Is AF Ablation Cost Effective?
William Martin-Doyle, BA1, Matthew R. Reynolds, MD, MSc2,3
1University of Massachusetts Medical School, Worcester, MA.2Beth Israel Deaconess Medical Center.3Harvard Clinical Research Institute, Boston, MA.
The use of catheter ablation to treat AF is increasing rapidly, but there is presently an incomplete understanding of its cost-effectiveness. AF ablation procedures involve significant up-front expenditures, but multiple randomized trials have demonstrated that ablation is more effective than antiarrhythmic drugs at maintaining sinus rhythm in a second-line and possibly first-line rhythm control setting. Although truly long-term data are limited, ablation, as compared with antiarrrhythmic drugs, also appears associated with improved symptoms and quality of life and a reduction in downstream hospitalization and other health care resource utilization. Several groups have developed cost effectiveness models comparing AF ablation primarily to antiarrhythmic drugs and the model results suggest that ablation likely falls within the range generally accepted as cost-effective in developed nations. This paper will review available information on the cost-effectiveness of catheter ablation for the treatment of atrial fibrillation, and discuss continued areas of uncertainty where further research is required.
Correspondence to: Matthew R. Reynolds, MD, MSc, Beth Israel Deaconess Medical Center, 185 Pilgrim Road/Baker 4, Boston, MA 02215.
The direct costs of treating atrial fibrillation in the United States have been estimated at $6.7 billion,1 a figure which is likely to grow with the large expected increases in the prevalence of AF.2 As one component of AF treatment, the use of catheter ablation to treat atrial fibrillation is growing rapidly.3-4 However, catheter ablation to treat AF is a relatively young and evolving technology, first described in 1998,5 is associated with significant upfront costs, and carries a risk of procedural complications. As previous reviews on the cost-effectiveness of AF ablation have noted, healthcare decision makers currently have only limited information to guide them on whether the use of AF catheter ablation represents good value.6-8 Cost-effectiveness analysis attempts to assess this value by quantifying the incremental changes in both cost and effectiveness involved with use of a new technology compared to the current standard of care, with results commonly expressed in units of cost per quality-adjusted life year.9 This review aims to summarize the available information on the cost-effectiveness of catheter ablation for the treatment of atrial fibrillation, and to identify continued areas of uncertainty where further research is required.
Clinical Evidence in Support of AF Ablation
In clinical studies conducted to date, AF ablation has generally been found to result in higher success rates(as measured by freedom from AF) compared to AADs, with less frequent but potentially more serious adverse events, as described elsewhere.10-13 A 2009 meta-analysis of 63 clinical studies on AF ablation completed through 2007(10) reported ablation success rates of 57% (single-procedure, off AAD therapy), 71% (multiple procedure, off AAD), and 77% (multiple procedure, AAD or unknown AAD), with major complications occurring in 4.9% of patients. Reported success rates for the treatment of paroxysmal AF are generally higher than for persistent AF, and while overall success rates are relatively high, there has been wide variation in results from study to study.14
While these figures appear promising when compared to the lower success rates typically achieved with AADs, especially in patients who have already failed one or more AADs, the limitations of the current clinical evidence base are widely recognized. Few RCTs comparing AF ablation to AADs have been conducted, and studies to date have generally been relatively small and of short duration, with few studies reporting follow-up longer than 12 months. Perhaps most importantly, while freedom from AF is the most common endpoint used in trials to date, it remains to be determined by randomized controlled trials whether ablation reduces the risk of stroke or mortality, as suggested by one nonrandomized study.15 These uncertainties in the clinical evidence base naturally lead to uncertainties in health economic assessments, which have used varied assumptions about long term ablation efficacy and the benefits of sinus rhythm maintenance.
AF Ablation and Quality of Life
AF has significant negative effects on quality of life in the majority of patients.16-17 In both randomized and nonrandomized studies of ablation which have measured QOL as an outcome, AF ablation has resulted in large improvements in quality of life.17-20 In one randomized controlled trial comparing AF ablation to AADs as first line therapy for paroxysmal AF, ablation resulted in statistically significant differences versus AADs on five of eight subscales of the SF-36 after 6 months, with the largest differences observed in the physical functioning and role-physical subscales, and significant differences also noted on the general health, social functioning, and bodily pain subscales.19 However, these studies have generally been limited by short follow-up duration and high rates of crossover.
