Left Atrial Appendage Occlusion Device Embolization (The LAAODE Study): Understanding the Timing and Clinical Consequences from a Worldwide Experience
Ghulam Murtaza2, Mohit K. Turagam15, Tawseef Dar14, Krishna Akella2, Bharath Yarlagadda3, Steffen Gloekler4, Bernhard Meier4, Jacqueline Saw5, Jung-Sun Kim6, Hong-Euy Lim7, Nietlispach Fabian8, James Gabriels9, Lucas V. Boersmaj10, Martin J. Swaans10, Mohmad Tantary11, Sibghat Tul Llah12, Apostolos Tzikas13, Rakesh Gopinathannair2, Dhanunjaya Lakkireddy2
1Department of Cardiology, Icahn School of Medicine at Mount Sinai, New York, NY.2Kansas City Heart Rhythm Institute and Research Foundation, Overland Park, Kansas.3Division of Cardiology, University of New Mexico.4Department of Cardiology, University Hospital of Bern, Bern, Switzerland.5Division of Cardiology, Vancouver General Hospital, University of British Columbia, Vancouver, British Columbia, Canada.6Division of Cardiology, Severance Cardiovascular Hospital, Yonsei University College of Medicine, Seoul, Korea.7Division of Cardiology, Cardiovascular Center, Korea University Guro Hospital, Korea University College of Medicine, Seoul, Korea.8University Heart Center, University Hospital Zurich, Zurich, Switzerland.9Department of Cardiology, Northwell Health, North Shore University Hospital, NY, USA.10Department of Cardiology, St. Antonius Hospital, Nieuwegein, the Netherlands.11Clinch Valley Medical Center, Virginia, USA.12Saint Joseph hospital and Medical Center, Phoenix, Arizona.13AHEPA University Hospital, Thessaloniki, Greece; Interbalkan European Medical Center, Thessaloniki, Greece.14Massachusetts General Hospital, Boston, Massachusetts.15Department of Cardiology, Garden City Hospital, Garden City, Michigan.
Left atrial appendage occlusion device embolization (LAAODE) is rare but can have substantial implications on patient morbidity and mortality. Hence, we sought to perform an analysis to understand the timing and clinical consequences of LAAODE.
A comprehensive search of PubMed and Web of Science databases for LAAODE cases was performed from October 2nd, 2014 to November 1st, 2017. Prior to that, we included published LAAODE cases until October 1st, 2014 reported in the systematic review by Aminian et al.
103 LAAODE cases including Amplatzer cardiac plug (N=59), Watchman (N=31), Amulet (N=11), LAmbre (N=1) and Watchman FLX (N=1) were included. The estimated incidence of device embolization was 2% (103/5,000). LAAODE occurred more commonly in the postoperative period compared with intraoperative (61% vs. 39%). The most common location for embolization was the descending aorta 30% (31/103) and left atrium 24% (25/103) followed by left ventricle 20% (21/103). Majority of cases 75% (77/103) were retrieved percutaneously. Surgical retrieval occurred most commonly for devices embolized to the left ventricle, mitral apparatus and descending aorta. Major complications were significantly higher with postoperative LAAODE compared with intraoperative (44.4% vs. 22.5%, p=0.03).
LAAODE is common with a reported incidence of 2% in our study. Post-operative device embolization occurred more frequently and was associated with a higher rate of complications than intraoperative device embolizations. Understanding the timings and clinical sequelae of DE can aid physicians with post procedural follow-up and also in the selection of patients for these procedures.
Key Words : Left atrial appendage closure device, Embolization, Atrial fibrillation, Watchman, Amplatzer cardiac plug, Amulet.
