Routine Transesophageal Echocardiography in Atrial Fibrillation Before Electrical Cardioversion to Detect Left Atrial Thrombosis and Echocontrast
Sebastian Feickert∞a, Giuseppe D´Anconaa*, Hüseyin Incea, Kristof Grafb, Elias Kugelb, Monica Mureroac, Erdal Safaka
aDepartment of Cardiology, Vivantes Klinikum im Friedrichshain und Am Urban, Berlin, Germany and Rostock University Medical Center, Rostock, Germany.bDepartment of Internal Medicine and Cardiology, Jüdisches Krankenhaus Berlin, Berlin, Germany.cDepartment of Communication and New Technology Studies, Federico II University, Naples, Italy.*These authors contributed equally.
Transesophageal echocardiography (TEE) before electrical cardioversion (ECV) in atrial fibrillation (AF) is not routinely performed in anticoagulated patients.
Starting from TEE findings of anticoagulated and non-anticoagulated patients referred for ECV, we investigated the rate of spontaneous echo-contrast (SEC) and left atrial thrombus (LAT) and identified their independent predictors.
A total of 403 patients were included: 262 (65%) had no anticoagulation, 47 (11.7%) were onnovel oral anticoagulant (rivaroxaban), 74 (18.4%) on warfarin INR>2, and 20 (5.0%) on warfarin INR<2.In 41 (10.1%) there was LAT and in 154 (38.2%) SEC. Patients with LAT had a significantly lower left ventricular ejection fraction (LVEF%) (p=0.001). Patients with SEC were significantly older (p=0.04), had lower LVEF% (p<0.0001),higher CHADSVASC score (p<0.0001), and higher rate of coronary artery disease (CAD) (p=0.03). In 56.8% of warfarin patients (INR>2) there was SEC (p=0.002). At multivariate analysis therapeutic anticoagulation with warfarin (p=0.003; OR:2.2; CI: 1.3-3.7),CHADSVASC score (p<0.0001; OR=1.2; CI: 1.1-1.4), and LVEF% (p<0.0001; OR:0.95; CI: 0.93-0.97; inverse relationship) were SEC predictors. A 3.5 CHADSVASC score cut-off was predictor of SEC (AUC: 0.7; p<0.0001). LVEF% was the only predictor of LAT (p=0.02; OR=0.96; CI: 0.93-0.99; inverse relationship).
Echocardiography before ECV identifies clear LAT/SEC in more than a third of AF patients, independently by their anticoagulation regimen. LAT/SEC rates increasewith decrement of LVEF%. Increment of CHADSVASC score increases SEC risk. In anticoagulated patients SEC rate remains higher than expected. Therapeutic anticoagulation with Warfarin appears positively and independently correlated to SEC occurrence.
Key Words : Transesophageal, Echocardiography, Thrombus, Atrial, Fibrillation, Echocontrast.
Sebastian Feickert, MD
Department of Cardiology, Vivantes Klinikum Am Urban, Dieffenbachstraße 1, 10967 Berlin-Kreuzberg
Atrial fibrillation (AF) is the most common sustainedtachyarrhythmia in the general population and is associated with a high risk of thromboembolism leading to ischemic events 1-3.
Transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE)are necessary tools to diagnose the presence of left atrialthrombosis (LAT)andLA spontaneous echo contrast (SEC). Both conditions are possibly related to the occurrence of cardiac thromboembolism 3.
Starting from TEE findings of anticoagulated and non-anticoagulated patients referred for electrical cardioversion (ECV) of stable persistent (> 48hrs) non-valvular AF, we investigated the rate of SEC and LAT and identified their independent predictors.
Patients were referred to our tertiary care facility from 1/2012 to 6/2015. Demographic, clinical, and echocardiographic data were collected and stored in the electronic medical recording system. Additional data 4 were collected in a separate database for the purpose of performing a doctoral thesis on the specific topic.
The patients included in the present analysis are not consecutive. In fact,onlypatientsthathad been in AF for at least 48 hours before being referred for ECV are included. Furthermore, none of the included patients had been treated for AF within the premises of our facility before. Elective ECV had been planned after having documented a pharmacologically unresponsiveness, defined as failure or intolerance after admission of at least one class I or III anti-arrhythmic drug and/or after patient/referring physician choice. None of the investigated patients presented significant cardiac valve malfunction/disease and none had been previously submitted to cardiac surgical operations.