While there is abundant evidence about the negative impact of AF on QOL and increasing evidence supporting the positive QOL impact of ablation, until recently there had been no available data on how those QOL changes translate into health state utility values, a fact noted by the authors of the first AF ablation cost-effectiveness analyses.21-22 Health state utility values range from 0 to 1 and are required to calculate quality-adjusted life years (QALYs) associated with a given health state – QALYs are simply the product of utility scores and life expectancy, summed over time.23 To address this lack of data on health state utilities in AF, the authors of the most recent AF ablation cost-effectiveness analysis,24 calculated the utilities of AF patients at baseline, and after successful conversion to NSR via AAD or ablation using previously validated methods for deriving utility scores from SF-12 or SF-36 questionnaires.25,26 Based on analysis of several AF cohorts, the authors reported a mean baseline utility value of 0.725 for patients in AF, and a change in utility for successful sinus rhythm maintenance of +0.065.
AF Ablation Costs and Cost Effectiveness
AAD treatment cost and hospitalizations
Hospitalization accounts for roughly half the medical costs associated with AF.1,27-30 Compared with rate control, rhythm control using AADs is associated with higher costs, partially due to higher rates of hospital admissions required to adjust medications.31-32 One study explored this relationship between AAD use and hospitalization cost, and found that medical costs among AF patients pursuing a rhythm control strategy rose dramatically with increasing numbers of recurrences, primarily driven by hospitalization costs.27 A recent meta-analysis of RCTs comparing AF ablation to AADs found that ablation is associated with significantly lower rates of hospitalization for cardiovascular causes than AADs, with a rate ratio of 0.15.33 One potential economic rationale for the use of AF ablation as opposed to AAD therapy, therefore, is that despite higher initial costs of ablation, there may be lower long-term follow-up and hospitalization costs resulting from ablation’s higher efficacy in maintaining normal sinus rhythm. Better documentation of this idea is needed.
Six studies to date have evaluated the total costs associated with pursuing an AF ablation treatment strategy, as shown in Table 1. Weerasooriya et al.34 first described the cost of AF ablation in 118 consecutive patients treated at a single center in France. The authors estimated that over a five year period, the cumulative cost of the ablation strategy reached €6,730 (in 2001 euros), similar to the five-year cost of €7,194 incurred with an antiarrhythmic drug strategy. The majority of costs of the ablation strategy were incurred upfront with the ablation procedure, and annual treatment costs after that point were higher among AAD patients; the authors note that after five years the costs associated with a pharmacologic strategy were higher than with ablation, and that costs continued to diverge after that point.
Table 1. Cost Estimates for AF Ablation
| Reference |
Location, perspective |
Type of AF, patient characteristics |
Analysis type |
Currency, year |
Time horizon |
Dis-count rate |
Comparator Therapy |
Cumulative cost of ablation over time horizon |
Cumulative cost of comparator therapy over time horizon |
| Weerasoriya et al., 2003(34) |
France, healthcare system |
Paroxysmal, AAD failures |
Model based on resource data from retrospective ablation cohort |
EUR, 2001 |
5 years; 10 years |
5% |
AADs |
5 years: €6,730
10 years: €8,291
|
5 years: €7,194
10 years: €12,760
|
| Chan et al., 2006(21) |
U.S., societal |
All types AF, at
low and moderate risk of stroke,
55 y.o. & 65 y.o. cohorts
|
Model based on published literature and Medicare data |
USD, 2004 |
Patient lifetime |
3% |
Rate control (RC); Amiodarone |
Moderate stroke risk /
55 y.o.: $59,380
Moderate stroke risk /
65 y.o.: $52,369
Low stroke risk / 65 y.o.: $43,036
|
Moderate stroke risk / 55 y.o.: RC: $50,509; Amiod:
