Posterior Wall Isolation for Atrial Fibrillation: Effects on Echocardiographic Parameters of cardiac function
Xin Zhang, Neil Beri, Pankaj Malhotra, Rakhee Makhija, Eric Nordsieck, Adam Oesterle, Dali Fan, Nayereh Pezeshkian, Uma Srivatsa
Division of Cardiovascular Medicine, UC Davis, Sacramento, CA.
Posterior wall isolation (PWI) in addition to circumferential pulmonary vein isolation (CPVA) requires more ablation of left atrial tissue. We compared the effect of PWI versus non-PWI methods (CPVA + linear lesions) on echocardiographic parameters of left atrial and left ventricular function.
We selected patients who had pre and post ablation echocardiogram at our institution. Parameters assessed were: Left ventricular outflow tract velocity time integral (VTI), left ventricular ejection fraction (LVEF), atrial Doppler velocity across mitral valve (A), E/E’, and deceleration time.
Of the 72 patients studied, 32.5% had PWA in addition to CPVA. The mean duration between echocardiograms was 650 + 542 days. PWA group had an average postoperative VTI 0.21 + 0.05 vs 0.21 + 0.05 in the non-PWA (p=0.61) group. Average improvement compared to pre ablation parameters: VTI was 0.03 + 0.06 vs 0.008 + 0.05 (p=0.17), postoperative A was 0.49 + 0.19 vs 0.57 + 0.19 (p=0.16), postoperative LVEF was 57.5 + 9.9% vs 57.8 + 10.8 % (p=0.89), with average change in LVEF 1.5 ± 7.8 vs 0.86 ± 9.7 (p=0.78) in PWA and non-PWA groups respectively. There was no significant difference in change in deceleration time or E/E’ when comparing the two groups.
PWA did not adversely affect echocardiographic parameters of left atrial function or left ventricular systolic or diastolic function when compared to other types of ablation.
Key Words : Atrial fibrillation posterior wall ablation echocardiogram.
Uma Srivatsa, MBBS, MAS, FACC, FHRS
Division of Cardiovascular Medicine
Department of Internal Medicine
UC Davis School of Medicine
Catheter ablation is a safe and effective treatment strategy for drug refractory persistent atrial fibrillation (AF) 1. Circumferential pulmonary vein ablation (CPVA) is the standard initial approach to catheter ablation of all patients with AF, and comparative results have been obtained with both radiofrequency (RF) point by point ablation and cryoballoon 2. However, patients with persistent AF often require more extensive ablation [3]. One such strategy is posterior wall isolation (PWI) 3. This can be achieved endocardially with a radiofrequency (RF) box lesion set 4, through a hybrid endocardial/epicardial surgical approach 5, as well as with the second generation cryoballoon catheter 6. While PWI has been more adopted in recent years with demonstrable improved durability and efficacy for patients with persistent AF compared to CPVA alone, it also involves significantly more extensive ablation of left atrial tissue 7.
The left atrium plays a critical role in normal cardiac hemodynamics, and absence of atrial systole has been shown to reduce overall left ventricular ejection fraction by anywhere from 20-30% 8. Extensive ablation has been demonstrated to worsen left atrial function more than CPVA alone 9, and there have been computational models which show that wider areas of ablation are inversely associated with both left atrial and left ventricular function 10. There have also been surgical studies that have observed worsening left atrial mechanical function after the Cox-Maze IV procedure 11. On the other hand, the effect of AF on deleterious atrial remodeling has been well described, as well as reversal of this remodeling with successful catheter ablation 1213. The overall effect of the more extensive ablation set with PWA on left ventricular and atrial function remains unclear. In this study, we compared patients who underwent PWI via either hybrid endocardial/epicardial surgical approach or cryoballoon to those who underwent conventional endocardial ablation of CPVA with or without linear lines.
