD vs Non-CKD |
| N |
2272 |
812 |
1460 |
- |
| Age (years) |
72.3±7.2 |
80.8±6.6 |
67.6±9.9 |
<0.01 |
| Male (%) |
63 |
49 |
72 |
<0.01 |
| Body-weight (kg) |
59.4±13.1 |
50.6±9.7 |
64.3±11.5 |
<0.01 |
| Ccr (mL/min) |
61.6±24.2 |
39.3±8.4 |
74.2±21.2 |
<0.01 |
| History |
| of CAD |
214 (9.4) |
91(11.2) |
123(8.4) |
0.10 |
| of PAD |
75 (3.3) |
23(2.8) |
52(3.5) |
0.41 |
| of CHF |
411 (18.1) |
240 (29.5) |
171 (11.7) |
<0.01 |
| of diabetes |
451(19.8) |
165(20.3) |
286(19.5) |
0.41 |
| of hypertension |
1264 (55.6) |
463(57.1) |
801(54.8) |
0.07 |
| of stroke or TIA |
338 (14.8) |
132(16.2) |
206(14.1) |
0.35 |
| of intracranial bleeding |
43 (1.9) |
13(1.6) |
30(2.0) |
0.59 |
| of GI bleeding |
40 (1.8) |
19(2.3) |
21(1.4) |
0.13 |
| of anti-platelet therapy |
304 (13.3) |
109(15.0) |
195(13.3) |
0.50 |
| Appropriate dose (%) |
77.4 |
85.7 |
72.9 |
<0.01 |
| CHADS2 score |
|
|
|
<0.01 |
| 0 |
258 (11.3) |
20 (2.4) |
238 (16.3) |
|
| 1 |
683 (30.0) |
128(15.8) |
555 (38.0) |
|
| ≥2 |
1331(58.5) |
664(81.8) |
667(45.7) |
|
| Mean |
1.95±1.32 |
2.57±1.23 |
1.61±1.20 |
|
| CHA2DS2-VASc score |
|
|
|
<0.01 |
| 0 |
75 (3.3) |
3 (0.4) |
72 (4.9) |
|
| 1 |
310 (13.7) |
13 (1.6) |
297 (20.4) |
|
| 2 |
414 (18.2) |
74 (9.1) |
340 (23.3) |
|
| ≥3 |
1473 (64.8) |
722 (88.9) |
751 (51.4) |
|
| mean |
3.21±1.67 |
4.19±1.45 |
2.67±1.67 |
|
| HAS-BLED score |
|
|
|
<0.01 |
| 0 |
154 (6.8) |
4 (0.5) |
150 (10.2) |
|
| 1 |
599 (26.3) |
15 (1.8) |
584 (40.0) |
|
| ≥2 |
1519 (66.8) |
793 (97.7) |
726 (49.7) |
|
| mean |
1.89±0.96 |
2.18±0.83 |
1.71±0.97 |
|
| Any cause death
(per 100-patient years) |
2.1 |
4.5 |
1.1 |
<0.01 |
| Major bleeding
(per 100-patient years) |
2.3 |
3.3 |
1.4 |
<0.01 |
| Intracranial hemorrhage |
0.3 |
0.2 |
0.3 |
|
| Gastrointestinal bleeding |
1.9 |
3.1 |
1.0 |
|
| Stroke/emboli (per 100-patient years) |
2.1 |
3.6 |
1.6 |
<0.01 |
| Ischemic strokes |
1.8 |
3.0 |
1.4 |
|
| TIA |
0.1 |
0.2 |
0.1 |
|
| Systemic emboli |
0.1 |
0.2 |
0.0 |
|
| Hemorrhagic stroke |
0.1 |
0.2 |
0.1 |
|
Data are presented as the mean ± standard deviation or n (%). Ccr, Creatinine clearance; CAD, coronary artery disease; PAD, peripheral artery disease; CHF, congestive heart failure; TIA, transient ischemia attack; CHADS2 score, Congestive Heart Failure, Hypertension, Age ≥ 75 Years, Diabetes Mellitus, Stroke History; CHA2DS2-VASc score, Congestive heart failure, Hypertension, Age≥75 years, Diabetes Mellitus, Previous Stroke/transient ischemic attack, Vascular disease, Age 65-74 years, Sex category;HAS-BLED score, Hypertension, Renal Disease and Liver Disease, Stroke History, Prior Major Bleeding or Predisposition to Bleeding, Age >65, Medication Usage Predisposing to Bleeding score
Comparison of baseline characteristics between the non-CKD and CKD groups for all four DOACs and for each type of DOACs ([Table 1] and [Table 2])