$55,795
Moderate stroke risk / 65 y.o.: RC: $39,391; Amiod:
$43,358
Low stroke risk / 65 y.o.: RC: $24,540; Amiod:
$38,425
|
| Khaykin et al., 2007(35) |
Canada, healthcare system |
Paroxysmal, average patient based on resource utilization patterns in Canada and France |
Model based on published literature, CARAF registry,
and Canadian price weights
|
CAD, 2005 |
5 years |
3% |
AADs, RC, AC (weighted average) |
Range of $16,278 to $21,294, with annual cost of $1,597 to $2,132. |
Range of $4,176 to $5,060 annually |
| Rodgers et al., 2008(22) / McKenna et al., 2009(36). |
U.K., healthcare system |
“Predominantly paroxysmal”, refractory to ≥1 AADs; base ase CHADS =1 |
Model based on published literature and ablation costs from 1 UK cardiologist |
GBP, 2006 |
Patient lifetime |
3.5% |
Amiodarone |
£26,027 |
£15,367 |
| Khaykin et al., 2009(37) |
Canada, healthcare system |
Paroxysmal, symptomatic, first-line |
Model based on resource data from RAAFT pilot tudy |
CAD, 2005 |
1 year; 2 years |
3% |
AADs |
1 year: $12,283 2 years: $15,303 |
1 year: $6,053 2 years: $14,392 |
| Reynolds et al., 2009(24) |
U.S., healthcare system |
Paroxysmal, re- fractory to ≥1 AADs, male, 60 y.o. without se- vere structural heart disease |
Model based on published iterature, FRACTAL registry, Medicare data, and ablation costs at authors’ institution |
USD |
5 years |
3% |
AADs |
$26,584 |
$19,898 |
AADs = antiarrhythmic drugs; AC = anticoagulation; AF = atrial fibrillation; Amiod = Amiodarone; CAD = Canadian dollars; CARAF = Canadian Registry of Atrial Fibrillation; EUR = Euros; FRACTAL = The Fibrillation Registry Assessing Costs, Therapies, Adverse events and Lifestyle; GBP = British Pound; NSR = normal sinus rhythm; RAAFT = Randomized Trial of RFA versus AAD as First-Line Treatment of Symptomatic Atrial Fibrillation; RC = rate control; USD = U.S. dollars
As part of a US cost-effectiveness model of AF ablation versus rate control or AADs, Chan et al.21 compared lifetime costs in hypothetical 55 year-old and 65-year old patient cohorts at moderate or low risk of stroke. Lifetime costs were calculated as somewhat higher for patients undergoing ablation, and ranged from $43,036 to $59,380 for ablation, compared to ranges of $24,540 to $50,509 for rate control, and $38,425 to $55,795 for amiodarone (all in 2004 US dollars). The authors estimated the initial cost of AF ablation as $16,500, and assumed lower costs thereafter for successfully treated ablation patients than for AAD-treated patients.
Khaykin and colleagues35 subsequently estimated the costs of AF catheter ablation in Canada compared to the cost of rate control or AAD treatment. This model also relied on published literature and data on AF healthcare utilization patterns in Canada and France, and estimated that over a five-year time horizon the costs of AF ablation would slightly exceed those of medical therapy, ranging from $16,278 to $21,294 with an annual cost of $1,597 to $2,132, compared to an annual cost of medical therapy ranged from $4,176 to $5,060 (in 2005 Canadian dollars). The paper concluded that costs of ablation and AAD therapy would be equal after 3.2 to 8.4 years of follow-up, or with 3% discounting applied, after 4.5 to 10.8 years of follow-up.
Rodgers et al.22 evaluated the cost-effectiveness of AF ablation from the U.K. healthcare system perspective, in an analysis initially released as part of a NICE health technology assessment, and subsequently published in a peer reviewed journal.36 Their cost assumptions for ablation and AADs included an ablation procedure cost of £9,810 and AAD costs of £186 in year 1, and then £32 per year thereafter (only generic amiodarone was modeled). Annual treatment costs were assumed to be equal for both the NSR and AF health states, at £646 per year – an assumption which does not factor in potentially higher long-term hospitalization costs associated with AAD adjustments. Based on these assumptions, for their base-case scenario the authors estimated lifetime costs of £26,027 for ablation and £15,367 for AAD treatment.
