Ablation in Atrial Fibrillation with Ventricular Pacing Results in Similar Spatial Catheter Stability as Compared to Ablation in Sinus Rhythm with Atrial Pacing
Matthew Dai, Chirag Barbhaiya, Anthony Aizer, Jonathan Hyde, Edward Kogan, Douglas Holmes, Scott Bernstein, Michael Spinelli, David S. Park, Larry A. Chinitz, Lior Jankelson
From the Leon H. Charney Division of Cardiology, Cardiac Electrophysiology, NYU Langone Health, New York University Grossman School of Medicine, NY, USA..
Improved catheter stability is associated with decreased arrhythmia recurrence after atrial fibrillation (AF) ablation. Recently, atrial voltage mapping in AF was demonstrated to correlate better with scar as compared to mapping in sinus rhythm (SR). However, it is unknown whether ablation of persistent AF in sinus rhythm with atrial pacing or in atrial fibrillation with ventricular pacing results in differences in catheter stability or arrhythmia recurrence.
We analyzed 53 consecutive patients undergoing first-time persistent AF ablation with pulmonary vein and posterior wall isolation: 27 were cardioverted, mapped, and ablated in sinus rhythm with atrial pacing, and 26 were mapped and ablated in AF with ventricular pacing. Ablation data was extracted from the mapping system and analyzed using custom MATLAB software to determine high-frequency (60Hz) catheter excursion as a novel metric for catheter spatial stability.
There was no difference in catheter stability as assessed by maximal catheter excursion, mean catheter excursion, or contact force variability between the atrial-paced and ventricular-paced patients. Ventricular-paced patients had significantly greater mean contact force as compared to atrial-paced patients. Contact-force variability demonstrated poor correlation with catheter excursion. One year arrhythmia-free survival was similar between the atrial paced and ventricular paced patients.
For patients with persistent AF, ablation in AF with ventricular pacing results in similar catheter stability and arrhythmia recurrence as compared to cardioversion and ablation in sinus rhythm with atrial pacing. Given the improved fidelity of mapping in AF, mapping and ablating during AF with ventricular pacing may be preferred.
Key Words : Atrial Fibrillation, Ablation, Stability, Excursion.
Lior Jankelson. Leon H. Charney Division of Cardiology, Cardiac Electrophysiology, NYU Langone Health, New York University Grossman School of Medicine, NY, USA
Radiofrequency (RF) ablation is a widely accepted and effective therapy in the management of atrial fibrillation (AF)1–3. However, ablation of persistent atrial fibrillation remains a therapeutic challenge, with recurrence rates of 30-60% at one year, and a frequent need for repeat ablation.4–7 Improved catheter stability results in more consistent catheter-tissue contact, both allowing for more effective transmural lesion formation and preventing excessive force that could result in cardiac perforation. Furthermore, improved catheter stability has been shown to be associated with decreased arrhythmia recurrence following AF ablation.8 Multiple strategies and techniques exist for improving catheter stability, including high frequency jet ventilation9–11, steerable catheter sheaths11–13, and rapid atrial pacing14. However, catheter stability may be affected by the underlying atrial rhythm. In patients with persistent AF, achieving stable sinus rhythm and reliable atrial pacing may be challenging prior to ablation, and pacing can only be performed in the ventricle. It is unknown whether ablation in AF with ventricular pacing versus in sinus rhythm (SR) with atrial pacing has any effects on catheter stability, lesion quality, or clinical outcomes. In the present study, we sought to compare the ablation characteristics and clinical outcomes between patients with persistent AF who were mapped and ablated in sinus rhythm with atrial pacing compared to atrial fibrillation with ventricular pacing.