Dhanunjaya Lakkireddy, MD, FACC, FHRS
Executive Medical Director
The Kansas City Heart Rhythm Institute (KCHRI) @ HCA MidWest
12200, W 106th street, Overland Park Regional Medical Center
Overland Park, KS 66215
Percutaneous left atrial appendage closure (LAAC) has emerged as a suitable alternative for stroke prevention in non-valvular atrial fibrillation (AF) patients considered poor candidates for long – term oral anticoagulation 1. Despite its efficacy, LAAC is not devoid of complications and can be associated with increased patient morbidity and mortality 2,3. Pericardial effusion, device embolization (DE), and device thrombosis are some of the complications that are infrequently associated with LAAC. Amongst these, DE is poorly understood with a reported incidence of <4% 4. Left atrial appendage (LAA) to device size mismatch and operator experience are believed to be the most common causes for DE 5. Currently, there is limited patient-level data regarding the clinical outcomes of patients who experience DE. We therefore sought to perform a retrospective analysis of LAAC DE cases from a worldwide multi-center experience to further understand the timing and clinical consequences of DE.
We searched PubMed and Web of Science databases for eligible studies from October 2nd, 2014 to November 1st, 2017. We used the following search terms: Left atrial appendage closure, LAA closure, LAA occlusion, LAA, Watchman, Amplatzer Cardiac Plug, Amulet, Wavecrest and LAmbre. We also included the cases of LAAC DE published in the systematic review by Aminian et al (search conducted until October 1st, 2014) 5. All the corresponding authors of the cases of DE obtained through our search were contacted to obtain patient–level data regarding the respective cases and additional unpublished cases of LAAO DE that occurred during the time period.
Studies reporting at least one case of LAAC DE and any new unreported cases of DE from the search described above were included in our analysis. Editorial comments, review articles, studies reporting DE with PLAATO device and any reported or unreported cases which were also included in a larger study or trial were excluded. We only included studies involving human subjects and published in the English language.
Data extractions and quality appraisal
Two investigators (GM and MT) independently performed the literature search and screened all titles and full text versions of all the relevant studies that met study inclusion criteria. The data from the individual studies were extracted using a standardized protocol and data extraction form by two independent investigators (GM and MT). Caution was taken to make sure that there was no duplication of cases in prior studies.
Definitions
· Intraoperative device embolization: Event occurred during the procedure.
· Acute device embolization: Event diagnosed postoperatively within 24 hours.
· Subacute device embolization: Event diagnosed postoperatively after 24 hours but < 1 week
· Delayed device embolization: Event diagnosed any time after 1 week post-procedure.
· Major complication: DE that required (i) any cardiac intervention or surgery, (ii) resulted in damage to the surrounding cardiovascular structures, (iii) precipitated symptoms of angina, stroke, congestive heart failure, limb ischemia or heart block or (iv) resulted in the death of a patient.
· Minor complication: any other complication that did not meet the above criteria was considered minor complication.
· Percutaneous retrieval: was defined as device retrieval through a peripheral vascular access without any surgical cut-down.
· Surgical retrieval: was defined as any surgical technique that was used to retrieve the embolized device.
Continuous variables are expressed as mean ± standard deviation (SD) if normally distributed, and median ± Interquartile range (IQR) when deviations from normality were present. Categorical variables are expressed as counts and percentages. Categorical variables were compared between the groups using Chi-squared test or Fisher's Exact test. Continuous variables were compared using nonparametric test (Kruskal-Wallis Test). A two tailed p value <0.05 was considered statistically significant. Statistical analysis was performed using IBM SPSS Statistics version 23.0 (IBM, Armonk, New York).
Search results and data synthesis
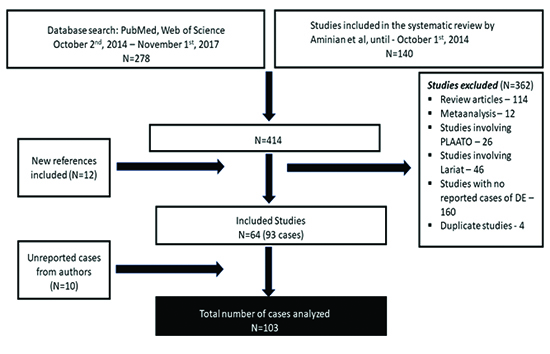
A total of 414 studies were identified during the initial literature search. Each study’s abstract was reviewed individually and screened based on study inclusion/exclusion criteria. Of these, 362 reports were excluded because of review articles (N=114), exclusive use of either the Lariat device (N=46), the PLAATO device (N=26), studies with no reported cases of DE (N=160) or duplicate studies (N=4). Finally, 64 studies reporting 93 cases were included. Patient-level data, as well as another 10 unreported cases of DE, were obtained from the individual corresponding authors of the included studies. 103 cases of DE were included in the final analysis [Figure 1].