Table 2. The comparison of CKD group and non-CKD group in each DOAC (a) Apixaban
|
CKD |
Non-CKD |
P value |
| N |
388 (38.3) |
626 (61.7) |
|
| Age (years) |
81.9±6.3 |
69.6±9.9 |
<0.01 |
| Male (%) |
48 |
71 |
<0.01 |
| Appropitate dose (%) |
79.8 |
75.2 |
0.38 |
| Body-weight (kg) |
50.6±9.9 |
63.0±11.4 |
<0.01 |
| Ccr (ml/min) |
38.5±7.6 |
72.2±19.2 |
<0.01 |
| CHADS2 score |
2.57±1.23 |
1.62±1.27 |
<0.01 |
| CHA2DS2-VASc score |
4.26±1.41 |
2.77±1.62 |
<0.01 |
| HAS-BLED score |
2.12±0.80 |
1.75±0.98 |
0.01 |
| Any cause death
(per 100-patient years) |
5.5 |
1.9 |
<0.01 |
| Major bleeding
(per 100-patient years) |
3.9 |
2.3 |
0.21 |
| Stroke/systemic emboli
(per 100-patient years) |
3.81.6 |
1.6 |
0.03 |
Data are presented as the mean ± standard deviation or n (%). Ccr, Creatinine clearance; CHADS2 score, Congestive Heart Failure, Hypertension, Age ≥ 75 Years, Diabetes Mellitus, Stroke History; CHA2DS2-VASc score, Congestive heart failure, Hypertension, Age≥75 years, Diabetes Mellitus, Previous Stroke/transient ischemic attack, Vascular disease, Age 65-74 years, Sex category; HASBLED score, Hypertension, Renal Disease and Liver Disease, Stroke History, Prior Major Bleeding or Predisposition to Bleeding, Age >65, Medication Usage Predisposing to Bleeding score
Table 2. (b) Edoxaban
|
CKD |
Non-CKD |
P value |
| N |
107 (40.0) |
160 (60.0) |
|
| Age (years) |
80.1±6.9 |
67.6±8.5 |
<0.01 |
| Male (%) |
44 |
73 |
<0.01 |
| Appropriate dose (%) |
91.5 |
83.8 |
0.25 |
| Body-weight (kg) |
50.1±8.8 |
63.0±10.3 |
<0.01 |
| Ccr (ml/min) |
36.9±9.9 |
73.0±16.0 |
<0.01 |
| CHADS2 score |
2.39±1.26 |
1.69±1.03 |
<0.01 |
| CHA2DS2-VASc score |
4.02±1.60 |
2.69±1.57 |
<0.01 |
| HAS-BLED score |
2.15±0.93 |
1.67±0.99 |
<0.01 |
| Any cause death
(per 100-patient years) |
1.5 |
0.0 |
0.58 |
| Major bleeding
(per 100-patient years) |
3.5 |
1.8 |
0.36 |
| Stroke/systemic emboli (per 100-patient years) |
0.0 |
1.8 |
0.51 |
Table 2. (c): Rivaroxaban
|
CKD |
Non-CKD |
P value |
| N |
177 (35.6) |
321 (64.4) |
|
| Age (years) |
80.5±6.7 |
67.0±10.3 |
<0.01 |
| Male (%) |
48 |
75 |
<0.01 |
| Appropriate dose (%) |
89.8 |
64.2 |
<0.01 |
| Body-weight (kg) |
51.1±9.9 |
66.2±11.5 |
<0.01 |
| Ccr (ml/min) |
39.1±8.5 |
76.0±20.4 |
<0.01 |
| CHADS2 score |
2.54±1.25 |
1.61±1.10 |
<0.01 |
| CHA2DS2-VASc score |
4.14±1.45 |
2.65±1.42 |
<0.01 |
| HAS-BLED score |
2.20±0.76 |
1.75±0.99 |
<0.01 |
| Any cause death
(per 100-patient years) |
4.5 |
1.0 |
0.024 |
| Major bleeding
(per 100-patient years) |
2.2 |
0.6 |
0.14 |
| Stroke/systemic emboli
(per 100-patient years) |
3.2 |
1.4 |
0.78 |
Table 2. (d) Dabigatran
|
CKD |
Non-CKD |
P value |
| N |
140(28.3) |
353(71.7) |
|
| Age (years) |
79.1±6.9 |
66.1±9.5 |
<0.01 |
| Male (%) |