We identified 53 consecutive patients at a single experienced electrophysiology center who underwent first time RF ablation for persistent AF. Of these, 27 were cardioverted then mapped and ablated in sinus rhythm with atrial pacing. Guided by operator preference or due to failure of initial cardioversion, 26 patients were mapped and ablated in AF with ventricular pacing. Pacing was performed at a cycle length of 500-600ms, regardless of pacing site. All procedures were performed under general anesthesia with high frequency jet ventilation. Electroanatomical mapping was performed using either the circular Lasso® or five-spine PentaRay® mapping catheter and the CARTO3® mapping system, version 4 (Biosense Webster Inc., USA). Radiofrequency ablation was performed using the ThermoCool SmartTouch® force-sensing catheter (Biosense Webster Inc., USA) using point-by-point ablation at a power of 50W. All patients underwent pulmonary vein isolation (PVI) via wide antral circumferential ablation of the left and right pulmonary veins, as well as posterior wall isolation (PWI) via superior and inferior posterior wall lines connecting the PVI lesion sets. Additional ablation of the left and right carinas and/or residual electro-active areas within the posterior wall were performed at the discretion of the operator. VisiTag lesion stability settings were set to 2mm and 5s. Electrical isolation, including entrance and exit block, was confirmed using differential pacing and adenosine administration.
Ablation analysis and catheter spatial stability
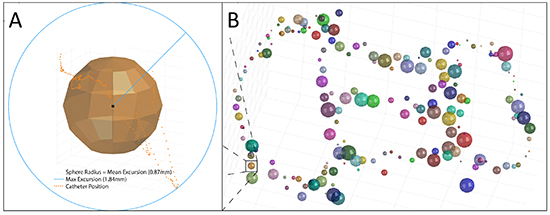
Our group had recently described a method for precise analysis of catheter-tip spatial stability, utilizing custom developed MATLAB script applied on X-Y-Z axis tip position data acquired at 60Hz8. Briefly, ablation data was extracted from CARTO® and analyzed using custom MATLAB script (Mathworks, USA). For each ablation lesion, the mean 3-dimensional (3-D) catheter position was calculated, and catheter excursion was defined as the distance between each recorded position of the catheter tip, sampled at 60Hz, to the mean 3-D catheter position for the lesion. Thus for calculation of excursion relative to a reference, we set the reference as the exact center in space of the entire “cloud” of positions recorded at 60Hz for each lesion. The mean and maximal catheter excursion were then calculated for each lesion (see [Figure 1]). Contact force variability was defined as the standard deviation of the contact force for the lesion.
Figure 1. Example ablation lesion set with excursion measures. A) For each ablation lesion, catheter position was sampled at 60Hz. The orange dotted trail represents all sampled positions during a single RF lesion. Mean and maximal catheter excursion were calculated for each ablation lesion, and the radius of each sphere represents the mean catheter excursion for that lesion. B) All patients underwent pulmonary vein isolation and posterior wall isolation. Full lesion set is projected with the left atrium removed. Sphere colors randomly assigned to enhance visibility.
Ablation and clinical endpoints
The primary ablation endpoint was catheter stability, defined by mean and maximal catheter excursion. The secondary clinical endpoint was one year freedom from AF recurrence, following a 3-month blanking period. Recurrence was defined as an atrial arrhythmia lasting longer than 30 seconds on ambulatory monitoring, or an atrial arrhythmia documented on a standard 12 lead electrocardiogram. Recurrences within 3 months were included if they necessitated a repeat ablation.
All statistical analysis was performed using SPSS Statistics 26 (IBM Corp., USA) and graphs were constructed using Prism 8 (GraphPad Software Inc., USA). Continuous variables are expressed as mean ± standard deviation, and categorical variables are expressed as percentages. Normality of data samples was assessed using Shapiro-Wilk test. Two sample hypothesis testing was performed using either Student’s t-test if samples had normal distributions or Mann-Whitney U test if samples did not have normal distributions. Hypothesis testing for categorical variables was performed using Fisher’s exact test. For Kaplan-Meier survival analysis, significance testing between groups was performed using log-rank test. For comparison between CF variability and catheter excursion, Pearson’s correlation coefficient was calculated.