Figure 1. Search criteria and flow diagram describing the process of case selection
Study baseline characteristics
A total of 103 cases of DE occurred from an estimated 5,000 percutaneous endocardial LAAC procedures done up until that point with an incidence of about 2%. Of these, 57% (N=59/103) occurred with Amplatzer Cardiac Plug (ACP), 30% (N=31/103) with Watchman (WM) and 11% (N=11/103) with Amulet device. One case each was reported with the investigational LAmbre and Watchman FLX devices (6,7). The median device size (IQR) in each group (ACP, WM, and Amulet) was 26 mm (IQR 24-28 mm), 24 mm (IQR 21-27 mm), and 28mm (IQR 25-31 mm), respectively. The median CHADS2 score was 4 (IQR 3-5) in ACP, 3 (IQR 3-4.5) in WM and 3 (IQR 3-5.5) in Amulet group. Median HAS-BLED scores were 3 (IQR 3-4), 3 (IQR 2.5-4), 3 (IQR 2.5-4) in each group, respectively. Other baseline characteristics of the study cohort are demonstrated in [Table 1].
Table 1. Baseline characteristics and timing of device embolization
| Variable |
Total N= 103 |
ACP N=59 |
Watchman N=31 |
Amulet N=11 |
p-value |
| Age (years) (IQR) |
75 (68-80) |
75 (68-80) |
68 (56.5-73) |
77 (74.5-85.5) |
0.15 |
| Female (%) |
14 (13.6%) |
8 (13.5%) |
2 (6.4%) |
4 (36%) |
0.13 |
| LAA size (mm) (IQR) |
20.3(18.5-24.2) |
22.8(18.8-25) |
17 ± 2.0(17-20.5) |
21.1(18.5-21.7) |
0.3 |
| Device Size (mm)(IQR) |
26(24-28) |
26(24-28) |
24(21-27) |
28(25-31) |
0.6 |
| CHADS2(IQR) |
4(3-5) |
4(3-5) |
4(3-4.5) |
3(3-5.5) |
0.9 |
| HAS-BLED(IQR) |
3.0(3-4) |
3(3-4) |
4(2.5-4) |
3(2.5-4) |
0.9 |
| Intraoperative DE |
40 (39 %) |
29 (49%) |
8 (25.8%) |
3 (27%) |
0.06 |
| Post-operative DE |
63 (61 %) |
30 (51%) |
23 (74.2 %) |
8 (73%) |
0.06 |
| Acute |
32 (50.8%) |
15 (50%) |
10 (43.5 %) |
6 (75%) |
|
| Subacute |
9 (14.3%) |
5 (16.7%) |
3 (13%) |
1 (12.5%) |
|
| Delayed |
22 (34.9%) |
10 (33.3%) |
10 (43.5%) |
1 (12.5%) |
|
ACP=amplatzer cardiac plug; IQR=interquartile range; DE= device embolization
Timing of device embolization and complications
DE occurred more commonly in the post-operative period than intraoperative period (61% vs 39 %, p=0.06). Among ACP devices, intraoperative embolization was reported in 49% (n=29/59) and post-operative in 51% (N=30/59) of cases. DE with WM and Amulet occurred predominantly in the postoperative period (74.2%; N=23/31 and 73%; N=8/11) with only 25.8 % (N=8/31) and 27% (N=3/11) occurring intraoperatively [Table 1].