54 |
72 |
<0.01 |
| Appropriate dose (%) |
93.6 |
72.6 |
<0.01 |
| Body-weight (kg) |
50.2±9.1 |
63.0±10.3 |
<0.01 |
| Ccr (ml/min) |
40.4±7.3 |
77.9±26.0 |
<0.01 |
| CHADS2 score |
2.58±1.35 |
1.57±1.13 |
<0.01 |
| CHA2DS2-VASc score |
4.11±1.51 |
2.52±1.47 |
<0.01 |
| HAS-BLED score |
2.24±0.96 |
1.63±0.94 |
<0.01 |
| Any cause death
(per 100-patient years) |
0.6 |
0.1 |
0.45 |
| Major bleeding
(per 100-patient years) |
2.5 |
1.4 |
0.48 |
| Stroke/systemic emboli
(per 100-patient years) |
3.8 |
1.7 |
0.23 |
Overall, the CKD group had significantly higher mean age and CHADS2,CHA2DS2-VASc, and HAS-BLED scores than the non-CKD group. Nevertheless, body weight was significantly lowerin the CKD groupthan in the non-CKD group. In our database of a single-center registry, 23% of patients with AF treated with a DOAC received an inappropriate dose.Regardingthe analysis of inappropriate dose use, the use of inappropriate low dose was obviously dominant compared to the use of inappropriate high dose (94.4 vs. 5.6%) [Table 3(a)]. On the contrary, the ratio of appropriatedose use was significantly higher in the CKD group than in the non-CKD group (85.7 vs.72.9%, p<0.01).
Table 3(a). The prescription among four DOACs.
| (a)The rate of appropriate dosing among four DOACs |
|
Apixaban |
Edoxaban |
Rivaroxaban |
Dabigatran |
| Appropriate dose(%) |
781 (77.1) |
230 (86.1) |
364 (73.0) |
385 (78.1) |
| Inappropriate dose |
|
|
|
|
| Low dose (%) |
229 (22.5) |
33 (12.4) |
119 (23.9) |
102 (20.7) |
| High dose (%) |
4 (0.4) |
4 (1.5) |
15 (3.1) |
6 (1.2) |
| (b) The comparison of the rate of appropriate dosing between the CKD and non-
CKD among four DOACs |
|
Apixaban |
Edoxaban |
Rivaroxaban |
Dabigatran |
P value |
| CKD (%) |
79.8* |
91.5 |
89.8 |
93.6 |
<0.01 |
| non-CKD (%) |
75.2 |
83.8† |
64.2 |
72.6 |
<0.01 |
| P value |
0.38 |
0.25 |
<0.01 |
<0.01 |
|
CKD, chronic kidney disease.
However, the ratio of appropriate dose usein the CKD group was significantly lower for apixaban than other DOACs [Table 3(b)]. In contrast, the ratio of appropriate dose use in the non-CKD group was significantly higher for edoxaban thanfor other DOACs. Based on the definition of CKD in this study, creatinine clearance was significantly lower in the CKD group than in the non-CKD group (39.3±8.4 vs. 74.2±21.2 mL/min, p<0.01).
Regardingeach type of DOAC, a similar tendency was observed in the comparison of baseline characteristics between the CKD and non-CKD groups—i.e., significantlyhigher values for mean age, appropriate dose use, and CHADS2, CHA2DS2-VASc, and HAS-BLED scores in the CKD group and significantly lower body weight in the CKD group. However, for apixaban, the ratio of appropriate dose use in the CKD group was comparable to that in the non-CKD group (79.8 vs.75.2%, p=0.38).
