Atrial Fibrillation in the Wolff-Parkinson-White Syndrome
Osmar Antonio Centurion MD, PhD, FACC
Division of Electrophysiology and Arrhythmias, Cardiovascular Institute, Sanatorio Migone-Battilana.
Asuncion, Paraguay, Departamento de Cardiologia, Primera Catedra de Clínica Médica, Universidad Nacional de Asuncion..
Since the advent of catheter ablation for atrial fibrillation (AF) aiming the pulmonary veins a few years ago, there has been an overwhelming interest and a dramatic increase in AF investigation. AF has a different dimension in the context of the Wolff-Parkinson-White (WPW) syndrome. Indeed, AF may be a nightmare in a young person that has an accessory pathway (AP) with fast anterograde conduction. It may be life-threatening if an extremely rapid ventricular response develops degenerating into ventricular fibrillation. Therefore, it is very important to know the mechanisms involved in the development of AF in the WPW syndrome. There are several possible mechanisms that may be involved in the development of AF in the WPW syndrome, namely, spontaneous degeneration of atrioventricular reciprocating tachycardia into AF, the electrophysiological properties of the AP, the effects of AP on atrial architecture, and intrinsic atrial muscle vulnerability. Focal activity, multiple reentrant wavelets, and macroreentry have all been implicated in AF, perhaps under the further influence of the autonomic nervous system. AF can also be initiated by ectopic beats originating from the pulmonary veins, and elsewhere. Several studies demonstrated a decrease incidence of AF after successful elimination of the AP, suggesting that the AP itself may play an important role in the initiation of AF. However, since AF still occurs in some patients with the WPW syndrome even after successful ablation of the AP, there should be other mechanisms responsible for the development of AF in the WPW syndrome. There is a clear evidence of an underlying atrial muscle disease in patients with the WPW syndrome. Atrial myocardial vulnerability has been studied performing an atrial endocardial catheter mapping during sinus rhythm, and analizing the recorded abnormal atrial electrograms. This review analizes the available data on this singular setting since AF has a reserved prognostic significance in patients with the WPW syndrome, and has an unusually high incidence in the absence of any clinical evidence of organic heart disease.
Correspondence to: Prof. Dr. Osmar A. Centurión, MD, PhD, FACC, Associate Professor of Medicine, Faculty of Medical Sciences, Chief, Department of Cardiology, Hospital de Clinicas, Asunción National University, Trejo y Sanabria 1657, Sajonia
Asunción, Paraguay.
Atrial fibrillation (AF) is a common arrhythmia with multiple possible complications that reaches a different dimension in the context of the Wolff-Parkinson-White (WPW) syndrome.1-4 Since the advent of catheter ablation for AF aiming the pulmonary veins a few years ago, there has been an overwhelming interest and a dramatic increase in AF investigation.5-7 Although, for most WPW patients the AP ablation is a curative solution, sustained episodes of AF still occur in certain patients despite the disappearance of the AP.8 Sharma et al by surgical means, and Haissaguerre et al12 by catheter ablation, have documented a reduction in AF inducibility following elimination of the AP in patients with WPW syndrome. Indeed, ablation of the AP is very effective in the abolition of conduction through the AP, and of clinical episodes of atrioventricular reciprocating tachycardia (AVRT) and AF; however, it does not prevent recurrences of AF in certain patients. Therefore, it is very important to determine all possible mechanisms for the development of AF in the WPW syndrome. It is paramount to understand that AF may be life-threatening in the setting of WPW syndrome with fast anterograde AP conduction, because a rapid ventricular response may develop degenerating into ventricular fibrillation.13 Several mechanisms responsible for the development of AF in the WPW syndrome were investigated in detail, namely, the spontaneous degeneration of AVRT into AF, the electrical properties of the AP, the effects of AP on atrial architecture, and the intrinsic atrial muscle vulnerability.14-22 Considering all the mechanisms proposed to explain the development of atrial fibrillation in the WPW syndrome, this review analizes the available data on this singular and interesting topic since AF has a reserved prognostic significance in patients with the WPW syndrome, and has an unusually high incidence in the absence of any clinical evidence of organic heart disease.
Figure 1 Atrial fibrillation in the Wolff-Parkinson-White syndrome
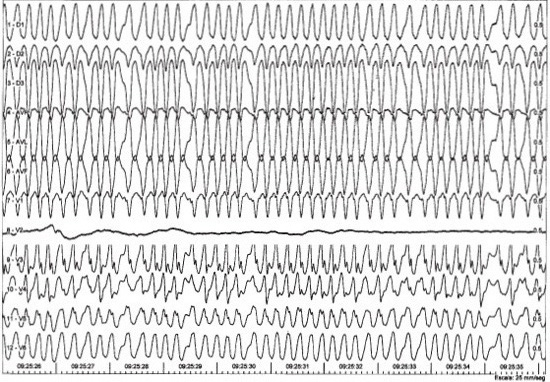
12 lead electrocardiographic recording in a patient with induced atrial fibrillation in the manifest Wolff-Parkinson-White syndrome. There is an evident very rapid ventricular rate. Reprinted with permission from Avalos Morel P, Centurión OA, Bianco Cáceres HF et al. Rev Soc Parag Cardiol 2005;2:159-168.