All patients provided written informed consent for their procedures, and all data collection and analysis was approved by the NYU Langone Medical Center Institutional Review Board.
Catheter stability and ablation characteristics
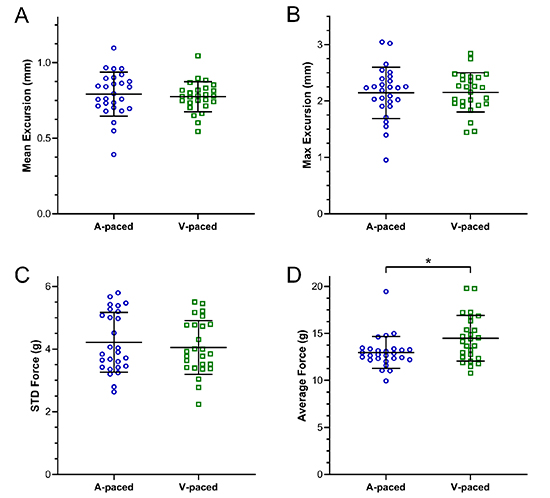
Baseline patient characteristics are provided in [Table 1]. Ventricular-paced patients had significantly larger left atrial diameters (4.9 ± 0.6cm vs 4.4 ± 0.8cm, p = 0.02), but similar left atrial volume indices (41 ± 15mL/m2 vs 33 ± 8mL/m2, p = 0.14), as well as greater time since initial diagnosis of AF (4.4 ± 4.7yrs vs 2.5 ± 4.2yrs, p = 0.02), compared to atrial-paced patients. Otherwise, there were no significant clinical or echocardiographic differences between the two groups. With respect to ablation characteristics [Table 2], there were no significant differences in measures of catheter stability between the atrial-paced and ventricular-paced patients. Atrial-paced patients had similar mean catheter excursions (0.79 ± 0.15mm vs 0.77 ± 0.10mm, p = 0.62), maximal catheter excursions (2.14 ± 0.45mm vs 2.15 ± 0.35mm, p = 0.94), and contact force variability (4.2 ± 1.0g vs 4.1 ± 0.9g, p = 0.58), compared to ventricular-paced patients [Figure 2]. In addition, the two groups had similar mean absolute impedance declines (7.7 ± 1.5ohms vs 7.1 ± 1.7ohms, p = 0.15) and percentage impedance declines (6.3 ± 1.2% vs 5.8 ± 1.2%, p = 0.12). Ventricular-paced patients had slightly greater average contact forces than atrial-paced patients (14.5 ± 2.4g vs 13.0 ± 1.7g, p = 0.02) as well as greater force-time-integrals (FTIs, 107 ± 20 gs vs 95 ± 15gs, = 0.02), which was driven by the greater contact forces.