Comparison of clinical outcomes between the non-CKD and CKD groupsfor all four DOACs and for each type of DOACs ([Table 1] and [Table 2])
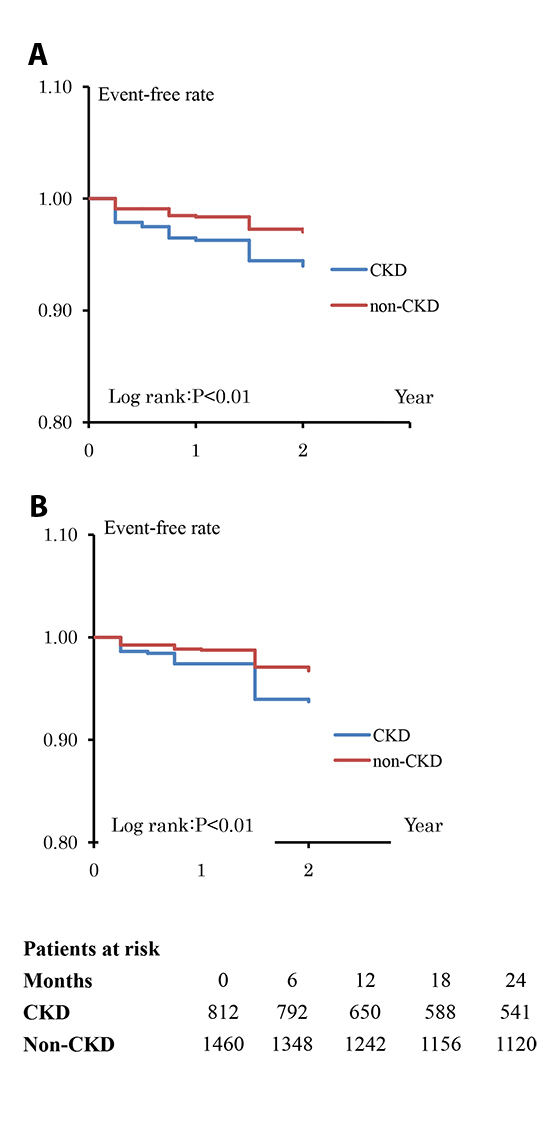
Overall, the CKD group showed significantly higher incidence rates of death from any cause, including major bleeding and stroke/systemic embolism,than the non-CKD group (death from any cause: 4.5 vs. 1.1 per 100patient-years, p<0.01; major bleeding: 3.3 vs.1.4 per 100patient-years, p<0.01; stroke/systemic embolism:3.6 vs. 1.6 per 100patient-years, p<0.01). The Kaplan–Meier event rate curves indicated that major bleeding and stroke/systemic embolism werefrequentlyobserved in the CKD group [Figure 1]. In addition, multiple logistic regression analysis was performed inboth groups.In the CKD group, age and previous stroke history were independent determinants of stroke/systemic embolism, and low body weight had a tendency to be a determinant of major bleeding [Table 4A].On the contrary, in the non-CKD group, age and prior stroke history were independent determinants of stroke/systemic embolism, and ageand prior bleeding history tended to be determinants of major bleeding [Table 4B]. Concerningeach type of DOAC, for all DOACs excludingapixaban, the incidence rates of major bleeding and stroke/systemic embolism in the non-CKD group were comparable to those in the CKD group. In contrast, for apixaban, the incidence rate of stroke/systemic embolism tended to be higher in the CKD group than in the non-CKD group (3.8 vs. 1.6 per 100patient-years, p=0.03).
Table 4A. Multivariate logistics analysis
| A) non-CKD group |
| (1) A predictor for major bleeding in the non-CKD patients |
|
Odds ratio |
95% confidence interval |
P value |
| Age (years) |
1.04 |
0.99-1.10 |
0.08 |
| Male |
1.46 |
0.48-2.57 |
0.43 |
| Appropriate dose use |
0.64 |
0.33-6.74 |
0.16 |
| Body weight (kg) |
0.98 |
0.90-1.00 |
0.62 |
| Ccr (ml/min) |
0.99 |
0.92-1.01 |
0.85 |
| Antiplatelet therapy |
0.82 |
0.30-2.97 |
0.70 |
| Prior history of bleeding |
2.40 |
0.99-5.11 |
0.06 |
| Prior history of stroke |
2.16 |
0.85-6.76 |
0.11 |
| (2) A predictor for stroke/systemic emboli in the non-CKD patients |
|
Odds ratio |
95% confidence interval |
P value |
| Age (years) |
1.06 |
1.01-1.11 |
0.02 |
| Male |
1.43 |
0.59-3.46 |
0.41 |
| Appropriate dose use |
0.76 |
0.37-1.54 |
0.45 |
| Body weight (kg) |
1.00 |
0.96-1.04 |
0.65 |
| Ccr (ml/min) |
0.98 |
0.95-1.01 |
0.42 |
| Antiplatelet therapy |
1.71 |
0.80-3.63 |
0.16 |
| Prior history of bleeding |
0.26 |
0.03-2.00 |
0.19 |
| Prior history of stroke |
2.77 |
1.15-6.73 |
0.02 |
| (1) A predictor for major bleeding in the CKD patients |
|
Odds ratio |
95% confidence interval |
P value |
| Age (years) |
1.02 |
0.94-1.08 |
0.76 |
| Male |
1.11 |
0.48-2.57 |
0.80 |
| Appropriate dose use |
1.51 |
0.33-6.74 |
0.58 |
| Body weight (kg) |
0.95 |
0.90-1.00 |
0.08 |
| Ccr (ml/min) |
0.97 |
0.92-1.01 |
0.14 |
| Antiplatelet therapy |
1.06 |
0.38-2.97 |
0.90 |
| Prior history of bleeding |
0.89 |
0.24-3.17 |
0.85 |
| Prior history of stroke |
1.13 |
0.45-2.80 |
0.78 |
| (2) A predictor for stroke/systemic emboli in the CKD patients |
|
Odds ratio |
95% confidence interval |
P value |
| Age (years) |
1.08 |
1.01-1.16 |
0.02 |
| Male |
0.89 |
0.36-2.15 |
0.80 |
| Appropriate dose use |
1.23 |
0.33-4.59 |
0.75 |
| Body weight (kg) |
1.02 |
0.97-1.07 |
0.37 |
| Ccr (ml/min) |
1.00 |
0.95-1.05 |
0.87 |
| Antiplatelet therapy |
1.97 |
0.78-4.96 |
0.14 |
| Prior history of bleeding |
1.71 |
0.54-5.43 |
0.35 |
| Prior history of stroke |
2.32 |
1.01-5.13 |
0.04 |