Electrophysiological properties of the accessory pathway in the WPW syndrome
Anterograde and retrograde electrophysiologic properties of the AP have been well investigated. The coexistence of a functional retrograde AP and sustained episodes of AVRT has been found to play an important role in triggering AF in patients with the WPW syndrome.13,23 In the electrophysiologic laboratory, it is relatively common to observe spontaneous degeneration of induced AVRT into AF in WPW patients. AF has a different dimension in the context of the WPW syndrome (Figure 1). It may be a nightmare in a young person that has an AP with fast anterograde conduction. AF may be life-threatening if an extremely rapid ventricular response develops degenerating into ventricular fibrillation. There is clear data to support that retrograde conduction to the atrium through multiple AP, or multifiber AP during AVRT can initiate AF. The incidence of spontaneous degeneration of induced AVRT into AF has been reported to be in the range of 16% to 26%,13 and it was found to occur in a similar proportion in patients with concealed WPW, and manifest WPW syndrome.24 Frequent tachycardias seem to promote an electrical remodeling and an increased atrial vulnerability to AF. For example, AVRT can increase atrial vulnerability as a result of a shortened atrial cycle length, increased sympathetic tone and atrial stretch due to hemodynamic changes that occur during AVRT. In this regard, Chen et al25 observed that the cycle lenght of reciprocating tachycardia at the time of electrophysiologic study was significantly shorter in WPW patients with than without AF. This finding suggests that it is easier to develop AF in a rapid episode of sustained AVRT.
Successful surgical or transcatheter ablation of the AP in patients without organic heart disease has been demonstrated to prevent future occurrence of AF in the majority of patients.11,13 This fact is well documented by long-term follow-up studies after successful AP ablation that demonstrated significantly reduced incidences of spontaneous AF. The recurrence rate of spontaneous AF after successful ablation of the AP is reported to be in the range of 6% to 10%.11,13 However, Hamada et al. made a very interesting observation in this respect. They observed that clinical episodes of AF recurred in 71% of their patients whose AF remained inducible immediately postablation, however, in none of the patients who remained uninducible postablation.26 Threrefore, there is a high incidence of AF recurrence in a subgroup of patients whose AF remained inducible despite successful ablation of the AP. A detailed examination of this subgroup of patients prone to develop AF could shed more light in the understanding of the mechanisms for the genesis of AF in WPW patients despite successful AP ablation.
Atrial double potentials and retrograde AP conduction.
NHsieh et al11,17 investigated the influence of atrial double potentials in the genesis of AF in patients with WPW syndrome. Double atrial potentials recorded in the coronary sinus are not an unusual phenomenon in patients with supraventricular tachyarrhythmias, and they have shown to potentiate the occurrence of atrial tachycardias. They demonstrated that patients with the WPW syndrome, especially with a left lateral bypass tract, had a higher incidence of double atrial potentials and induced AF than patients with AVNRT. Furthermore, WPW patients with double atrial potentials had a higher incidence of induced AF than those WPW patients without double atrial potentials. Campbell et al11,23 demonstrated a high incidence rate of AF that was initiated with incremental right ventricular pacing and premature ventricular contraction (PVC). They described in detail the role of retrograde multiple AP as a mechanism of premature atrial contraction that initiates atrial repetitive fir Hsieh et al11,17 investigated the influence of atrial double potentials in the genesis of AF in patients with WPW syndrome. Double atrial potentials recorded in the coronary sinus are not an unusual phenomenon in patients with supraventricular tachyarrhythmias, and they have shown to potentiate the occurrence of atrial tachycardias. They demonstrated that patients with the WPW syndrome, especially with a left lateral bypass tract, had a higher incidence of double atrial potentials and induced AF than patients with AVNRT. Furthermore, WPW patients with double atrial potentials had a higher incidence of induced AF than those WPW patients without double atrial potentials. Campbell et al23 demonstrated a high incidence rate of AF that was initiated with incremental right ventricular pacing and premature ventricular contraction (PVC). They described in detail the role of retrograde multiple AP as a mechanism of premature atrial contraction that initiates atrial repetitive firing or intratrial reentry in the vulnerable period of the atrium during AVRT.23 They stated that intermittent retrograde conduction over a second AP with faster conduction caused early atrial depolarization in a critical and vulnerable period of the atrium, setting the scenario for reentry to occur.