In one case, DE was found on routine 6-month transesophageal echocardiography (TEE) 6. Uncomplicated DE occurred in 62% (64/103) and complicated DE occurred in 36% (37/103) of patients. Death occurred in 8 cases (8%). Bailout surgery to retrieve the device was needed in 25.2% (26/103) of cases. Of all the complicated DEs, 75.7% (28/37) were reported to have occurred in post-operative period and 24.3% (9/37) in the intraoperative period (p=0.02) [Table 2B]. The rate of major adverse events (including death) was significantly higher in patients who had postoperative DE compared with those who had intraoperative DE (44.4%; n=28/63 vs 22.5%; n=9/40: p=0.034). Furthermore, the rate of surgical intervention was 7.5% (3/40) for intraoperative DE vs 38% (23/63) for post-operative DE (p=0.016) [Table 2A]
Table 2A. Comparison of intraoperative and postoperative device embolizations
| Variable |
Intraoperative embolization N=40 |
Postoperative embolization |
P-value |
| Total N=63 |
Acute N=32 |
Subacute N=9 |
Delayed N=22 |
| Complications |
9 (22.5%) |
28 (44.4) |
12 (37.5%) |
4 (44.4%) |
12 (54.5%) |
0.034 |
| Surgery |
3 (33%) |
23 (82%) |
7 (58%) |
4 (100%) |
12 (100%) |
|
| Stroke/TIA |
2 (22%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
|
| Myocardial infarction |
1 (11%) |
2 (7%) |
2 (17%) |
0 (0%) |
0 (0%) |
|
| Cardiogenic shock |
1 (11%) |
2 (7%) |
1 (8%) |
0 (0%) |
1 (8%) |
|
| Valvular damage |
3 (33%) |
2 (7%) |
1 (8%) |
0 (0%) |
1 (8%) |
|
| Limb ischemia |
0 (0%) |
1 (4%) |
1 (8%) |
0 (0%) |
0 (0%) |
|
| Internal bleeding |
2 (22%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
|
| Death |
1 (11%) |
7 (25%) |
2 (17%) |
1 (25%) |
4 (33%) |
|
TIA=trasient ischemic attack
Table 2B. Comparison of complicated and uncomplicated embolizations
| Variable |
Complicated embolizations N=37 |
Uncomplicated embolizations N=64 |
P-value |
| Intraoperative diagnosis |
9 (24%) |
31 (48.4%) |
0.02 |
| Postoperative diagnosis |
28 (76%) |
33 (51.6%) |
0.02 |
| Acute (within 24 hours) |
12 (33%) |
20 (31.2%) |
0.37 |
| Subacute (within 1 week) |
4 (11%) |
4 (6.3%) |
|
| Delayed (after 1 week) |
12 (32%) |
9 (14.1%) |
|
| Device type |
|
|
0.31 |
| Amplatzer cardiac plug |
19 (51%) |
40 (62.5%) |
|
| Watchman |
12 (32.4%) |
17 (26.7%) |
|
| Amulet |
6 (16%) |
5 (7.8%) |
|
| Watchman FLX |
0 |
1 (1.5%) |
|
| LAmbre |
0 |
1 (1.5%) |
|
| Site of embolization |
|
|
0.002 |
| Left atrium |
2 (5.4%) |
15 (23.4%) |
|
| Left ventricle |
12 (32.4%) |
7 (11%) |
|
| Left ventricular cavity |
7 (19%) |
4 (6.2%) |
|
| Left ventricular outflow tract |
5 (13.5%) |
3 (4.7%) |
|
| Mitral valve apparatus |
4 (11%) |
3 (4.7%) |
|
| Aorta |
6 (16.2%) |
22 (34.4%) |
|
| Ascending aorta/arch of aorta |
1 (2.7%) |
5 (7.8%) |
|
| Descending/abdominal aorta |
3 (8%) |
14 (21.8%) |
|
| Aorta/iliac bifurcation |
2 (5.4%) |
3 (4.7%) |
|
Site of device embolization and complications
