Dynamic Local Activation Time Mapping in Heavily Scarred Left Atrium and Persistent Atrial Fibrillation: A proof of concept case report
Benjamin Mac Curtain12, James Mannion13, Santhosh David4, Roger Byrne1, Usama Boles1
1Heart and Vascular Centre, Cardiology Department, Mater Private Hospital, Dublin 7, Ireland.2Royal College of Surgeons in Ireland,University of Medicine and Health Sciences, School of Medicine, Dublin 2, Ireland.3University Hospital Waterford, Co. Waterford, Ireland.4Letterkenny University Hospital, Co Donegal, Letterkenny, Ireland.
We report the case of a 68-year-old male, presenting with persistent atrial fibrillation (Pe AF) refractory to anti arrhythmic medications and cardioversion, on a background history of ischaemic heart disease. Pre and post standard pulmonary vein isolation (PVI), left atrial (LA) voltageanalyses wereperformed, followed by dynamic local activation time (DLAT) mapping in addition to focal activity identification.Thisdemonstrated a heavily scarred LA, and a number ofareas of focal activity.
The patient remained in atrial fibrillation (AF) post rotor (focal activity) targeting,howevernotable changes in AF cycle length (CL)werenotedandslowed by an average of 25.3 milliseconds.
Comparison between DLAT mappingpre and post PVI were anatomically similar but not identical. The anatomical distribution of heavy scar areas in the LA did not correspond to the DLAT areas of interest.
The patient subsequentlyremained in normal sinus rhythm (SR) for 6 monthson a low dose Beta blockade in a short follow up period. DLAT mapping and its characteristics in heavily scarred LA are reported in this case.
Key Words : Catheter Ablation, Atrial fibrillation, Rotational Activities, Left Atrial Scar, Dynamic Late Activation Time.
Correspondence to: Dr Usama Boles MB, BCH, MSc, PhD, FRCPI, FESC, FHRS
Cardiologist and Electrophysiologist
Heart and Vascular Centre, Atrial Fibrillation Institute,
Cardiology Department,Mater Private hospital,
Dublin, Ireland
While success rates regarding PVI for PeAF have been reported to be as low as 50%, there has also been literature reporting higher procedure success rates targeting LA substrates and macro re-entry circuits 1. DLAT is a new concept to identify active rotors in the left atrial body. It has been shown that using DLAT to target focal or rotational points of interest can help to retore SR in AF 2. The role of DLAT in restoring SR in heavily scared LA is not fully documented, and hence this case servesto highlight thisadd-on technique.
This case report presents a 68 year old male, presenting on a background history of ischemic heart disease, with Pe AF, refractory to anti-arrhythmic medications (i.e. beta blocker and amiodarone)and electrical cardioversion, 3 months prior. He presented to the emergency department with worsening dyspnoea and was subsequently found to have an elevated brain natriuretic peptide (BNP).
The patient was brought in for an ablation procedure under general anaesthetic. Catheter access was achieved through the right femoral vein. Intra cardiac echocardiography (ICE) (Biosense Webster, Inc., Diegem, Belgium) was used to guide transseptal puncture using a BRK0 needle (Abbott Vascular, Santa Clara, California,USA).A Multipolar PentarayEco Catheter, (Biosense Webster, Inc., Diegem, Belgium) was used in atrial endocardium mapping. The Pentarray is a 7F catheter and has 22 poles distributed evenly throughout 5 splines at the tip of the catheter.
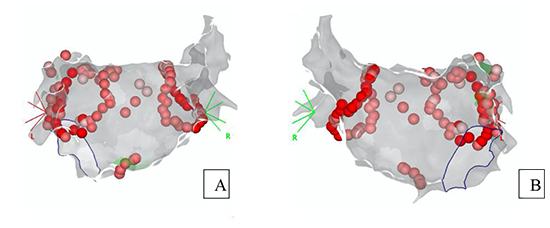
For DLAT mapping thePentarray multielectrode catheter was required to maintain a consistent position for a period of 30 seconds to analyse the rotational activity. A standard 30-35 Watts were used for the ablation to achieve an ablation index of 500 anteriorly and 400 posteriorly, respectively 3.Standard ablation was performed as a wide antral circumferential ablation (WACA) continuous line, first. Then,DLAT was measured using Cartofinder(CF) (BiosenseWebster, Inc., Diegem, Belgium) pre and post PVI. These images can be seen in the Results section. The ablation sites can be observed below in [Figure 1A] and [Figure 1B].