All patients or their legal representatives signed informed consent to treatment, data collection, and data analysis for scientific research purposes. An ethical commission revision was waved being the study a retrospective analysis of prospectively collected patients´ data and having the study no effect upon the standard of patients´ management.
ECHOCARDIOGRAPHIC EXAMINATION
In preparation to the ECV, all patients underwent TTE and TEE, according to the local standards.Exams were performed by experienced echocardiographers. At TTE, bidimensional(2D) volumetric measurements were used to derive left ventricular ejection fraction (LVEF%) and LAdimension. At TEE, LA and LA appendage (LAA) were viewed in the mid-esophageal window using simultaneous biplane imaging.
Thrombus in the LAA was defined as an echogenic mass with a different texture than the LA wall and a uniform consistency. SEC was documented in case of a swirling pattern of increased echogenicity in the LAA and/or LA. Grading of SEC was not reported 5. Evidence of cardiac valve pathology was investigated and excluded.
Data are presented as absolute numbers, percentages, mean ± standard deviation for normally distributed variables and median with 75% IQR values for variables with non-normal distribution. We assessed for normal distribution using the Shapiro-Wilk test. Patients had been referred from different referring physicians and anticoagulation management was not homogenous. We first compared patients´ demographic and clinical data according to the anticoagulation regimen. A second grouping was performed according to the presence of LAT and SEC at pre-ECV TEE. We identified 4 groups (with/without LAT and with/without SEC). Analysis of the variance (ANOVA), Student t-test, Wilcoxon signed-rank test, χ-square, and Fischer-exact test were used whenever appropriate to compare groups (according to anticoagulation regimen, with LAT vs. w/o LAT; with SEC vs. w/oSEC). A p-value <0.05 was considered as significant. Two multivariable models were built and stepwise backward logistic regression was performed to identify independent echocardiographic and clinical determinants for LAT and SEC. We included in the logistic regression model only those variables that at univariate analysis had a statistical difference with a p<0.1. Receiver operating characteristic (ROC) curves were built to identify cut-off values that could predict LAT and SEC. Statistical analyses were performedusing SPSS statistical software version19 (SPSS Inc., Chicago, Ill., USA).
A total of 403 patients are included in the present analysis.
Demographic and clinical data of the overall cohort are reported in [Table 1]. A longer than 3 weeks oral anticoagulation with either novel oral anticoagulants (NOAC) or Warfarin at therapeutic levels (INR>2) had been already performed in 30.0%.
A total of 262 patients (65%) had received no previous anticoagulation, 47 (11.7%) were treated with NOAC (rivaroxaban), 74 (18.4%) were anticoagulated with warfarin and had an INR>2 for >3 weeks at time of ECV (verified by either weekly laboratory testing or daily testing with a home-measurement-device), and 20 (5.0%) had received warfarin but at time of ECV had an INR<2 [Figure 1].
Figure 1. Flow diagram of patient’s baseline data and events, apportioned by anticoagulation management
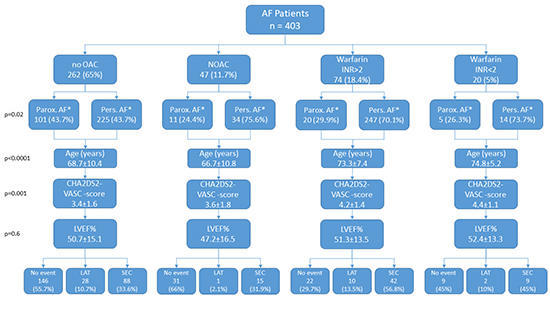
AF: Atrial Fibrillation; OAC: oral anticoagulants; NOAC: novel oral anticoagulants; LVEF: Left Ventricular Ejection Fraction; LAT: Left Atrial Thrombosis; SEC: Spontaneous Echo-contrast; *Information available on 362 patients
[Table 1] reports clinical data according to the anticoagulation regimen. It appears that AF duration (paroxysmal and persistent) is unevenly distributed among the different categories of anticoagulated/non-anticoagulated patients. It emerges in fact, that a significantly higher rate of persistent AF (and significantly lower rate of paroxysmal AF) was present in anticoagulated patients (p=0.02). Furthermore, the subgroup of anticoagulated patients included a significantly higher rate of patients suffering from coronary artery disease (p=0.03). Moreover, patients receiving warfarin were significantly older (p<0.0001) and had a significantly higher CHA2DS2-VASc-score (p=0.001).