The most common site for embolization was the left atrium (LA) (22.5%, n=9/40) for intraoperative cases and the descending aorta/abdominal aorta (19.7%, n=12/61) for post-operative cases [Table 3]. In general, devices embolized to left ventricle (LV) and mitral valve apparatus are more likely to get complicated in comparison to other sites of embolization (p=0.002) [Table 2B]. Furthermore, devices embolized to LV and mitral valve apparatus were more likely to require surgical intervention compared to other sites (p= 0.0074). LA embolization had a 94% chance of being snared percutaneously. Overall, the trend for surgical requirement increased dramatically if the embolized device was found in the LV/left ventricular outflow tract (LVOT)/mitral valve apparatus (44.4%, n=12/27) compared to the aorta or iliac bifurcation (13.7%, n=4/29), or the left atrium (6%, n=1/17) (p=0.0074). [Table 4]
Table 3. Mode of retrieval with site of device embolization
| Site of Embolization
Total N= 73 |
Need for surgery
N=26* |
Percutaneous snaring
N=75* |
p-value |
| LEFT ATRIUM 17 |
1 |
16 |
|
| Intraoperative cases 9 |
1 |
8 |
|
| Post-operative cases 8 |
0 |
8 |
|
| LEFT VENTRICLE 20 |
8 |
12 |
|
| Left ventricular cavity 13 |
6 |
7 |
|
| Intraoperative cases 7 |
1 |
6 |
|
| Post-operative cases 6 |
4 |
2 |
|
| Left ventricular outflow tract (LVOT) 7 |
2 |
5 |
|
| Intraoperative cases 1 |
0 |
1 |
|
| Post-operative cases 6 |
2 |
4 |
|
| MITRAL VALVE APPARATUS 7 |
4 |
3 |
0.0074 |
| Intraoperative cases 3 |
2 |
1 |
|
| Post-operative cases 4 |
2 |
2 |
|
| AORTA 29 |
4 |
25 |
|
| Ascending aorta/Arch of aorta 6 |
1 |
5 |
|
| Intraoperative cases 2 |
0 |
2 |
|
| Post-operative cases 4 |
1 |
3 |
|
| Descending aorta/Abdominal Aorta 18 |
3 |
15 |
|
| Intraoperative cases 5 |
0 |
5 |
|
| Post-operative cases 13 |
3 |
10 |
|
| Aortic/Iliac bifurcation 5 |
0 |
5 |
|
| Intraoperative cases 3 |
0 |
3 |
|
| Post-operative cases 2 |
0 |
2 |
|
The numbers from different tables might not add since the data in different patients is missing
Embolization site, mode of retrieval and complications with each device type
The most common sites of DE (both intraoperative and postoperative) for the ACP was the LA (25%, n=15/59) and for the Watchman device was the descending aorta/abdominal aorta (38.7%, n=12/31). [Table 3]
The mode of retrieval was predominantly percutaneous snaring for each device type. Specifically, 78% (46/59) of ACP, 67.7% (21/31) of WM and 72.7% (8/11) of Amulet DE were successfully snared percutaneously. Only 2 cases described internal bleeding during percutaneous snaring and both of them involved WM devices which embolized intraoperatively. All other successful percutaneous retrievals were uneventful. The need for surgical intervention was most frequent with WM device (32.2%, n=10/31) followed by Amulet device (27.3%, n=3/11) and the ACP device (22%, n=13/59) [Table 3]. Patients who required surgical intervention had a higher incidence of prolonged hospitalization and mortality. Of 26 cases that required surgical retrieval, 38.4% (n=10/26) had major complications which included severe valvular damage (n=6) and death (n= 6).