In 2009, Khaykin and colleagues37 published an economic analysis of the RAAFT pilot study in Canada, comparing the costs of AF ablation to antiarrhythmic drugs as first-line therapy for the treatment of symptomatic paroxysmal AF. Following the first year of follow-up, costs were $12,283 in the ablation arm and $6,053 in the AAD arm (in 2005 Canadian dollars), and there was a significant difference in the rate of hospitalizations for AF favoring the ablation arm (9% vs. 54%). At the end of the two-year treatment period, costs for patients in the antiarrhythmic arm approached those of patients in the ablation arm, at $14,392 for AADs versus $15,303 for ablation. However, during the second year of the trial AAD patients were allowed to receive ablations. Since during the second year 18 of 37 AAD patients underwent ablations, this two-year AAD cost figure more accurately represents the cost of a delayed ablation strategy rather than a pure AAD strategy.
Most recently, Reynolds et al.24 assessed the cost-effectiveness of AF ablation from the US healthcare system perspective, relying on data from the published literature and AF ablation costs and QOL outcomes at the authors’ own institution. Initial costs of ablation were estimated at $15,000, with annual follow-up costs of $1,300 in year 1 and $200 in later years if NSR was maintained. AAD-associated costs, based on resource utilization observed in the FRACTAL registry,27 were set at $4,000 per year for patients who were well on a first line drug and $3,500 per year for patients well on amiodarone. Addition or changes of an AAD in either the AAD or ablation arm were assumed to incur the cost of a telemetry admission at $5,000. Like the previous analyses, over a five-year time horizon, ablation was found to cost somewhat more than therapy with antiarrhythmic drugs ($26,584 versus $19,898, in US dollars), and the authors noted that the initial higher costs of ablation were partly offset by lower long-term costs compared to AAD treatment over time.
Cost-Effectiveness of AF Ablation
Three studies,21,22,24 have evaluated the cost-effectiveness of AF ablation, as described in Table 2. These studies evaluated cost-effectiveness using the commonly accepted metric of the incremental cost-effectiveness ratio (iCER),9 which is measured in units of cost per quality-adjusted life year (QALY). All three studies used a Markov decision analytic model approach, and model inputs relied mainly on published literature, supplemented by previously unpublished cost information and other assumptions when necessary. There are various important differences between the structures and assumptions of these models, including the target AF patient population considered, the choice of comparator treatment, the differential risk of stroke / mortality assumed between NSR and AF states, the differential health state utility assumed between NSR and AF states, and the time horizon. The general structure of the three models and description of evaluated target patient populations are shown in Table 2.
Table 2. AF Ablation Cost-Effectiveness Analyses: Model Structures
| Item |
Chan et al., 2006(21) |
Rodgers et al., 2008(22) / McKenna et al., 2009(36) |
Reynolds et al. |
| Type of AF considered |
All types AF |
“Predominantly paroxysmal”, refractory to ≥1 AADs |
Paroxysmal AF, refra |
| Patient characteristics |
Three cohorts considered: Age 55 / moderate stroke risk Age 65 / moderate stroke risk Age 65 / low stroke risk |
Average age: 52 80% male Base-case stroke risk: CHADS2 =1 |
Age: 60
Male
No severe structural heart disease |
| Location |
United States |
United Kingdom |
United States |
| Perspective |
Societal |
Healthcare system |
Healthcare system |
| Analysis type |
Markov model |
Markov model |
Markov model |
| Sources used for model inputs / assumptions |
Published literature and Medicare data |
Published literature and ablation costs from 1 UK cardiologist |
Published literature, FRACTAL registry, Medicare data, and ablation costs at authors’ institution |
| Time horizon
|
Patient lifetime |
5 years;
Patient lifetime |
5 years |
| Anticoagulation |
All groups on warfarin or aspirin depending on stroke risk; if NSR achieved, warfarin→ aspirin after 6 months NSR |
Anticoagulation equivalent between groups: 64% on warfarin, 27% aspirin, 9% no anticoagulation |
Anticoagulation equivalent between groups |
| Comparator therapy |
Rate control (RC)
or
AAD (amiodarone) |
AAD (amiodarone) |
AAD: Sotalol / flecainide first-line; amiodarone second-line; rate control / anticoagulation (RC/AC) for treatment failures |
| Treatment strategy if NSR not maintained (Markov process) |
Ablation: Average 1.3 ablations/patient in 1st 12 months. Patients in AF >12 months after ablation shifted to anticoagulation only.