Table 1. Clinical and echocardiographic data in the overall cohort and according to anticogualtion regimen
|
Total(403) |
No Anticaogulation(262; 65%) |
NOAC(47; 11.7%) |
Warfarin INR>2(74; 18.4%) |
Warfarin INR<2(20; 5.0%) |
p-value |
| Age (years) |
69.6±10.3 |
68.7±10.4 |
66.7±10.8 |
73.3±7.4 |
74.8±5.2 |
<0.0001 |
| Gender: F/M |
188/215 |
115/147 |
20/27 |
44/30 |
9/11 |
0.1 |
| LVEF% |
50.7±14.8 |
50.7±15.1 |
47.2±16.5 |
51.3±13.5 |
52.4±13.3 |
0.6 |
| LA Diameter |
4.3±0.7 |
4.2±0.6 |
4.5±0.8 |
4.4±0.7 |
4.6±0.5 |
0.1 |
| CHA2DS2-VASC -score |
3.6±1.6 |
3.4±1.6 |
3.6±1.8 |
4.2±1.4 |
4.4±1.1 |
0.001 |
| Diabetes Mellitus |
133(33%) |
83(31.7%) |
15(31.9%) |
26(35.1%) |
9(45%) |
0.6 |
| CAD |
185(45.9%) |
108(41.2%) |
25(53.2%) |
38(51.4%) |
14(70%) |
0.03 |
| Creatinine (mg/dl) |
1.1±0.5 |
1.1±0.5 |
1.1±0.5 |
1.1±0.4 |
1.3±0.5 |
0.6 |
| Paroxismal AF* |
137(37.8%) |
101(43.7%) |
11(24.4%) |
20(29.9%) |
5(26.3%) |
0.02 |
| Persistent AF* |
225(62.2%) |
130(56.3%) |
34(75.6%) |
47(70.1%) |
14(73.7%) |
14(73.7%) |
| Previous Thromboembolism |
17 (4.2%) |
10(3.8%) |
2(4.3%) |
5(6.8%) |
0 |
0.5 |
| LAT |
41 (10.2%) |
28(10.7%) |
1(2.1%) |
10(13.5%) |
2(10%) |
0.2 |
| SEC |
154 (38.2%) |
88(33.6%) |
15(31.9%) |
42(56.8%) |
9(45%) |
0.002 |
LA: Left Atrium; CAD: Coronary Artery Disease; LAT: Left Atrial Thrombosis; SEC: Spontaneous Echo-contrast
Clear evidence of LAT was present,at pre-ECV TEE, in 41 patients (10.2%) and SEC in 154 (38.2%).
A total of 27 patients (6.6%) had both LAT and SEC. Patients with evidence of LAT and/or SEC did not undergo ECV and were referred back to the treating cardiologist to optimize anticoagulation. Repeatedfollow-up imaging, starting after four weeks of optimized anticoagulation treatment, was recommended in all cases. All remaining patients (235/403; 58.3%) underwent at least one ECV attempt (data concerning sinus rhythm achievement are not reported). No acute thromboembolic events immediately after ECV were reported.
Patients under Warfarin and with INR> 2 had a trend for higher LAT rate (13.5%) and a significantly higher SEC rate (56.8%; p=0.002) [Table 1].
[Table 2]-[Table 3] show clinical data according to the presence of LAT/SEC.