Table 4. Comparison of different device types
| Variable |
ACP N=59 |
WM N=31 |
Amulet N=11 |
P-Value |
| Intraoperative embolizations |
29 (49.2%) |
8(25.8%) |
3 (27.3%) |
0.066 |
| Site of Embolization |
|
|
|
|
| Left atrium |
08 |
01 |
0 |
|
| Left ventricle |
06 |
01 |
0 |
|
| Descending aorta/Abdominal aorta |
02 |
3 |
0 |
|
| Arch of aorta/Ascending aorta |
02 |
0 |
0 |
|
| Aortic bifurcation/Iliac bifurcation |
02 |
0 |
1 |
|
| Mitral valve apparatus |
02 |
0 |
1 |
|
| Left ventricular outflow tract (LVOT) |
0 |
0 |
0 |
|
| Unknown |
07 |
03 |
1 |
|
| Postoperative embolization |
30 (50.8) |
23 (74.2%) |
8 (72.7%) |
|
| Site of Embolization |
|
|
|
|
| Left atrium |
7 |
1 |
0 |
|
| Left ventricular outflow tract (LVOT) |
4 |
1 |
1 |
|
| Ascending aorta/Arch of aorta |
1 |
1 |
1 |
|
| Descending aorta/Abdominal aorta |
3 |
9 |
0 |
|
| Aortic/Iliac bifurcation |
0 |
1 |
1 |
|
| Mitral valve apparatus |
3 |
0 |
1 |
|
| Left ventricular cavity |
5 |
0 |
1 |
|
| Unknown |
7 |
10 |
3 |
|
| Complications |
19 (32.2%) |
12 (38.7%) |
6 (54.5%) |
0.35 |
| Surgery |
13 |
10 |
3 |
|
| Valvular damage |
|
1 |
1 |
|
| Internal bleeding |
0 |
2 (while PC snaring) |
0 |
|
| Stroke/TIA |
2 |
0 |
0 |
|
| Myocardial infarction |
2 |
0 |
1 |
|
| Cardiogenic shock |
1 |
0 |
2 |
|
| Limb ischemia |
0 |
0 |
1 |
|
| Death |
7 |
1 |
0 |
|
| Retrieval process |
|
|
|
|
| Surgery |
13 (22%) |
10 (32.2%) |
3 (27.3%) |
0.568 |
| Percutaneous snaring |
46 (78%) |
21 (67.8%) |
8 (72.7%) |
0.568 |
| Compression factor (IQR) |
14.1% (11.3-24.5%) |
19% (14.1-19%) |
23% (19.8-30.9%) |
|
ACP=amplatzer cardiac plug; WM=watchman; PC=percutaneous snaring; IQR= interquartile range
Impact of LAA morphology on device embolizations
Conclusions regarding morphology and its impact, if any, on DE cannot be drawn as the morphology of the LAA was not reported in majority of the cases (68%, n=70/103). Among those reported, cauliflower morphology was reported in 14 cases followed by chicken wing in 9, cactus in 6 and windsock in 4.
Acute leak was reported in 8.7 % (n=9/103) of patients. Out of these 9 patients, 7 belonged to the ACP 3 and Amulet groups 4, one belonged to WM group and one belonged to LAmbre. Six out of these nine patients had postoperative (acute) DE and three had intraoperative DE.
Operator reported reasons for device embolization
Out of 21 device-LAA mismatches, device oversizing was reported in 4 patients, device undersizing was reported in 7 patients and in the remaining 10 patients, the mismatch was not specifically defined.
This is the largest reported series of DE with LAAO to date. The main findings of this systematic review are: 1) the incidence of DE is 2% in our series; 2) DE occurred more frequently in the postoperative period and was associated with higher risk of serious complications, need for surgical retrieval and mortality compared with intraoperative DE; 3) operator reported device/LAA size mismatch is the most commonly identified factor associated with DE.
Earlier studies have reported that DE are more commonly observed intra-procedurally 5. On the contrary, in our study we found that more DE occurred post-procedurally. More than 50% of cases were recognized within the first 24 hours and 35% cases after one week. Embolized devices were found within the LA if recognized early and in the LV, LVOT, or aorta if found late.
The rate of major complications (including death) was significantly higher in postoperative DE cases compared to intraoperative DE. The need for surgical intervention and the rate of mortality significantly increased with LAAO DE occurring later from the time of deployment. All the complicated embolizations (100%, n=12/12) diagnosed more than 1 week after the procedure required surgical intervention and 33% of these resulted in mortality. This may relate to the fact that over time, the embolized device migrates out of the LAA and LA towards the mitral valve apparatus and LVOT. Devices in the LV are more likely to be trapped by the valves (mitral or aortic), both before and during the process of retrieval, requiring open surgical removal in most of the cases. Also, delay in recognition of LAAO DE prevents any prompt action until patient’s condition deteriorates and this can lead to increases in morbidity and mortality. Embolized ACP devices tended to locate in the LA (both intra and postoperatively) and also were less likely to require surgical intervention. This could perhaps be related to the design and structure of the device preventing it from going through the MV. In our study, we found that DE to LV and mitral valve apparatus were more likely to get complicated in comparison to other sites of embolization and were also more likely to require surgical intervention compared to other sites.