RC / AAD: Patients in AF maintained on initial treatment strategy (RC / AAD). |
Average 1.3 ablations/patient in 1st 12 months. Patients in AF post-AAD or in AF >12 months after ablation shifted to anticoagulation only. |
Ablation: Ablation 1→AAD1→
Ablation 2→AAD2 →RC/AC
AAD: AAD1→AAD2→RC/AC |
The study by Chan et al. in 2006 was the first to evaluate the cost-effectiveness of AF ablation.21 This model evaluated the cost-effectiveness of AF ablation compared to both rate control and AAD (amiodarone) treatment over a lifetime time horizon in three patient cohorts: a 55 year-old AF patient cohort at moderate stroke risk, a 65 year-old cohort at moderate stroke risk, and a 65 year-old cohort at low stroke risk. The primary goal of this study was to determine what reduction in stroke risk would be necessary for AF ablation to be cost-effective compared with either rate control or antiarrhythmic drug strategies. Therefore, the authors considered a range of reductions in stroke and mortality following conversion to normal sinus rhythm, which was assumed to be achieved by a higher percentage of ablation patients than by patients following any other strategy. In contrast, due to a lack of available data on health state utilities in AF, the authors assumed utility changes near zero following successful conversion to NSR.
For the patient cohorts evaluated, the Chan model calculated an incremental cost-effectiveness ratio (iCER) of ablation versus rate control of $28,700/QALY for 55 year-old patients at moderate risk of stroke, $51,800/QALY for 65 year-old moderate stroke risk patients, and an unfavorable $98,900/QALY for 65 year-old low stroke risk patients, as shown in Table 3. These results were based on assumptions favoring the ablation arm in terms of stroke and mortality risk: that 78% of ablation patients would be in NSR at the end of the first year, compared to approximately 36% and 58% of rate control and amiodarone patients, that patients in NSR would have stroke risks ranging from 0.5%-0.9% (depending on baseline stroke risk and treatment with warfarin or aspirin) compared to 0.7%-2.3% for patients in AF, and that patients experiencing a stroke would face a mortality risk of 8.2%-17.9%. Since the rate control strategy dominated the AAD strategy in this cost-effectiveness analysis (i.e., was associated with greater effectiveness at less cost), a comparison between the AAD and the ablation strategy was not made.
Table 3. AF Ablation Cost-Effectiveness Analyses: Findings in QALYs, Costs, and Incremental Cost-Effectiveness Ratios
| Finding |
Chan et al., 2006(21) |
Rodgers et al., 2008(22) /
McKenna et al., 2009(36) |
Reynolds et al., 2009(24) |
|
55 y.o., mod stroke risk |
65 y.o., mod stroke risk |
65 y.o., low stroke risk |
5 year time horizon |
Patient lifetime time horizon |
Base case, 5 years |
| Quality adjusted life years (QALYs) |
|
|
|
|
|
|
| Ablation |
14.26 |
11.06 |
11.40 |
11.18 |
12.14 |
3.51 |
| Comparator |
AAD: 13.81
RC: 13.95 |
AAD: 10.75
RC: 10.81 |
AAD: 11.02
RC: 11.21 |
10.76 |
10.77 |
3.38 |
| Incremental QALYs |
vs. AAD: 0.45
vs. RC: 0.31 |
vs. AAD: 0.31
vs. RC: 0.25 |
vs. AAD: 0.38
vs. RC: 0.19 |
0.42 |
1.37 |
0.13 |
| Cumulative costs over time period |
|
|
|
|
|
|
| Ablation |
$59,380 |
$52,369 |
$43,036 |
£26,016 |
£26,027 |
$26,584 |
| Comparator |
AAD: $55,795
RC: $50,509 |
AAD: $43,358
RC: $39,391 |
AAD: $38,425
RC: $24,540 |
£15,352 |
£15,367 |
$19,898 |
| Incremental QALYs |
vs. AAD: not calculated
vs. RC: $8,871 |
vs. AAD: not calculated
vs. RC: $12,978 |
vs. AAD: not calculated
vs. RC: $18,496 |
£10,664 |
£10,660 |
$6,686 |
| Incremental cost-effectiveness ratio (iCER), base-case |
vs. AAD: not calculated
vs. RC: $28,700/QALY |
vs. AAD: not calculated
vs. RC: $51,800/QALY |
vs. AAD: not calculated
vs. RC: $98,900/QALY |
£25,510/QALY
(£20,831 to £27,745 for other CHADS2 scores) |
£7,780/QALY
(£7,763 to £7,910 for other CHADS2 scores) |
$51,431/QALY |
| Sensitivity analyses |
Assumptions with significant impact on iCER (values varied within plausible limits) |
Rate of stroke in AF (warfarin)
Discount rate
Reversion rate to AF post-ablation
Ablation cost
Utility of warfarin therapy