Table 2. Clinical and echocardiographic data according to the presence of left atrial thrombosis at TEE
|
No-LAT(362) |
LAT(41) |
p-value |
| Age (years) |
69.5±10.6 |
70.3±8.1 |
0.5 |
| Gender: F/M |
195/167 |
20/21 |
0.5 |
| LVEF% |
51.6±14.3 |
42.4±16.6 |
0.001 |
| LA Diameter (cm) |
4.3±0.7 |
4.4±0.5 |
0.3 |
| CHA2DS2-VASC -score |
3.6±1.6 |
3.9±1.5 |
0.2 |
| Paroxismal AF* |
125(38.1%) |
12(35.3%) |
0.7 |
| Persistent AF* |
203(61.9%) |
22(64.7%) |
0.7 |
| Previous Thromboembolism |
14 (3.9%) |
3(7.3%) |
0.3 |
| Diabetes Mellitus |
116(32%) |
17(41.5%) |
0.2 |
| CAD |
167(46.1%) |
18(43.9%) |
0.7 |
| Creatinine (mg/dl) |
1.1±0.5 |
1.3±0.6 |
0.1 |
LA: Left Atrium; CAD: Coronary Artery Disease; LAT: Left Atrial Thrombosis; SEC: Spontaneous Echo-contrast
Table 3. Clinical and echocardiographic data according to the presence of spontaneous echo-contrast at TEE
|
No-SEC(249) |
SEC(154) |
p-value |
| Age (years) |
68.9±11.4 |
70.9±8.3 |
0.04 |
| Gender: F/M |
136/113 |
79/75 |
0.5 |
| LVEF% |
53.3±13.4 |
46.6±15.8 |
<0.0001 |
| LA Diameter (cm) |
4.2±0.7 |
4.4±0.6 |
0.1 |
| CHA2DS2-VASC -score |
3.4±1.6 |
4.1±1.5 |
<0.0001 |
| Paroxismal AF* |
89(40.3%) |
48(34.0%) |
0.2 |
| Previous Thromboembolism |
9 (3.6%) |
8(5.2%) |
8(5.2%) |
| Persistent AF* |
132(59.7%) |
93(66.0%) |
0.2 |
| Diabetes Mellitus |
78(31.3%) |
55(35.7%) |
0.3 |
| CAD |
104(41.8%) |
81(52.6%) |
81(52.6%) |
| Creatinine (mg/dl) |
1.1±0.4 |
1.2±0.6 |
0.1 |
LA: Left Atrium; CAD: Coronary Artery Disease; LAT: Left Atrial Thrombosis; SEC: Spontaneous Echo-contrast
At univariate analysis patients with LAT had a significantly lower left ventricular ejection fraction (LVEF%) (p=0.001). Patients with SEC were significantly older (p=0.04), had a significantly lower LVEF% (p<0.0001), higher CHADSVASC score (p<0.0001), and higher rate of CAD (p=0.03).
Two separate logistic regression models were built to identify determinants of LAT and SEC. LVEF% was the only echocardiographic independent predictor of LAT (p=0.02; OR=0.96; CI: 0.93-0.99; inverse relationship) and SEC (p<0.0001; OR:0.95; CI: 0.93-0.97; inverse relationship) [Table 4]. At ROC analysis a LVEF of 45% or lower showed a significant prediction of LAT and SEC (AUC: 0.7; p<0.0001; Sensitivity 75.0%- Specificity 60.0%). Moreover, therapeuticanticoagulation with warfarin (INR>2) (p=0.003; OR: 2.2; CI: 1.3-3.7) and CHADSVASC score (p<0.0001; OR=1.2; CI: 1.1-1.4) were both independent predictors of SEC. At ROC analysis aCHADSVASC score value of 3.5 was the cut-off to predict SEC (AUC: 0.7; p<0.0001; Sensitivity 64.0%- Specificity 60.0%).
Table 4. Logistic regression analysis to identify determinants of LAT and SEC
|
OR |
CI |
p-value |
| LAT Determinants |
| LVEF% |
0.96 |
0.93-0.99 |
0.02 |
| SEC Determinants |
| LVEF% |
0.95 |
0.93-0.97 |
<0.0001 |
| Warfarin Anticoagulation (INR>2) |
2.2 |
1.3-3.7 |
0.003 |
| CHA2DS2-VASC -score |
1.2 |
1.1-1.4 |
<0.0001 |
| Age |
0.97 |
0.94-1.0 |
0.08 |
| CAD |
1.1 |
0.6-1.8 |
0.6 |
| Persistent AF |
0.7 |
0.4-1.1 |
0.2 |
LVEF: Left Ventricular Ejection Fraction; CAD: Coronary Artery Disease; LAT: Left Atrial Thrombosis; SEC: Spontaneous Echo-contrast
Findings of our analysis can be summarized as follows:a) routine TEE prior to ECV shows clear signs of LAT/SEC in more than a third of referred AF patients independently by their anticoagulation regimen; b) the rate of LAT/SEC increases significantly with the decrement of LVEF% but does not seem to be independently related, at least in our analysis, to LA size; c) cumulative risk stratification methods, such as the CHADSVASC score, seem to have an independent predictive power particularly upon the risk of SEC; d) the risk of SEC increases for CHADSVASC scores above a 3.5 value; e) finally, even in anticoagulated patients the LAT and SEC rates remain higher than expected. In particular, therapeutic anticoagulation (INR>2) with Warfarin appears to be independently correlated with SEC occurrence.