Table 5. Clinical characteristics and outcomes of patients with complicated surgical interventions
| Clinical variables |
Device type/timing |
Outcome |
| Acute severe MR due to entrapment of the device in the anterior mitral apparatus and mitral chordae rupture, was noted with the presence of a flail anterior leaflet. Also, the device caused dynamic obstruction of the LVOT, all leading to cardiogenic shock. Emergent surgery was planned. |
ACP device, diagnosed after 30 days post procedure, CHADS2 score 8 HASBLED score 4 |
Death |
| Aortic cusps damage. Aortic valve replacement and pacemaker implantation |
WM, Intraprocedural |
Prolonged hospitalization |
| Acute heart failure secondary to mitral valvular damage |
ACP, Post-operative within 24 hours HASBLED score 3 |
Prolonged hospitalization (18 days) |
| Surgery with reconstruction of mitral valve |
ACP, Intraoperative , CHADS2score 4 HASBLED score 3 |
Prolonged hospitalization (13 days) |
| MR leading to hemodynamic instability |
Amulet, Intraoperative, CHADS2 score 6 HASBLED score 4 |
Prolonged hospitalization |
| Surgical intervention |
ACP, Post-operative |
Death |
| Surgical intervention |
ACP, Post-operative |
Death |
| Ruptured mitral chordae tendinae/severe MR |
WM, CHADS2 score 4 HASBLED score 4, Post-operative |
Death |
| Hybrid surgical trans apical retrieval of the device but developed MOF |
ACP |
Death |
| Device dislocated one day after intervention and was caught in the mitral valve; Patient was transferred to University hospital of Bonn, device was removed and patient successfully operated; However, died of bleeding complications 6 days after the operation |
ACP, Post-operative, CHADS2 score 3 HASBLED score 3 |
Death |
ACP=amplatzer cardiac plug; MR=mitral regurgitation; LVOT=left ventricular outflow tract; MOF=multiorgan failure
The goals of this study are to make operators aware of the timings, outcomes and complications involved with LAAODE. We highlighted the temporal and spatial association of LAAODE with clinical outcomes. An operator should maintain a high index of suspicion for LAAO DE for early recognition and mitigation of a complicated course. It is possible that a proportion of the post-operative DE occur within the first 24 hours but are only detected later during routine follow-up or when a patient becomes symptomatic. Routinely performing transthoracic echocardiography (TTE) within the first 24 hours (as early as 3-4 hours) following a procedure may help to identify and possibly minimize the complications of an acute DE. In our experience these devices are difficult to locate on Xray due to the lack of radiopaque materials in their construction. Future generation devices should include radiopaque materials to facilitate Xray localization. Due to the reported lag between time of actual embolization and time of diagnosis in some cases, consideration should be given to performing a TTE before the routine 1 month follow-up to identify any DE 6. Patient education regarding symptoms and signs of DE (unusual palpitations, congestive heart failure decompensation/shortness of breath, stroke/transient ischemic attack, limb ischemia) could also play an important role in early diagnosis. Early recognition is key in minimizing morbidity and mortality associated with DE.
Out study is limited by all the issues related to its retrospective observational nature. In addition, the rhythm at the time of embolization was not reported by the authors. Another limitation is residual confounding. Lastly, heterogeneities between operators, institutions and device specific variables could influence the LAAODE rates.
DE with percutaneous LAA occlusion is common with a reported incidence of 2% in our review. DE occurred more frequently in the postoperative period and was associated with higher risk of serious complications, need for surgical retrieval and mortality compared to intraoperative embolization.