Ccr, creatinine clearance.
Figure 1. (A) Kaplan Meier curve for major bleeding between the chronic kidney disease (CKD) group and the non-CKD group The incidence of major bleeding in the CKD group was significantly higherthan that in the non-CKD group (Logrank: p<0.01). (B) Kaplan Meier curve for stroke/systemic emboli between the CKD group and the non-CKD group The incidence of stroke/systemic emboli in the CKD group was significantly higher than that in the non-CKD group (Logrank: p<0.01).
The major findings of this study were as follows:(1) The incidence of major bleeding and stroke/systemic embolismwas higher in patients with CKD than in those without CKD.(2) Multivariate analyses revealed that low body weight tended to be a predictor of major bleeding, whereas age was a predictor of stroke/systemic embolism in the CKD group.(3) Only patients with CKD on apixaban treatment had a significantly higher incidence of stroke/systemic embolism than those without CKD.
The relationship among AF, CKD, age, and body weight
Severalstudies have reported a substantial relationship amongAF, CKD, age, and body weight (1-3, 10, 17-19), andolder age is associated with the occurrence of AF 1-3.CKD and AF share numerous risk factors and conditionsthat promote their incidence.Therefore, it is established that CKD increases the incidence of AF10, 19.In contrast,AF elimination by catheter ablation was associated with improvement in renal function at 1-year follow-up in patients with mild to moderate renal dysfunction 20, indicating that AF equallyaccelerates CKD progression.
Similarly, a relationship between age and CKD has been reported 21. The absolute glomerular filtration rate (GFR) value decreased with an increase in age20. Furthermore, Japanese patients with AF are generally small and lean22.According to a previous report, frailty in elderly patients increased with an increase in age 23. Body loss has equallybeen defined as one of the criteria for frailty24. Thus, there seems to be a relationship amongCKD, age, and bodyweight somewhat, and we have to consider that AF patients with CKD tend to be olderand have lower body weight. In this study, AF patients with CKD were older and had lower body weight than those without, which isconsistentwith the findings of the aforementioned studies.
Effect of CKD, age, and body weight on major bleeding and stroke/systemic embolism in patients with AF
Several reports have described the association between renal function and major bleeding or stroke/systemic embolism(10, 25-32). In addition, older age is considered a predictor of major bleeding events33, 34 and stroke/systemic embolism33, 35, 36. In addition, it is actually included as one of the factors forthe CHADS2, CHA2DS2-VASc, and HAS-BLED scores. In this study, age was an independent predictor of stroke/systemic embolism, agreeingwith the abovementioned finding.Low body weight tended to be a predictor of major bleeding in this study. Nevertheless,the relationship between body weight and major bleeding remainsfairly controversial37-40. However, several studies have described that lean patients were at higher risk for bleeding complications 41-44. DOACs seemed safer and more effective than vitamin K antagonists, even in patients with low body weight 45. However,the risk of increased bleeding by DOACsin underweight patients has been highlighted in previous studies46, 47.In summary, high age and low body weight, which are specific characteristics of patients with CKD, may be closely associated with an increase in major bleeding or stroke/systemic embolism.