A notable number of 262 patients (65%) had received no previous anticoagulation to hospital admission. Traceable reasons for no previous anticoagulation included a CHADSVASC score <3 for females and < 2 for males, non-compliance to anticoagulation, or absolute contraindication to anticoagulation resulting mainly from increased bleeding risk. Furthermore, a not negligible number presented to their outpatient doctor on the day of admission with a sudden unset of a previously untreated atrial fibrillation episode, which, due to the pronounced symptoms, immediately led to the patient being referred to our hospital for acute medication and subsequent TEE and ECV.Our tertiary care hospital mainly treats patients referred by their family doctor, or their outpatient cardiologist with a specific indication to ECV. While we are convinced that all the necessary efforts to anticoagulate the patient have been made properly, within a society dense with fragile and elderly patients it is quite common to encounter situations where permanent oral anticoagulation is contraindicated. We recommend continuation of oral anticoagulation for at least 4 weeks after successful ECV in all patients and discuss alternative options to permanent anticoagulation (e.g. left atrial appendage closure) with the further attending physician of all patients with a high stroke and high bleeding risk.
LAT prevalence and prediction
Although guidelines recommend ECV without TEE after a 3-week course of anticoagulation 2, routine TTE and TEE before ECV of AF are the present standard of practice in our clinic, and in many other German facilities, independently by the adopted anticoagulation regimen and by its duration and therapeutic level. In fact, systemic embolism during ECV may occur in spite of adequate anticoagulation and it ranges around 0.5%-1% for both patients anticoagulated with vitamin K antagonists (VKA) and NOACs 6-8. This risk is not negligible and may be secondary to the fact that LAT rate may be higher than expected and LAT may persist even in anticoagulated patients. More specifically, few studies have investigated the echocardiographic evidence of LAT in patients with non-valvular AF prior to ECV. In this selected group of patients LAT prevalence is ranging from 4% to 8% even after having received either NOACs or therapeutic warfarinization 9-11.
Previous studies have shown that the CHADS2 and CHA2DS2-VASc scores predict the presence of LAT in patients undergoing TEE before AF catheter ablation 11-13.In a logistic regression model including 372 anticoagulated patients Bejinariu et al. have shown that CHA2DS2-VASc (OR =1.2) and LVEF% (OR=0.96) were the only independent determinants for LAT 14. This means that patients with a very high risk score for thromboembolism could be refractory to standard anticoagulation and develop LAT.
More recently Kosmalska et al. have specifically investigated the usefulness of TEE before ECV of atrial arrhythmias in a prospective series of 269 patients 15. LAT and/or SEC were detected in a higher rate of patients (29%). Interestingly, in 94.9% of patients with LAT or SEC, an appropriate anticoagulation regimen had been adopted 15. Dementia, low velocities in LAA, SECin LA, consecutive episodes of AF, and longer duration of AF were all significant predictors of LAT and/or dense SEC. CHA₂DS₂VASc score was not an independent predictor of LAT and SEC 15.
In our real-worldexperience,we have reported an overall LAT rate of 10.2% (and 38.2% for SEC). Interestingly, in our experience patients under NOAC had a trend for a lower incidence of LAT (2.1%) and patients on warfarin with therapeutic INRs values had the highest LAT rate (13.5%), even higher than that observed in non-anticoagulated patients (10.7%). This could be due to the fact that patients on warfarin had a more complex comorbid profile, including older age and significantly higher CHA2DS2-VASC scores. In this context, identification of clinical predictors of LAT may be of help to support anticoagulation therapy and to guide TEE screening before ECV.
We were not able to identify an independent relationship between LAT and CHADVASC scorealthough we did find LVEF% to be the only echocardiographic independent predictor for LAT.
