Impact of Atrial Fibrillation in Patients with Acute Myocardial Infarction and Cardiogenic Shock Receiving Coronary Revascularization with Percutaneous Ventricular Assist Device Support
Teruhiko Imamura1
1Second Department of Medicine, University of Toyama, Japan.
Key Words : Heart failure, Anticoagulation, Hemodynamics.
Correspondence to: Teruhiko Imamura MD Ph.D. FAHA FACC FESC FHFSA FJCC
Second Department of Medicine, University of Toyama,
2630 Sugitani Toyama Toyama 930-0194 Japan
Atrial fibrillation is common in patients with advanced heart failure and associated with high mortality,1 whereas its impact on those receiving mechanical circulatory supports remains controversial.2Gupta and colleagues demonstrated that atrial fibrillation was not associated with in-hospital mortality in patients with acute myocardial infarction and cardiogenic shock requiring coronary revascularization and percutaneous ventricular assist devices.3 Several concerns should improve their findings.
Despite a propensity score matching, there still remained statistically un-matched variables, including age and sex, which would also have considerable impacts on mortality and morbidity.
Approximately 20–30% of patients had coagulopathy at baseline, whereas most patients with atrial fibrillation would have received anticoagulation therapy to prevent stroke. The definition of coagulopathy might be unclear.
Appropriate anti-coagulation therapy during coronary revascularization with percutaneous ventricular assist devices remains great concern particularly when patients have atrial fibrillation. Additional analysis investigating the association between the magnitude of anti-coagulation therapy and comorbidities among those with atrial fibrillation would clarify the optimal anti-coagulation therapy in such a clinical situation.
We appreciate the comments made by Dr. Imamura on our paper recently published in the JAFIB discussing the impact of atrial fibrillation on hospitalization outcomes of acute myocardial infarction associated cardiogenic shock while undergoing percutaneous coronary intervention with ventricular assist device1. Please find below our responses to the queries raised by Dr. Imamura.
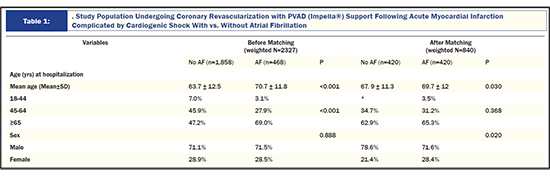
1) We used 1:1 propensity-score matched analysis and we concur with the observation that there remained the statistical difference between the two groups for the mean age of admission and sex distribution of cohorts. Despite this finding,we feel that the numbers did not differ significantly from each other to yield major outcomes difference in the clinical arena. For example, mean age was 67.9 vs. 69.7 years whereas both groups predominantly consisted of males (>70%). We agree thatstricter selection control could be possible in future prospective studies.
2) As we mentioned in the methodology section of the paper, we utilized an administrative retrospective database for our analysis creating inherent limitations. As Dr. Imamura correctly pointed out, nearly 20% of hospitalizations had demonstrated coagulopathy at baseline, which was identified using ICD-9 CM diagnostic code from any of the secondary discharge diagnoses. The ICD-9 CM codes used in the analysis were 286.0-286.9, 287.1, 287.3-287.5,289.84, 649.30-649.34.
Figure 1.
3) We completely agree that it is important to investigate the association between the magnitude of anticoagulation therapy and comorbidities among those with atrial fibrillation to aid in clarifying the optimal anticoagulation therapy in this high-risk clinical scenario. However, as mentioned in the manuscript, the National Inpatient Sample database does not contain detailed information on the magnitude and duration of anticoagulation therapy in these patients.
We thank Dr. Imamura for their comments regarding our analysis and we believe these valuable comments underscore the importance of this first large-scale analysis of this understudied but important research topic.
TI receives grant support from JSPS KALENHI: JP20K17143.