Rate of hemorrhage on warfarin
Efficacy of rate control |
Utility of NSR vs AF
Prognostic value NSR (stroke prevention)Time horizon Reversion rate to AF post-ablation |
Utility of NSR vs AF
Time horizon
Utility of rate control
Ablation cost |
| Probability that AF ablation is cost-effective at assumed willingness-to-pay |
$50,000/QALY: 82%
$100,000/QALY: 96% |
$50,000/QALY: 40%
$100,000/QALY: 78% |
N/A |
£20,000/QALY: 16.5%
£30,000/QALY: 68.6% |
£20,000/QALY: 98.1%
£30,000/QALY: 99.6% |
N/A |
Later authors took slightly different approaches to the structure of their cost-effectiveness analyses. Rodgers et al. evaluated the cost-effectiveness of AF ablation compared to AAD treatment with amiodarone, from the perspective of the UK healthcare system.22,36 The analysis modeled cost-effectiveness for a “predominantly paroxysmal” AF patient cohort with characteristics conforming to those reported in a case series of patients seen in UK clinical practice,38 including an average age of 52 and 80% male gender. Like the Chan et al. analysis,21 the UK group assumed some differential reductions in stroke and mortality following conversion to NSR, with the assumption that NSR is maintained more frequently in patients undergoing ablation, in 84% of ablation patients at one year, compared to 37% of amiodarone patients. However, Rodgers and colleagues also assumed that quality of life gains secondary to achieving NSR would translate into meaningful improvements in health state utility compared to patients in AF.
Unlike the Chan et al. analysis, Rodgers et al. did not include a rate control comparator arm in their analysis, and assumed that ablation patients had already failed at least one AAD, consistent with current recommendations that ablation be used as second-line treatment for rhythm control.39 The authors conducted their analysis over a range of patient cohorts with differential stroke risks based on CHADS2 score, taking a CHADS2 score of 1 as the base-case scenario. Over a 5-year time horizon, the authors derived an iCER for AF ablation compared to amiodarone of £25,510 per QALY for the base case scenario, ranging from £20,831 to £27,745 per QALY for patients with CHADS2 scores from 3 to 0. When extended to a lifetime time horizon, the calculated iCERs were significantly more favorable, at £7,780 per QALY for the base case, ranging from £7,763 to £7,910 per QALY.
Finally, Reynolds et al. evaluated the cost-effectiveness of AF ablation from the US healthcare system perspective, comparing ablation to antiarrhythmic drugs for the treatment of paroxysmal AF patients who had already failed one or more antiarrhythmic drugs.24 The target patient population selected for modeling was 60 year-old men without severe structural heart disease, to conform to the typical characteristics of ablation patients reported in the published literature. In contrast to the previous analyses, the authors assumed no difference in stroke risk or mortality between the NSR and AF health states. The authors instead chose to focus on differences in utility between NSR and AF health states to drive any calculated differences in incremental quality-adjusted life expectancy between ablation and AADs. Since data on health state utilities for AF patients were not previously available, the group calculated utility weights for the AF and NSR health states based on AF patient responses to SF-12 and SF-36 questionnaires, as described above, assigning utility values of 0.725 and 0.79 to the AF and NSR health states.
Also unlike previous authors, Reynolds and colleagues did not calculate cost-effectiveness beyond a five-year time horizon, given the lack of long-term clinical data on AF ablation, nor did they assume that AAD treatment and its associated costs would be continued in the AAD patient cohort following recurrence of AF, as assumed in a few prior analyses. The authors assumed 60% single procedure efficacy off drugs, a 25% redo ablation rate, and 90% efficacy after 2 procedures with or without adjunctive AAD treatment.10 The authors note that their assumptions were conservative given that individual series and RCTs have reported higher success rates with ablation of paroxysmal AF.
