Unexpected Detection of Floating Thrombi in Left Atrium After Left Atrial Appendage Ligation with Atriclip Device: A Case Report
Sana N. Buttar1, Peter B. Hansen2, Christian Hassager3, Henrik Ø. Andersen1
1Department of Cardiothoracic Surgery, University Hospital of Copenhagen, Rigshospital, Denmark.2Department of Thoracic-Anaesthesiology, University Hospital of Copenhagen, Rigshospital, Denmark.3Department of Cardiology, University Hospital of Copenhagen, Rigshospital, Denmark.
AtriClip device has demonstrated an excellent efficacy, long-term durability and safety of left atrium appendage (LAA) closure. We report, the unexpected postoperative transesophageal echocardiography (TEE) finding of thrombi in left atrium (LA) after deployment of an AtriClip in a 73-year-old man with chronic atrial fibrillation and 3-vessel-coronary artery disease undergoing coronary artery bypass grafting (CABG) surgery and LA appendage ligation. The heart was re-arrested and thrombi were retrieve successfully through a left atriotomy. This case emphasizes the unanticipated role of AtriClip in dislodging the thrombus from LAA, in addition to the importance of sufficient and well-founded imaging (Transesophageal Echocardiogram/ Multidetector Computed Tomography) before and after the deployment of AtriClip device.
Key Words : , , ,.
Sana Naseer Buttar
Vesterbrogade 89A, 3th
1620, Copenhagen, Denmark
The left atrial appendage (LAA) is the primary source of thromboembolic events in patients with non-valvular (90%) and valvular (60%) atrial fibrillation (AF) 1. As the standard-of-care with oral anticoagulants (OAC) has limited applicability to selected patients, novel interventional and surgical approaches have emerged for LAA occlusion 2. While LAA occlusion with percutaneous approaches fail to provide 100% solution due to inherent limitations 3, the use of AtriClip has shown near 100% occlusion rates in comparison to previous surgical techniques 4, in addition to excellent efficacy and safety 3,4. To date, no randomized studies or societal guidelines have been published regarding AtriClip use in patients with AF undergoing cardiac surgery.
Herein, we present a case of thrombi in left atrium (LA) after deployment of AtriClip device on LAA in a patient undergoing coronary artery bypass grafting (CABG) surgery.
A 73-year-old man with a history of hypertension, vascular claudication, chronic atrial fibrillation (AF) and 3-vessel-coronary artery disease, presented for coronary artery bypass graft (CABG) surgery and left atrium appendage (LAA) ligation using the AtriClip device. He was anticoagulated with Pradaxa (New Oral Anticoagulant (NOAC), 150mg twice daily) for nine years, which was discontinued four days before the surgery as per institutional guidelines. Unfortunately, on the scheduled day of CABG surgery, the procedure was postponed due to emergency operations. The patient was discharged to home on the same day without re-commencement of Pradaxa as the surgery was re-scheduled only four days later.
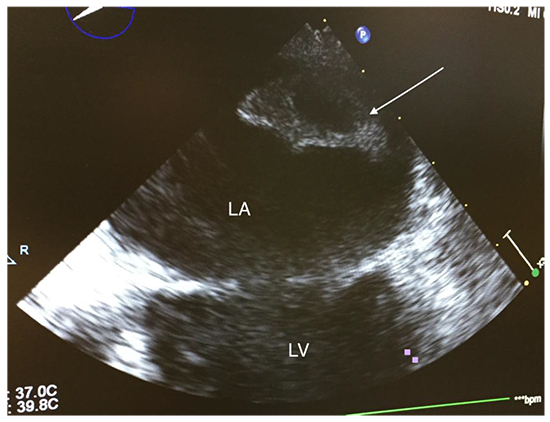
The procedure was performed via median sternotomy. Baseline cardiac rhythm was AF. A complete 2-dimensional (2D) intraoperative transesophageal echocardiogram (TEE) before cardiopulmonary bypass (CPB) demonstrated severely depressed left ventricle function (Ejection Fraction (EF) 30%) and dilation of both atriums and appendages. Mitral – and aortic valves were found to be normal, while the tricuspid valve was noted to have a mild insufficiency. The interrogation of LA and LAA showed no evidence of thrombus. The CPB was commenced after achieving an activated clotting time (ACT) > 480 seconds, which was maintained throughout the surgery. Before the cardioplegic arrest, the surgical manipulation of LAA was performed to size the appendage. Subsequently, an AtriClip device was deployed uneventfully across the base of the LA appendage, isolating it from the LA. The heart was then arrested to perform the CABG surgery. A post-procedural TEE unexpectedly revealed echo-dense object in the LA, suspected to be a thrombus [Figure 1].
Figure 1. Two-dimensional transesophageal echocardiogram (TEE) after deployment of AtriClip, showing the largest thrombus in the left atrium (LA) indicated by the arrow. LV; Left Ventricle.