Table 1. Baseline Clinical Characteristics
|
Overall (n = 53) |
A-paced (n = 27) |
V-paced (n = 26) |
p |
| Sex (% male) |
74% (39/53) |
74% (20/27) |
73% (19/26) |
1 |
| Age (yrs) |
63 ± 12 |
64 ± 10 |
62 ± 14 |
0.92 |
| BMI (kg/m2) |
30.7 ± 6.5 |
29.3 ± 4.6 |
32.1 ± 7.8 |
0.12 |
| LVEF (%) |
55 ± 12 |
57 ± 12 |
53 ± 13 |
0.11 |
| LA Diameter (cm) |
4.6 ± 0.7 |
4.4 ± 0.8 |
4.9 ± 0.6 |
0.02 |
| LA Volume Index (mL/m2) |
37 ± 13 |
33 ± 8 |
41 ± 15 |
0.14 |
| Years Since AF Diagnosis |
3.4 ± 4.5 |
2.5 ± 4.2 |
4.4 ± 4.7 |
0.02 |
|
|
|
|
|
| CHA2DS2-VASc |
2.1 ± 1.7 |
2.0 ± 1.6 |
2.2 ± 1.7 |
0.78 |
| HTN |
62% (33/53) |
59% (16/27) |
65% (17/26) |
0.78 |
| DM |
15% (8/53) |
19% (5/27) |
12% (3/26) |
0.7 |
| CHF |
21% (11/53) |
22% (6/27) |
19% (5/26) |
1 |
| CVA |
6% (3/53) |
4% (1/27) |
8% (2/26) |
0.61 |
| Vascular Disease |
4% (2/53) |
7% (2/27) |
0% (0/26) |
0.49 |
| OSA |
36% (19/53) |
37% (10/27) |
35% (9/26) |
1 |
|
|
|
|
|
| Post-Ablation Medications |
|
|
|
|
| Anti-arrhythmic |
87% (46/53) |
81% (22/27) |
92% (24/26) |
0.42 |
| BB or CCB |
85% (45/53) |
78% (21/27) |
92% (24/26) |
0.25 |
|
|
|
|
|
| Post-Ablation Monitoring |
|
|
|
|
| ILR, PPM, or ICD |
11% (6/53) |
11% (3/27) |
12% (3/26) |
1 |
| Number of Monitors |
2.3 ± 1.1 |
2.4 ± 1.0 |
2.1 ± 1.2 |
0.41 |
BMI = body mass index, LVEF = left ventricular ejection fraction, LA = left atrium, AF = atrial fibrillation, HTN = hypertension, DM = diabetes mellitus, CHF = congestive heart failure, CVA = cerebrovascular accident, OSA = obstructive sleep apnea, BB = beta-blocker, CCB = calcium channel blocker, ILR = implantable loop recorder, PPM = permanent pacemaker, ICD = implantable cardioverter-defibrillator
Table 2. Ablation Characteristics
|
Overall (n = 53) |
A-paced (n = 27) |
V-paced (n = 26) |
p |
| Count |
146 ± 44 |
136 ± 37 |
156 ± 49 |
0.10 |
| Lesion Duration (s) |
7.4 ± 0.8 |
7.4 ± 0.7 |
7.4 ± 0.8 |
0.53 |
| Average Force (g) |
13.7 ± 2.2 |
13.0 ± 1.7 |
14.5 ± 2.4 |
0.02 |
| Contact Force Variability (g) |
4.1 ± 0.9 |
4.2 ± 1.0 |
4.1 ± 0.9 |
0.58 |
| Max Power (W) |
51.1 ± 1.0 |
51.2 ± .4 |
50.9 ± 1.4 |
0.22 |
| Base Impedance (ohms) |
120 ± 14 |
120 ± 12 |
120 ± 16 |
0.90 |
| Impedance Decline (ohms) |
7.4 ± 1.6 |
7.7 ± 1.5 |
7.1 ± 1.7 |
0.15 |
| Percent Impedance Decline |
6.0 ± 1.2% |
6.3 ± 1.2% |
5.8 ± 1.2% |
0.12 |
| FTI (gs) |
101 ± 19 |
95 ± 15 |
107 ± 20 |
0.02 |
| Mean Excursion (mm) |
0.78 ± 0.12 |
0.79 ± 0.15 |
0.77 ± 0.10 |
0.62 |
| Max Excursion (mm) |
2.15 ± 0.40 |
2.14 ± 0.45 |
2.15 ± 0.35 |
0.94 |
Contact force variability was defined as the standard deviation of the contact force. FTI = force time integral
Figure 2. Measures of catheter stability in atrial-paced and ventricular-paced patients. There was no significant difference in mean excursion (A), maximal excursion (B), or standard deviation of contact force (C) between the two groups. Ventricular paced patients had significantly greater average contact force, compared to atrial paced patients (p = 0.02) (D).