Figure 1A and 1B. Anterior and posterior views of the PVI (pulmonary vein isolation) and DLAT (dynamic local activation time) radiofrequency ablation sites. The PVI was performed as standard. Rotational / focal activity was detected using DLAT and these areas were further targeted for ablation. These areas can be seen at the atrial roof, left superior pulmonary vein, superior and mid posterior wall, peri-mitral area and around the left atrial appendage base.
Voltage mapping was created simultaneously with LA geometry pre and post PVI. Post PVI was done to confirm complete bidirectional block at the pulmonary veins antral region.
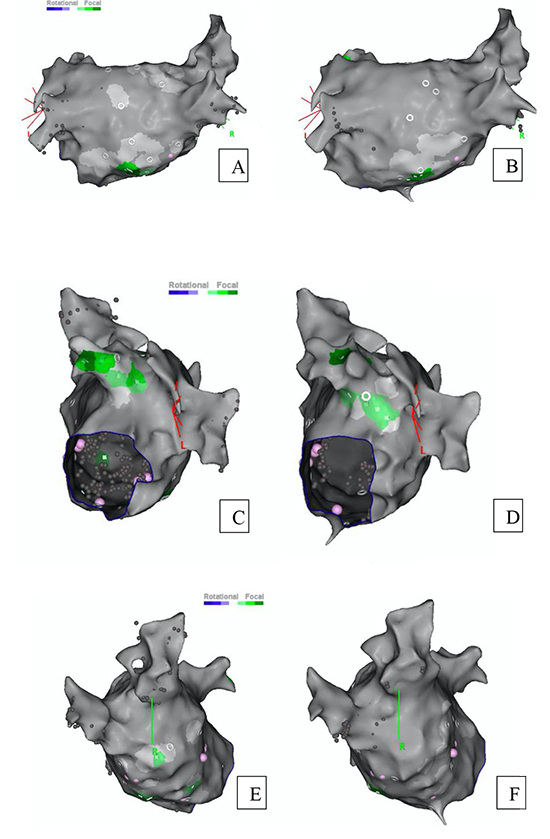
Mapping identified focal activities in theLAroof close to the left superior PV, base of left atrial appendage (LAA), posterior wall and peri-mitral to septal LA regions as seen in [Figure 2]. No rotational activities were identified.
Figure 2. PA view of Pre (A) and Post (B) PVI (pulmonary vein isolation) DLAT (dynamic local activation time) images from CF (Carto finder). Both revealed a target in the peri mitral posterolateral regions. LAA view of Pre (C) and Post (D) PVI DLAT images from CF. The green colour indicates a target area for ablation and a critical isthmus for the focal activity. RL view of Pre (E) and Post (F) PVI DLAT images from CF. The peri mitral activity was more frequent in pre PVI in image E (note the green areas)
The average Cycle length (CL) was seen to slow by25.3 3.9 milliseconds (ms)after ablation as seen in [Table 1]. The greatest slowing in CL can be observed vicinity of the LAA area. In addition, the number of interest points targeted pre and post PVI were different due to disappearance of DLAT activity at the roof of the LA closer to right pulmonary veins post WACA isolation. Although it is a small sample size, the magnitude of CL slowing does not seem related to ablation time. There is a clear decrease in driver points identified post PVI in the mid anterior-inferior LA, Anteroseptal LA, mid to right roof LA and LAA roof. An increase in the points of interest can be observed in the LAA basolateral area.
Table 1. DLAT (Dynamic local activation time) Drivers pre and post ablation: The anatomical location of the drivers is given, as well as if the driver was detected pre and post ablation. The type of driver, ie Rotational or focal is also categorised. The average local cycle lengths (CL) are also detailed as well as the change in CL in ms. Ablation duration is also displayed.
| Location of DLAT |
Driver Type |
Driver identified (Pre ablation) |
Driver identified (Post ablation) |
Average local CL pre ablation (ms) |
Average local CL post ablation (ms) |
Ablation Duration (ms) |
∆ CL (ms) |
| Mid Anterior-Inferior LA |
Focal |
6 |
2 |
167 |
194 |
67 |
-27 |
| Anteroseptal LA |
Focal |
3 |
1 |
170 |
192 |
55 |
-22 |
| Mid to right roof LA |
Focal |
6 |
0 |
171 |
NA |
NA |
NA |
| LAA basolateral |
Focal |
4 |
5 |
170 |
192 |
193 |
-22 |
| LAA roof |
Focal |
3 |
2 |
171 |
201 |
87 |
-30 |
| Mean +/- SD |
NA |
4.4 +/- 1.5 |
2+/-1.9 |
169.8+/-1.6 |
194.8+/-4.3 |
100.5 +/-63 |
-25.3+-3.9 |
*DLAT= dynamic local activation timing, PVI = Pulmonary vein isolation,Δ CL= differences in cycle length, LA = left atrium, LAA = left atrial appendage.