Using these conservative assumptions, the model resulted in an incremental cost-effectiveness ratio of $51,431 per QALY gained for AF ablation compared to antiarrhythmic drugs. It should be noted that this iCER is consistent with the findings of the previous two analyses, and that it approximately equals the threshold value of $50,000/QALY that is frequently cited as acceptable in the United States.40 The authors further noted that should future clinical data demonstrate either stroke or mortality reduction following AF ablation, or that the freedom from AF and improved QOL achieved with ablation are maintained for longer than 5 years, then the cost-effectiveness of AF ablation would be even more favorable.
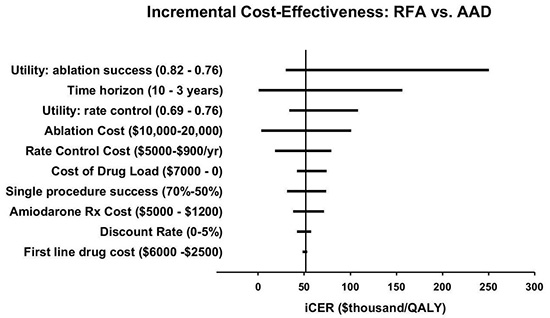
ses to identify model variables with significant impact on their overall findings. A “tornado diagram” from the Reynolds et al. 2009 study24 is reproduced in Figure 1, which displays the ranges in iCER that result when the value of key assumptions is varied within plausible limits of uncertainty. These one-way sensitivity analyses identified the utility of ablation success, the time horizon of the analysis, the utility of rate control, and the cost of ablation as the variables with the most impact on the incremental cost-effectiveness ratio. The Rodgers et al. and Chan et al. groups identified similar variables as the largest sources of uncertainty in their models Table 3. The UK group’s sensitivity analysis reinforces the Reynolds et al. finding that the differential utility of NSR vs. AF is a key variable influencing cost-effectiveness, and in addition they identified the prognostic benefits of NSR for stroke risk reduction and the long-term reduction of risk of recurrent AF following ablation as other key variables with significant effects on cost-effectiveness.
Figure 1. Incremental Cost-Effectiveness: AF ablation vs. AAD from Reynolds et al., 2009.(24) Reproduced with permission. Tornado diagram displaying the results of key 1-way sensitivity analyses on the iCER for ablation compared with AAD therapy. The base-case result is denoted by the vertical line, and the changes to the iCER by varying individual parameters within plausible limits (shown in parentheses) are shown in the horizontal bars
In addition to this type of one-way sensitivity analysis, the UK group also conducted a value-of-information (VOI) analysis,22 to quantify the expected value of perfect information regarding various assumptions used in their model. The VOI analysis assigns a monetary value to the maximum amount a decision maker should be willing to pay for perfect information about areas of uncertainty. This analysis found that further research to more precisely determine the magnitude and duration of health state utility changes in patients following ablation and AAD treatment would be of the greatest value.
Using Monte Carlo simulation, both the UK study and the Chan et al. study21 also evaluated the probability of cost-effectiveness at certain assumed values for willingness to pay. The Chan et al. study found that ablation was most likely to be cost-effective in younger AF patients at moderate stroke risk (55 year-old, moderate risk cohort), with an 82% probability of being cost-effective at a willingness to pay of $50,000/QALY, and a 96% probability at $100,000/QALY. Rodgers and colleagues found that the probability of being cost-effective was highly dependent on both time horizon and assumed willingness to pay. In the 5-year, base-case (CHADS2=1) analysis, the probability of cost-effectiveness for AF ablation at willingness to pay values of £20,000/QALY and £30,000/QALY only reached 16.5% and 68.6%. However, when the time horizon was extended to the patients’ lifetimes, the corresponding probabilities of being cost-effective reached 98.1% and 99.6% Table 3.
Studies evaluating the costs associated with catheter ablation have generally found that ablation is somewhat more costly than AAD treatment short-term, with estimates varying from country to country and depending on the time horizon and specific comparator drug. However, the higher rates of NSR achieved by ablation compared to AADs appear to offset these upfront costs by reducing the long-term costs of repeat hospitalizations and other care associated with AAD treatment. A recent meta-analysis of RCTs does suggest that ablation reduces the rate of hospitalizations compared with AADs,33 et al. but more research is needed in this area.