SEC prevalence and prediction
SEC is resulting from an interactionbetween multiple hematologic (erythrocyte sedimentation rate, serum fibrinogen level, hematocrit level, plasma proteins concentration) and hemoreological factors (blood flow velocity, blood viscosity, and shear rate) 16. In comparison to LAT, the prevalence of SEC can be over 50% in patients with non-valvular AF 17. As documented in our and in previous experiences 14, the majority of patients with SEC do not have LAT and vice-versa. This could support the fact that the two conditions have different etiopathogenesis.
Independent clinical and echocardiographic determinants for SEC have been poorly investigated. Bejinariu et al. have proposed the independent relationship among LA dimensions, LVEF%, CHADSVASC -score, and SEC occurrence 14. Our findings confirm that a LVEF% < 48% and a CHADSVASC score > 3.5 are good independent predictors of SEC occurrence.
The clinical impact of SEC remains controversial. A series of studies focusing on patients treated with different therapeutic and sub-therapeutic anticoagulation regimenshave confirmed the low thromboembolic risk of SEC, even in non-anticoagulated patients 3,16,18.
The current guidelines do not indicate if patients with SEC can be safely cardioverted in the absence of LAT 2. In this context, many practitioners consider early ECV ofpatients with SEC to be unsafe.Although anticoagulation therapy with warfarin is widely used to prevent thromboembolism in AF, it actually does not affect red cell aggregation in vitro and, consequently, it has no effect on LA SEC prevention /resolution 19. Ito et al. were the first to investigate the effect of warfarin therapy on LA SEC in patients with non-valvular AF. They confirmed that effective anticoagulation did not reduce the quantitative value of LA SEC 20. In our reported experience, therapeutic anticoagulation with warfarin appeared actually positively and independently correlated to SEC occurrence, even after adjusting for echocardiographic parameters (LVEF%), demographic data (age), and cumulative risk scores (CHA2DS2-VASC).
In this context, delayed ECV to perform appropriate anticoagulation in patients with AF and associated SEC may present consistent additional risks and fewer benefits.Stoddard et al. have demonstrated a higher prevalence of SEC and of new-onset LAT in patients who do not undergo early ECV 21. Moreover, a longer permanence in AFwill reduce the immediate success rate of ECV and the maintenance of sinus rhythm after successful ECV 22. Finally, the ACUTE trial has confirmed that TEE-guided early ECV with abbreviated anticoagulation allows for hemorrhagic events reduction, shorter time to cardioversion, and greater rate of sinus rhythm restoration 23.
The study includes a heterogeneous group of patients referred from different facilities after being managed with different anticoagulation strategies. In this context, although the overall sample size is significant (in consideration of the fact that all patients had non-valvular AF and underwent pre-ECV TTE and TEE), pre-ECV treatment was not uniform and most of the patients had actually received no anticoagulation before being sent to our facility. Moreover, we do not have a structured follow-up on the referred patients and, as a matter of fact, we are not aware of the evolution of LAT and SEC in those patients that were denied ECV. Furthermore, the duration of AF did not emerge as a potential independent derteminant for SEC and LAT in our logistic regression model. The stronger impact of other variables such as LVEF, warfarinization, and CHADVASC score upon SEC/LAT may veil the real effect of AF duration. Some of those determinants, like LVEF, may actually be a surrogate of AF duration, suggesting there may exist a collinearity among the independent determinants. Unfortunately, there is no way to eliminate this collinearity from the present data.
Additionally, a stratification of patient groups into those with and those without anticoagulation for primary analyses could be usefull to gain additional information about independent risk factors but has not been performed to avoid a considerable decrease in power by reducing the sample size.
The occurrence of LAT and SEC is consistent, independently from the anticoagulation regimen adopted. Clinical and echocardiographic parameters can be used to predict the occurrence of LAT and SEC in patients with non-valvular AF. This information could be used in the future to select patients that, in spite of appropriate anticoagulation, should be evaluated with TEE before undergoing ECV.
Finally, although most of our present clinical decisions are based on our interpretation of TEE findings, in the very next future new methods of imaging analysis, based on artificial intelligence systems, will be made available for the daily clinical practice. Improved and automated image interpretation will allow us to better understand the LA and LAA anatomy and possibly detect specific anatomical features and early signs correlated to LAT and SEC occurrence [24].