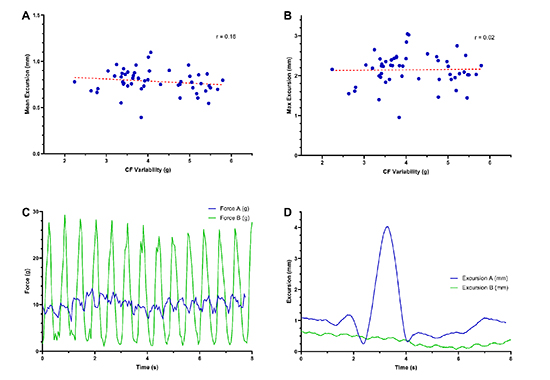
Contact force variability demonstrated poor correlation with catheter excursion, r=0.16 and 0.02 for mean and maximal excursion, respectively.
Procedure characteristics
Compared to atrial-paced patients, ventricular-paced patients had a non-significant trend towards increased total procedure time (169 ± 34min vs 151 ± 36min, p = 0.08). There was no significant difference in RF time (43 ± 13min vs 41 ± 13min, p = 0.64) [Table 3]. There no procedural complications.
Table 3. Procedure Characteristics
|
Overall (n = 53) |
A-paced (n = 27) |
V-paced (n = 26) |
p |
| RF Time (min) |
42 ± 13 |
41 ± 13 |
43 ± 13 |
0.64 |
| Total Procedure Time (min) |
160 ± 36 |
151 ± 36 |
169 ± 34 |
0.08 |
| Number of DCCVs |
1.0 ± 0.7 |
0.8 ± 0.6 |
1.2 ± 0.7 |
0.09 |
| ≥2 DCCVs (%) |
19% (10/53) |
11% (3/27) |
27% (7/26) |
0.18 |
RF = radiofrequency, DCCV = direct current cardioversion
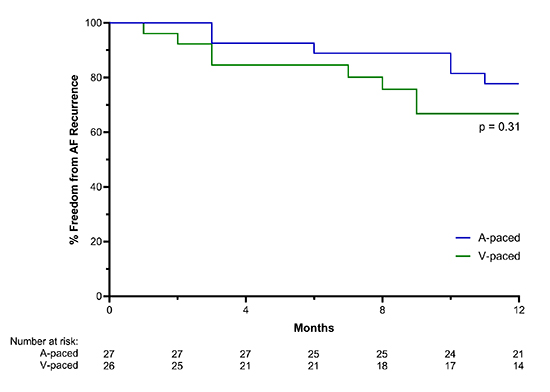
48 of 53 (91%) patients completed 1 year follow up, with an average follow up length of 11.5 ± 1.9 months. Follow up length was similar between the two groups. Overall 6 patients (11%) had long term continuous monitoring with an implantable device (PPM, ICD, or ILR), equally distributed between groups. The remaining patients underwent 1 or 2-week ambulatory event monitoring at 3, 6, and 12 months post-procedure (average 2.3 ± 1.1 monitors). 87% of patients were maintained on an anti-arrhythmic medication (Amiodarone, Dronedarone, or Flecainide) for one month post-procedure, and 85% of patients were continued on long term beta-blocker and/or calcium channel blocker therapy [Table 1]. One year arrhythmia-free survival was similar between the atrial-paced and ventricular-paced patients (78% vs 67%, p = 0.31) [Figure 3].
Figure 3. One year arrhythmia free survival. There was no significant difference in one year arrhythmia free survival between the atrial-paced and ventricular-paced patients (78% vs 67%, p = 0.31).
In this study, we utilized a novel ablation data analytic tool to determine if pacing site and the rhythm during AF ablation affect procedural characteristics, and most importantly catheter spatial stability. We have recently demonstrated that improved catheter spatial stability is associated with lower rates of arrhythmia recurrence after AF ablation8. Therefore, it is important to understand the interaction of the atrial rhythm during AF ablation and catheter spatial stability.