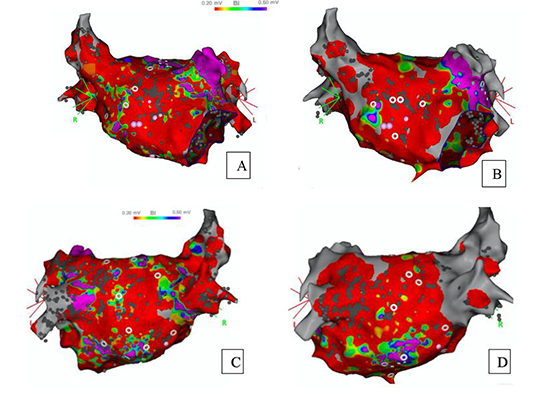
Voltage maps show visually, the LA is extensively scarred when scar is identifiedas voltages lower than 0.5mV (i.e. red colour). Comparing the images in [Figure 2]to
[Figure 3A, 3B, 3C, and 3D] they do not necessarily correlate to low voltage, or scar tissue either. Examining A and B, we can see a further example of focal DLAT points correlating visually to areas of non-scarred endocardium.
Figure 3A, 3B, 3C, and 3D. Anterior LA view of Pre (A) and Post (B) PVI (pulmonary vein isolation) voltage mapping. Posterior LA(Left atrial) view of Pre (C) and Post (D) PVI voltage mapping . Red colourcorresponds to heavily scarred area where voltages are below 0.5mV. Both visually indicate heavy scar of LA.
Around2% of the entire population suffer from AF, and of those, 25% are categorised as PeAF4. Many strategies were adopted for PeAF ablation to increase the success rate, such as substrate modification and fractionated complex ablation5,PV and non-PV approaches, for example targeting ganglionated plexi have also been examined in the literature. 6posterior wall isolation. 7 andastepwise approach is recommended yet,PVI remains the mainstay of treatment8.
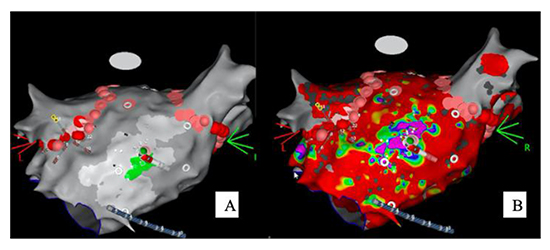
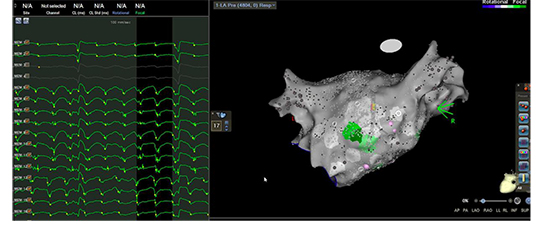
Figure 4. Intraprocedural image displaying the focal activity measured by CF (Carto finder)(left) corresponding to healthy and non-scarred endocardium on the electroanatomical map in Postero-inferior region.
Dynamic Local Activation (DLAT) mapping is a relatively new approachjust introduced using a technology called CF. This is an additional module to complement the standard ablation protocols. It works by measuring unipolar signals for a given point for 30 seconds using a multipolar diagnostic catheter. These signals are further processed to remove unwanted data, such as ventricular signals. Using the 2 electrodes in closest proximity to the measured point and generating bipolar signals from these points, noise is removed.