After approval from our Institutional Review Board, we evaluated 168 patients who underwent ablation at our institution for early persistent (7 days- 3 months), persistent (3-12 months) and long -standing persistent AF (> 12 months). Our posterior wall (PW) group included patients that underwent ablation with either cryoballoon or through a hybrid surgical endocardial/epicardial approach. Our non-posterior wall (NPW) group included patients that underwent CPVA with RF or cryoballoon, both with and without the addition of linear roof and/or mitral isthmus lines.
Baseline demographic, characteristic, and echo data were obtained through chart review. We evaluated and compared pre and post ablation echocardiographic markers of left atrial and left ventricular function including mitral inflow “A” velocity, left ventricular outflow tract (LVOT) velocity time integral (VTI), and ejection fraction. Mitral A velocity was obtainable only in patients with sinus rhythm due to lack of atrial systole during atrial fibrillation.
STATA 13.1 was used for all statistical analyses. Continuous variables are expressed as mean + SD or SE; categorical variables are presented as percentages, comparisons were performed with t-test and χ2 test respectively. P-values of 0.05 and below were considered significant.
Seventy two patients (mean age 67 + 8 yrs, male 58.4%, BMI 31 + 6, hypertension 72%, diabetes 25%, heart failure 22%, cardiovascular disease 33%, CHADS2VASC score 2.7 + 1.4) had both pre and post ablation echocardiograms available for review in our EMR in the time frame elaborated in methods section. Twenty-nine were in our PW group, of which seven had undergone hybrid surgical ablation and 22 had cryoballoon ablation. In the NPW group, nine patients underwent CPVA plus linear lines (mitral isthmus and/or roof isolation), four underwent CPVA alone with cryoballoon, and the remaining 30 patients underwent CPVA alone with RF. Mean duration between echocardiographic evaluations was 650 ± 543 days. Echocardiograms were performed 254±305 days before ablation, and 419 ± 431 days after ablation.
Preablation rhythm at time of echocardiogram was sinus for 3/22 (13.6%) patients in the PW group compared to 27/48 (56.25%) in the NPW group (p=0.001). Baseline characteristic data are listed in [Table 1]. Patients who had PWI had a higher BMI (32.8 ± 6.9 versus 30.0 ± 5.3, p=0.05). They also had more obstructive sleep apnea (34.5% vs 14.0%; p=0.04) and heart failure (34.5% vs 14.0%; p=0.04). There were more persistent AF (24.1%) patients in the PW group compared to 27/43 (62.8%) in the NPW group (p=0.001). At the time of post ablation echocardiography, 26/29 patients (89.7%) were in sinus rhythm in the PW group compared to 34/43 (79.1%) in the NPW group (ns). After a year of follow up, with or without antiarrhythmic drugs, 19% in PW and 17.6% in NPW group with persistent and long standing persistent AF had recurrence of AF; 4.7% and 31.2 % of the respective groups with early persistent AF had recurrence of AF.