The prevailing method for assessing catheter stability is indirect, via contact force variability. In our work we utilize a direct and precise method for stability assessment, based on excursion. As depicted in [Figure 4], CF variability and spatial stability as measured by excursion analysis can be completely dissociated: while force variability may be minimal, implying good catheter stability, large excursions may be present, reflecting highly unstable catheter position of the catheter during lesion placement. Atrial pacing has been demonstrated to enhances catheter stability compared to sinus rhythm14,15. Pacing at an accelerated ventricular rate reduces contact force variability and increases the proportion of time within a pre-specified contact force range. Our data, directly analyzing catheter stability through three dimensional positional excursion rather than indirectly by contact force, suggests that catheter ablation during atrial fibrillation with ventricular pacing, compared to sinus rhythm with atrial pacing, does not result in significant differences in spatial stability and lesion quality markers. Despite the difference in the underlying atrial rhythm, measures of catheter spatial stability were similar between the two groups. There were no differences in impedance decline between atrial paced and ventricular paced patients, further evidence that the ventricular rate and regularity are major determinants of catheter stability.
Figure 4. Catheter spatial stability as excursion vs. contact force variability. A, B demonstrate the poor correlation between CF variability and catheter excursion. C, D represent an example for the dissociation between CF variability and catheter excursion. While CF variability is high for point A, excursion is low (green tracings panel C and D). Vice versa, for point B the CF variability is low while excursion is high (blue tracings panel C and D).
Ventricular-paced patients had longer procedure times and trended towards a greater number of electrical cardioversions. This can be explained by the fact that some patients in this group had unsuccessful cardioversion attempts at the beginning of the procedure, which led to the decision to perform ablation in AF with ventricular pacing instead. All ventricular-paced patients in our study were successfully cardioverted to sinus rhythm by procedure end.
Performing mapping and ablation while in AF with ventricular pacing may have benefits to persistent AF ablation beyond catheter stability. Underlying atrial myopathy and fibrosis, particularly within the posterior wall of the left atrium, can serve as additional triggers and propagators of persistent AF. A recent study by Qureshi et al.16 found that mapping during atrial fibrillation as compared to sinus rhythm, may enhance the identification of low voltage regions that correlate with atrial fibrosis on cardiac MRI 27. Thus mapping in AF may provide additive invaluable information regarding arrhythmogenic substrate and may facilitate refining of the ablation strategy, without compromising catheter stability.
With regards to hemodynamic implications of pacing, as the typical heart rate is kept at 100 beats per minute, allowing adequate ventricular filling, no instances of pacing related hemodynamic instability are expected.
Overall one year arrhythmia-free survival was 73%, which is in line with previous data for persistent AF ablation4,6,7. There was no significant difference in recurrence between the atrial-paced and ventricular-paced patients, but this should be seen within the power limitation of the cohort. The ventricular-paced patients had significantly greater LA diameters, time since AF diagnosis, as well as trend toward greater LA volume indices and lower LV ejection fraction. These measures have been shown to be associated with increased arrhythmia recurrence17-20 thus sample size may have confounded recurrence outcomes.
This was a retrospective study of a consecutive cohort with a follow up time of 1 year. It is possible that the lack of statistically significant difference in arrhythmia recurrence is the result of a relatively small sample size. Likewise, logistic regression analysis to assess for predictors of arrhythmia recurrence was not possible. Patients ablated in AF with ventricular pacing may represent a subset with more complex substrate, evident by resistance to DCCV.
Ablation of persistent atrial fibrillation in atrial fibrillation with ventricular pacing, compared to sinus rhythm with atrial pacing, results in similar spatial catheter stability and lesion quality as assessed by impedance decline and ablation parameters. Given the recent evidence suggesting voltage mapping during atrial fibrillation may provide more accurate assessment of atrial fibrosis, it may be preferable, at least in patients presenting in AF, to ablate during atrial fibrillation with ventricular pacing, and defer cardioversion until after procedure completion.