Any unipolar signals from the atrium that fits within the bipolar signal range from the earliest onset to the latest offset (Bipolar electrogram (EGM) window) are included in the wavelet analysis as displayed below in [Figure 5] which is an example of the DLAT from this case. DLAT is shown in 250 ms sections in relation to the 30 second measurement window. It is calculated as the maximal negative slope of the atrial unipolar signal within the bipolar range mentioned above 9. Focal signals are measured by determining unipolar signals that have a QS pattern. Each of these QS patterns within a 10-millimetre (mm) radius and 50 ms window are measured. If one of these occurs two or more times they are counted as focal areas of interest. The area of interest, in terms of rotational points, is determined by measuring rotational signals by relating CL to its conduction wave and EGMs. If these EGM patterns fit the preprogramed “head meets tails” pattern of the algorithm then they are graphically displayed as a rotational point of interest 10. Of note, both micro and macro re-entry circuits are identified by the software analysis. Macro re-entry, or rotational circuits may correlate to areas of lesser scar tissue and hence better long terms prognosis, thisnotion may be examined in future studies.
Figure 5. DLAT (Dynamic local activation time) wavelets and corresponding areas of focal activity. The EGMs (electrogram) on the left correspond to the focal point of interest displayed. A recording is taken for 30 seconds and is filtered to remove noise and ventricular signals. The noise is removed by generating bipolar signals from the unipolar signals and creating a bipolar EGM window. LAT is calculated using wavelet analysis on the unipolar signals that falls within this bipolar EGM window and is dispalyed within fixed 250 ms windows.
Rationale for DLAT mapping and ablation for this case
In PeAF it has been put forward that an array of wavelets, re-entrant and focal sources are driving factors for the disease in addition to pulmonary veins potentials9. This may be caused by structural remodelling as a result of initial focal electrical activity. Furthermore, this structural remodelling may cause electrical remodelling, creating a positive feedback cycle11.
It has also been postulated that AF may be driven by fibrillatory conduction stemming from focal activity. As well as this, re-entry circuits causing a shortened CL have also been linked to the disease 12. These two patterns, either focal or rotational are distinct from one another in the sense that the electrical activity propagates in a rotational pattern for the so called “rotational” activity while the “focal” activity refers to a waveform that is detected and spreads in a radial pattern 13.The focal activity in AF has been shown tooccur due to an endocardial and epicardial mismatch 14, 15. Scaring has been shown to increase this endocardial and epicardial mismatch, possibly explaining our focal activity results 16. Rotational activity has been defined as a 360 degree rotation of 1.5 times while focal activity has been defined as a pattern propagating radially for 2 or more consecutive waveforms 2. Focal and rotational patterns have been observed to maintain a constant location, however, they may vary with the timing of measurement 17.
Some previous work has tried to examine the relationship between rotor activity and scar tissue in the atriausing voltage as a marker for degree of scarring. It was found that the degree of rotational activity complexity was directly correlatedto the degree of scarring present, in analysing 28 patients with Pe AF18. It has also been suggested that the use of further measurements to target scar tissue may be helpful in improving outcomes for patients with scarred atrial tissue 19.
The usability of DLAT mapping techniques in heavily scarred atria has been questioned due to its low voltage and inherently fragmented waveforms 1. This use of a focal and rotational electrical activity approach in PVI, may improve clinical outcomes when correlated with standard electroanatomical mapping. Honarbakhsh et al found that while most rotational activity picked up by DLAT was associated with minimally scarred endocardium, PVI did not significantly alter AF CL in these areas. 2. Pre and post PVI CL to determine the effect of ablation on CL at the DLAT points of interest in a heavily scarred atrium is displayed in [Table 1].
Procedure response in previous studies has been considered CL slowing more than or equal to 30 ms or else AF termination upon ablation 20. In this case ablation of the DLAT points of interest did not result in conversion to SR butthe average AF CL was seen to slow by 25.3 ms. The patient has not developed AF through the 6-month period post ablation.
In summary of this case we report a 68 male who suffers from symptomatic PeAF refractory to cardioversion and anti-arrhythmic medications. We evaluated this relatively new approach of rotational and focal activity mapping and ablation. We identified a mean of 4.4 areas of interest per region of interest that reduced to a mean of 2 areas of interest per region post standard WACA. Targeting those focal activities resulted in slowing the CL of AF. A short follow up period revealed apparent success of procedure, with de-escalation of his anti-arrhythmic medications.
In our case, DLATin Pe AF served as an additional strategy to improve success in themaintenance of normal SRpost ablation. Heavilyscarredleft atrialtissue has revealed points of only focal, not rotational, activity to target.Further large scale trials examining this approach in heavily scarred atrial tissue are warranted relatively new strategy may have a promising impact to maintain normal SR.