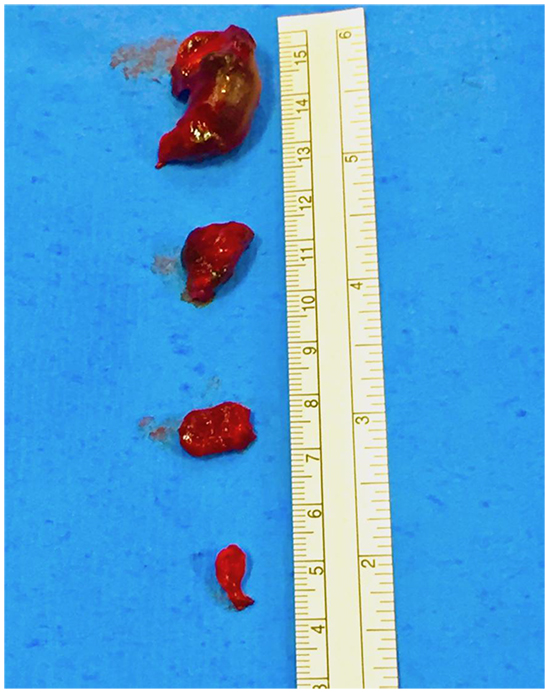
A decision was made to re-arrest the heart and retrieve the suspected thrombus in the LA via the right atrium (RA) and through fossa ovalis. Four objects with the consistency of thrombus were removed from the LA with the largest one located free floating close to the right pulmonary veins, while the other three were trapped in the clamp of the AtriClip and could easily be detached from the device [Figure 2].
Figure 2. Evacuated thrombi with the largest thrombus found free floating in the left atrium (LA) close to the right pulmonary veins, while three smaller thrombi were seen trapped in the AtriClip.
All chambers in the heart were inspected meticulously with no further findings of thrombus. The incisions of fossa ovalis and RA were closed and the patient was weaned off from the CPB followed by de-heparinization. The follow-up TEE revealed no more thrombus in the LA. The patient had an uneventful postoperative course except anticipated AF for which digoxin and warfarin was commenced. Patient was discharged home after five days of surgery.
Most updated guidelines from European Society of Cardiology (ESC - 2016) 5 and AHA/ACC/HRS (2019) 6 on AF management recommend surgical LAA occlusion/excision in patients undergoing open-heart surgery (Class IIb; Evidence Level B). Surgical methods of LAA exclusion such as running sutures, purse-string or external ligation, have failed to provide reproducible and durable LAA occlusion 7. However, a few non-randomized studies have shown that the AtriClip has excellent efficacy for stroke prevention and long-term durability of LAA closure 3,4. In addition, the device has been deemed as a safe procedure with some reporting no device-related complications post-procedural or in follow-up period 3, while others revealed minimal anticipated adverse events such as pericardial effusions with or without pericarditis, tachyarrhythmias and respiratory dysfunction mostly related to atelectasis after thoracoscopic application 4.
In our case, the AtriClip device may have broken an undetected thrombus free from the LAA after the manipulation of the LAA for sizing and subsequent deployment of the device, leading the thrombus to be broken down into multiple small fragments pushed into the LA. Thus, AtriClip application could have resulted in a serious and unanticipated complication, which, however, was avoided by timely discovery and rescue of the thrombi. Another possible way of thrombus dislodgement could be during positioning of the heart for CABG. However, in our case CABG was performed after the AtriClip placement suggesting that the force needed to break the thrombus free from the LAA, was already applied by the AtriClip. In addition, some of the thrombi were extracted from the clamped AtriClip during the thrombi evacuation from the LA. Thus, in our case AtriClip was most likely the source of dislodging the undetected thrombus, which also is in line with a previous study 8.
Two-dimensional (2D) TEE has been proved to be an accurate tool in identifying LA/LAA thrombus, thus consensually; it is used as a gold standard procedure for detection of thrombus 9. However, three-dimensional (3D) TEE has shown to further improve differentiation of thrombi from pectinate muscle and other surrounding structures 9. In our case, an experienced echocardiographer was not able to detect a thrombus in LA or LAA despite using multiplanar 2D TEE. Given the exceptional higher risk of thrombus development in our patient due to chronic AF and preoperative discontinuation of anticoagulation, 3D TEE may have assisted further in identifying the thrombus. Nevertheless, considering the challenging LAA morphology and in result complex anatomic features of thrombi, it can be difficult to detect them by TEE modalities 9. Multidetector computed tomography (MDCT) provides more accurate assessment of LAA anatomy and thereby findings of thrombi 9. In our high-risk patient, MDCT may also have been an ideal pre-procedural approach in visualizing the thrombus.
In conclusion, AtriClip may aggravate thromboembolic event if LAA thrombus is undetected. Patients with high risk of thrombus formation should undergo an extensive pre-operative TEE examination, in some complicated cases perhaps MDCT, to confidently exclude a thrombus in LAA before AtriClip application. A post-AtriClip deployment TEE during the operation is a must in all patients.