Table 1. Baseline characteristics
| Variable |
Total (n=72) |
PWI (n=29) |
Non-PWI (n=43) |
p-value |
| Age, y |
66.8 ± 8.3 |
68.1 ± 8.8 |
65.9 ± 7.8 |
0.26 |
| Gender, females (%) |
30 (41.7%) |
10 (34.5%) |
20 (46.5%) |
0.31 |
| BMI |
31.1 ± 6.1 |
32.8 ± 6.9 |
30.0 ± 5.3 |
0.05 |
| HTN |
52 (72.2%) |
22 (75.9%) |
30 (69.8%) |
0.57 |
| DM-II |
18 (25%) |
7 (24.1%) |
11 (25.6%) |
0.89 |
| CAD/PAD |
24 (33.3%) |
11 (37.9%) |
13 (30.2%) |
0.50 |
| OSA |
16 (22.2%) |
10 (34.5%) |
6 (14.0%) |
0.04 |
| HF |
16 (22.2%) |
10 (34.5%) |
6 (14.0%) |
0.04 |
| TIA/CVA |
4 (5.6%) |
0 (0%) |
4 (9.3%) |
0.09 |
| CHADS2VASC |
2.7 ± 1.4 |
3 ± 1.2 |
2.4 ± 1.4 |
0.4 |
| Smoking |
30 (44.1%) |
11 (44.0%) |
19 (44.2%) |
0.99 |
| ETOH |
40 (58.8%) |
12 (48.0%) |
28 (65.1%) |
0.17 |
| PeAF |
28 (38.9%) |
19 (65.5%) |
9 (20.9%) |
0.0001 |
| Preablation sinus rhythm |
34 (47.2%) |
7 (24.1%) |
27 (62.8%) |
0.001 |
BMI: body mass index; HTN: Hypertension; DM-II: diabetes mellitus type II; CAD/PAD: coronary artery disease or peripheral artery disease; OSA: obstructive sleep apnea; HF: heart failure; TIA/CVA: transient ischemic attack or cerebrovascular accident; CHADS2VASC: stroke risk score for atrial fibrillation; ETOH: alcohol abuse history; PeAF: Persistent atrial fibrillation
Left ventricular systolic function: [Table 2]
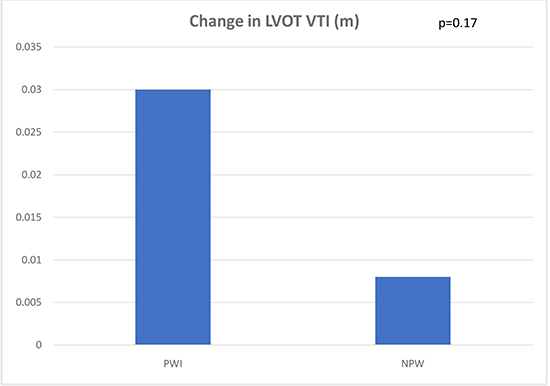
Average left ventricular EF in the pre-ablation PW group was 56 ± 11% vs 57 ± 11% in the NPW group (p=0.71) [Figure 1a]. Average post-ablation EF was 58 ± 10% in the PW group and 58 ± 11% in the NPW group (p=0.89). Average change in LVEF was +1.5 ± 7.8% in the PW group compared to +0.9 ± 9.7% in the NPW group (p=0.78). In the PW group, pre-ablation LVOT VTI was 0.18 ± 0.07 compared to 0.20 ± 0.06 in the NPW group; post-ablation LVOT VTI in the PW group was 0.21 ± 0.05 compared to 0.21 ± 0.05 in the NPW group, and the difference between these two groups was not statistically significant. The average change in LVOT VTI between pre and post ablation echocardiograms was +0.03 ± 0.06 in the PW group and 0.008 ± 0.05 in the NPW group [Figure 1b]
, (p=0.17).