Three studies have evaluated the cost-effectiveness of AF ablation compared to rhythm control or antiarrhythmic drug strategies in selected AF populations. Results of these analyses indicate that compared to AAD therapy, ablation treatment results in improved quality adjusted life expectancy at somewhat higher cost, and that AF ablation is likely to be a cost-effective treatment option for appropriately selected patients. Notably, in all analyses conducted to date, incremental cost-effectiveness ratios for AF ablation in selected populations were close to the value of $50,000 per QALY that is typically considered acceptable in the United States, as well as to the £20,000-£30,000 per QALY cost-effectiveness threshold applied in the United Kingdom.41
The assumptions used to construct cost-effectiveness models have a noteworthy impact on determining which patients might be the most cost-effective candidates for ablation. If one assumes that the major health benefits for ablation over alternative treatments are reductions in stroke and mortality risk, as in the Chan et al. model, then ablation will appear most cost-effective in patients with at least a moderately elevated risk of stroke. If, however, QALY gains following ablation are driven primarily by improvements in symptoms and quality of life associated solely with maintenance of sinus rhythm, then the optimal ablation candidate from a cost-effectiveness standpoint is somewhat different. Under this set of assumptions, cost-effectiveness is most likely in patients with lower baseline quality of life scores (i.e. patients highly symptomatic from their AF) who lack major comorbid conditions, since impaired quality of life due to other health problems might be less likely to respond to ablation.
Limitations of Current Studies
Current cost-effectiveness analyses rely heavily on data from completed randomized trials of AF ablation. This restricts the AF population in which cost-effectiveness can be reasonably estimated to the primary subjects of AF ablation trials to date: relatively young, symptomatic paroxysmal AF patients treated second line, following AAD failure. In addition, many key assumptions in these cost-effectiveness models are based on sparse evidence, resulting in significant uncertainty about the true value of these parameters and therefore the cost-effectiveness of AF ablation. Perhaps most importantly, it is not yet known whether AF ablation will reduce the risk of stroke and mortality when compared to alternative therapies. Another key uncertainty is whether freedom from AF and improved quality of life are maintained long-term after initially successful ablations; there is little systematic long-term evidence of cure in ablated patients. In addition to the lack of long-term efficacy data, there have been no large long-term cost collection studies in these patients. Analyses suggesting that ablation is cost equivalent to medical therapy are therefore contingent on the uncertain assumption that ablation efficacy is maintained long term. In addition, since data on the safety and efficacy of AF ablation have primarily been generated at leading treatment centers, it is also unclear whether the clinical results of AF ablation in real-world clinical practice (where operator experience and procedure volume may be lower) are as favorable as were modeled in these cost-effectiveness studies. These limitations all introduce significant uncertainty into the evaluation of the cost-effectiveness of AF ablation.
Future directions in AF ablation Cost Effectiveness Analysis
Data on the efficacy of AF ablation in reducing stroke and mortality and improving quality of life over the long term is needed. The Catheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation Trial (CABANA),42 a randomized controlled trial comparing AF ablation to rate control or AAD medication, began enrolling patients in August 2009. CABANA has been designed with a planned enrollment of 3,000 AF patients who will be followed for a minimum of two years, and the trial will prospectively gather data on mortality, stroke, and other clinical outcomes in a broad AF patient population, addressing many of the limitations of the current clinical evidence base. CABANA will also collect data on health economic and QOL outcomes. Completion of CABANA is expected in 2015. In addition to CABANA, other recently completed and ongoing clinical trials43-50 studying AF ablation in a range of settings can be expected to inform future cost-effectiveness analyses of AF ablation in additional patient groups. Going forward, these trials should help address the questions of whether AF ablation is both clinically appropriate and cost-effective, not only in currently recommended AF populations, but also when used in other settings, including as first-line therapy, in persistent AF, and in patients with comorbidities such as congestive heart failure.
Until such data is available, cost-effectiveness models extrapolating from the currently available clinical data suggest that AF ablation is a cost-effective treatment option for those selected AF patients for whom ablation is endorsed by current consensus guidelines.14,39