Several previous reports have described thata combination of vitamin K antagonist and antiplatelet therapy is associated with a high annual risk of fatal and non-fatal bleeding episodes 48, 49. However, an observational study on real-world Asian patients treated with DOAC and antiplatelet agents showed no incremental bleeding risk (of additional antiplatelet therapy to DOAC) in a large pooled population50. Therefore, our study findings may be compatible with previous results.
Use of inappropriate low dose in patients with CKD
For apixaban, the incidence of stroke was higher in AF patients with CKD than in those without CKD in the present registry, andthis finding might be very suggestive. The prescription of an inappropriate low dose is often observed in the realworld. Theoretically, an inappropriate low dose might lead to increased safety but decreased effectiveness 51.
The renal clearance ratio of apixaban is approximately 25% 52. Asub-analysis of ARISTOTLE trial datarevealed that treatment with apixaban led to an apparent reduction in the incidence of major bleeding in patients with creatinine clearance <50mL/min compared to treatment with vitamin K antagonists. Thus, apixaban prescription might be logicallyeffective in patients with CKD. However, the use of appropriate apixaban dose was significantly lower in the present registry. This is probably because patients with CKDhave been reported to be predisposed to major bleeding,as mentionedearlier; additionally, themanufacturer’s label recommendations for the reduceddose of apixaban (at least two of the following characteristics: age ≥80 years, weight ≤60kg, or serum creatinine level ≥1.5mg/dL) are more intricate than those for other DOACs. In addition, the reduced dose of apixaban is one-half the standard dose (2.5 mg vs. 5 mg). In contrast, the reduced dose of rivaroxaban and dabigatran approximately rangesbetween 70-75% of the standard dose (15 mg vs. 20 mg and 110mg vs.220mg, respectively). Furthermore, the number of patients in the low-dose DOAC groups of the ARISTOTLE trials was not sufficientenough to establish superiority, equivalence, or non-inferiority 53. Though speculative, there might be an association between dose regimens and medication compliance. A systemic review described that the prescribed number of doses per day was inversely related to compliance 54.
These findings could explain the possible increase in the incidence of stroke/systemic embolism byan inappropriate low dose of apixaban55,56.The difference in inappropriate low dose among the four DOACs might have influenced the resultsof this study;nonetheless, there was low statistical power for the evaluation of the effects of inappropriate low dose on clinical outcomes. Therefore, future studies involving larger populations with long-term follow-up will be needed.
This study has several limitations. First, although this study was retrospective in design, data on clinical outcomes, including those at 2-year follow-up interval, were prospectively collected from all patients. However, propensity score matching was not adopted because the number of patients greatly varied for the four DOACs.Therefore, the impact of renal function on clinical events remains unclear. However, themain objective of this study was to reveal the characteristics of AF patients with CKD. Second, because this study wasretrospective, clinical events, such as minor bleeding, might not have beencompletelydetected. Third, the number of patients with CKD was small. In addition, the definition of CKD involvestwo important factors:estimated-GFR (e-GFR)and proteinuria. However, in this study, because proteinuria data were unavailable due to the retrospective design, and the creatinine clearanceratehas been applied as the index of renal functionin the prescription of most DOACs, thecreatinine clearance ratewas exclusively adopted in this study. The impact of CKD on the clinical outcomes should have beenanalyzed, considering both e-GFR and proteinuria.Fourth, in this study, CKD was defined as a creatinine clearance of less than 50mL/min. According to thisdefinition,all CKD patients taking dabigatran, rivaroxaban, and edoxaban metthe appropriate low dose criteria. On the contrary, some CKD patients taking apixaban did not meet the appropriate low dose criteria, which may have been due to the biased protocol. However, this study aimed to evaluate the current status of the characteristics and clinical outcome of DOAC prescription, including the rate of use of appropriate doses among patients with AF and CKD.Therefore, these limitationswarrant future studies involving larger populations with long-term follow-up.
Patients with CKD were characterized by factors that predisposed them to major bleeding and thromboembolic events, such as older age and low body weight. In a single-center registry, only treatment with apixaban in the CKD group led toa higherincidence of thromboembolic events, indicating the importance of the use of an appropriate dose.