Table 2. Echocardiographic data
| Variable |
Total (n=72) |
PWI (n=29) |
Non-PWI (n=43) |
p-value |
| Preablation LVOT VTI (m) |
0.19 ± 0.06 |
0.18 ± 0.07 |
0.20 ± 0.06 |
0.45 |
| Postablation LVOT VTI (m) |
0.21 ± 0.05 |
0.21 ± 0.05 |
0.21 ± 0.05 |
0.61 |
| Change in LVOT VTI (m) |
0.018 ± 0.05 |
0.03 ± 0.06 |
0.008 ± 0.05 |
0.17 |
| Preablation LVEF (%) |
56.6 ± 10.6 |
56.0 ± 10.6 |
57.0 ± 10.7 |
0.71 |
| Postablation LVEF (%) |
57.7 ± 10.4 |
57.5 ± 9.9 |
57.8 ± 10.8 |
0.89 |
| Change in LVEF (%) |
1.2 ± 8.9 |
1.5 ± 7.8 |
0.86 ± 9.7 |
0.78 |
| Preoperative "A" velocity (MV inflow doppler) (m/s) |
0.65 ± 0.24 |
0.49 ± 0.15 |
0.73 ± 0.24 |
0.01 |
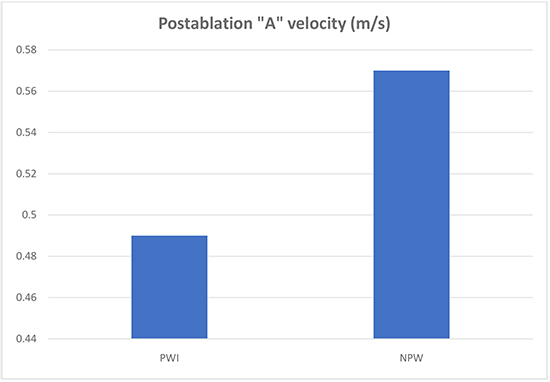
| Postoperative "A" velocity (MV inflow doppler) (m/s) |
0.53 ± 0.19 |
0.49 ± 0.19 |
0.57 ± 0.19 |
0.16 |
| Change in DT |
47.14 ± 93.8 |
40.6 ± 88.5 |
54.5 ± 101.64 |
0.10 |
| Change in LA volume index |
-1.95 ± 10.2 |
-4.93 ± 11.45 |
-0.77 ± 12.53 |
0.35 |
| Change in E/E’ |
2.14 ± 4.37 |
1.03 ± 2.38 |
2.81 ± 6.21 |
0.49 |
LVOT VTI: left ventricular outflow tract velocity time integral; LVEF: left ventricular ejection fraction; MV: mitral valve; LA: left atrium; DT: deceleration time
Figure 1a. Comparison of postablation left ventricular ejection fraction in the PWI (posterior wall isolation group) compared to NPW (non-posterior wall).
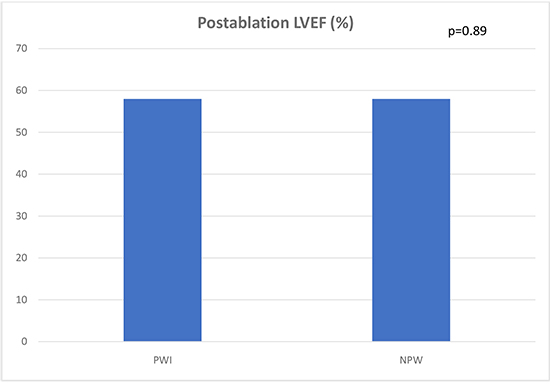
Figure 1b. Comparison of change in left ventricular outflow tract velocity time integral in the posterior wall ablation group versus non posterior wall.
Left ventricular diastolic function:
The change in DT was similar in the PW group and NPW groups (40.6±88.5 vs 54.5±101.64; p=ns). The change in E/E’ ratio was also similar between the two groups: 1.03±2.38 in the PW group and 2.81±6.21 in the NPW group (p=0.49)
Mean preablation and post ablation pulmonary pressures measured using tricuspid flow in echocardiogram were 31 + 8.5 mm Hg and 31 + 9.6 mmHg respectively. The differences between PW and NPW groups were non-significant.
Left atrial function and size:
Left atrial parameters assessed included A velocity on mitral inflow Doppler if patients were in sinus rhythm as well as left atrial volume index. Preoperative A velocity was lower in in the PW group was 0.49±0.15 compared to 0.73±0.24 in the NPW group, (p=0.01). The average postoperative A velocity on mitral inflow Doppler assessment was 0.49 ± 0.19 in the PW group compared to 0.57 ± 0.19 in the NPW group, (p=0.16) [Figure 1c]. “A” velocity was not able to be assessed in patients who were in atrial fibrillation at time of follow up imaging. There was no difference between the PW and NPW groups in the change in left atrial volume index (-4.93±11.45 vs -0.77±12.53; p=0.35) respectively.
Figure 1c. Comparison of postablation Doppler “A” velocity across the mitral valve in the posterior wall isolation group versus non-posterior wall.
Posterior wall ablation has become a commonly used ablation strategy for patients with persistent atrial fibrillation, and a meta-analysis of studies has shown superiority compared to CPVA alone7. The rationale behind posterior wall ablation is that it shares a common embryology with pulmonary vein tissue 14, and develops significant conduction abnormalities 15 and remodeling in patients with worsening atrial fibrillation 1617, all of which result in a substrate for development and maintenance of arrhythmia.
Heart failure and atrial fibrillation are often coexisting disease processes that result in a multiplicative effect on worsening outcomes 18. Worsening left ventricular function has a direct correlation with mortality in patients with atrial fibrillation 19. Likewise, worse left atrial function is an independent predictor of mortality in patients with heart failure 20. It logically follows that it is critical that we know the impact of ablation procedures on those parameters, lest we potentially cause more harm than good.
Echocardiographic parameters for LV and LA function have been reported in prior studies involving posterior wall ablation 521, but to our knowledge there are no studies that directly compare the effect of posterior wall ablation using a variety of modalities on echocardiographic parameters with patients who undergo non-posterior wall ablation procedures. Our data set shows that the more extensive lesion set achieved by posterior wall ablation, either by cryoballoon or hybrid surgical technique, does not adversely affect parameters of LV function LVOT VTI, and ejection fraction when compared to less extensive ablation procedures. In fact, there was a small but statistically significant increase in LVOT VTI in the PW group compared to NPW. While there was a statistically significant increase in “A” velocity after ablation, this was limited by the fact that only 3 patients in the PW and 27 patients in the NPW were in sinus rhythm pre-ablation, compared to 19 and 9 respectively, as “A” can only be measured in sinus rhythm.
We are aware of improved atrial remodeling and left ventricular function in patients with atrial fibrillation who undergo catheter ablation 1222. One study involving patients with persistent atrial fibrillation who underwent hybrid surgical posterior wall ablation showed that patients who responded to ablation had a greater atrial and left ventricular remodeling effect than those who did not 23. Though the PW constitutes more than 50% of the entire surface of left atrium, from our study results, it could be inferred that PW does not have a significant mechanical role in left atrial hemodynamics, and electromechanical ablation of it has a negligible impact on our measured parameters. Another possibility is that any downside from the more extensive ablation lesion set is offset by the higher success rate in maintaining sinus rhythm and potentially contributing to a higher chance of positive remodeling, and notably more than 80% of our cohort remained in NSR during follow up echocardiogram.
There are several limitations for our study inherent to retrospective analysis. The time between pre and post ablation echocardiograms vary significantly for this patient group, which may allow for development of significant confounding variables (MI, worsening valvulopathy, etc) when assessing pre and post ablation echocardiographic data. There is known inter-reader variability when assessing echocardiograms, particularly in the assessment of LVEF, although we also took into account quantitative measurements such as LVOT VTI and A wave velocity. Due to differences in echocardiography protocols, “A” wave and LVOT VTI was not adequately measured in all of our patients. In addition, a large proportion of patients pre-ablation were in atrial fibrillation, precluding measurement of “A” velocity, making it difficult to assess a change in “A” velocity velocity. Baseline characteristics varied significantly between the two groups – as posterior wall ablation was performed for patients with longer duration of persistent AF, may result in bias in the data. This was alleviated somewhat by using each patient was his own control in comparing changes in pre and postablation LVEF and VTI. Finally, as this study represents a single center experience with retrospective data, results may not be generalizable.
Posterior wall isolation is a safe and effective method for catheter ablation of atrial fibrillation. Compared to patients who underwent non-posterior wall isolation procedures, there was no negative effect in left ventricular function. While measurement of left atrial function was limited by the small number of patients in sinus rhythm prior to ablation, there likewise appeared to be no negative effect in left atrial size or function from posterior wall isolation.