Spontaneous occurrence of PVC depolarizes the atrium in a retrograde manner that can cause AF to develop. Iesaka et al27 hypothesized that during AVRT, the complex excitation inputs into the atrium over the retrograde multiple or multifiber AP could trigger AF. They identified retrograde multiple and multifiber AP based on the results of electrophysiologic studies and radiofrequency catheter ablation. The incidence of clinical PAF, as well as, induced AF was significantly greater in the multiple AP patients. However, the incidence of clinical AVRT was similar between multiple and single AP patients. The incidence of AF initiated during ventricular pacing and AVRT was significantly greater in the multiple AP patients. A very interesting finding in this study27 was that AF inducibility during AVRT and ventricular pacing was eliminated by partial ablation of multiple or multifiber AP. However, AVRT inducibility remained in most patients with partial ablation of the multiple o multifiber AP. The incidence of induced AF after total ablation was similar between patients with multiple or single AP. The authors based on their findings indicate that the existence of a retrograde multiple or multifiber AP is strongly related to AF inducibility. In addition, the complex excitation inputs into the atrium over the retrograde multiple or multifiber AP is necessary to trigger AF. Retrograde conduction of PVC to the atrium in the WPW syndrome caused multiple episodes of PAF in a patient without previous arrhythmias after having a myocardial infarction.15 During the electrophysiological study the patient presented two spontaneous episodes of AF initiated by PVC conducted to the atria through the AP. After successful catheter ablation of the AP the patient did not present arrhythmia recurrences, although he had multiple PVCs recorded in a 24 Hs Holter monitoring.15 It may be argued that atrial vulnerability could be a predisposing factor in this kind of patients with a previous myocardial infarction. The impairment of the diastolic left ventricular function could modify the electrophysiological properties of the atria because of an increase in atrial pressure and atrial stretch. However, the fact that the patient did not have AF episodes after catheter ablation of the AP is against this mechanism being the only element responsible for the arrhythmia episodes. This interesting single case clearly demonstrates how complex is the mechanism to develop AF in the WPW syndrome. The authors15 hypothesize that PVCs with a short coupling interval resulted in VA conduction to the atria and activated the left atrium during the atrial vulnerable phase, thereby precipitating the onset of AF. This hypothesis is supported by two facts: first, AF episodes were experienced only after myocardial infarction in the presence of an AP. This could be related to a possible increase in the appearance of PVCs with different origins and coupling intervals. Second, new AF episodes were not experienced after successful AP ablation despite the fact that Holter monitoring performed after ablation demonstrated the presence of frequent polymorphic PVCs. In this regard, Jackman et al. observed multiple retrograde conductions over separate AP branches during AVRT and reentry originating from the branching networks. They indicated that microreentry mimicking atrial flutter or fibrillation could originate within the branching networks of the AP strands and that this may account for the unusually high incidence of AF in the WPW syndrome.28 In their study, they utilized closely spaced orthogonal catheter electrodes in the coronary sinus and found electrophysiologic evidence for a branching or multifiber structure of the left free wall AP. However, this finding has not been comfirmed in a large population. Moreover, this finding was indirectly contradicted by other mapping studies of AF initiation in patients with the WPW syndrome.13,29,30 These two studies demonstrated that the onset of AF was more frequently initiated near the high right atrium regardless of the AP location.13,29,30 Fujimura et al13 showed that most episodes of AF started at a high right atrial site regardless of AP location, with only 19% of AF episodes starting at the electrode site in the coronary sinus closest to the AP
Intraatrial wavefront collision and anterograde AP conduction
There are several studies that stressed the relation between anterograde conduction properties of the AP and AF in the WPW syndrome.13,24,30,32 Ong et al. performed an atrial mapping study using a multiple electrode array during surgery and suggested a possible mechanism of sustaining atrial fibrillation in patients with WPW syndrome.30 They demonstrated that wavefront collisions between incoming atrial wavefronts via an AP during non-preexcited beats generated new wavefronts to help perpetuate AF. This concept of intraatrial wavefront collision possibly explains susceptibility to AF in patients with multiple AP. Multiple and asynchronous wavefronts could be generated by conduction over multiple AP or widely separated strands forming multifiber AP during AVRT. The wavefronts collision in the atrium could be a mechanism for induction and perpetuation of AF. Although, it seems a plausible conception the exact electrophysiologic mechanism remains to be clarified in detail.
Fujimura et al13 observed that the anterograde AP effective refractory period (ERP) was shorter in the group with AF than in the control group, and that there were no significant differences in retrograde properties. Della Bella et al24also reported similar findings. They found that the anterograde ERP of the AP was significantly shorter in WPW patients with spontaneous AF that in those WPW patients without spontaneous AF. They also found that AF was more frequent in patients with manifest WPW than in those with concealed WPW syndrome. These findings suggest that the retrograde conduction properties of a single AP are not the critical determinants of AF. The study by Asano et al31 is in accord with this concept. Although they studied symptomatic and asymptomatic patients, they found that the incidence of spontaneous AF in the manifest WPW group was higher than in the concealed WPW group. However, this was not the same for the induction of AVRT in these two groups. The induction of AVRT was 75% in the manifest WPW group compared to 100% in the concealed WPW group. The mean AVRT cycle length was shorter in patients with concealed WPW than in the manifest WPW patients. This fact does not explain the lower incidence of AF in the concealed WPW group, since shortening of Fujimura et al13 observed that the anterograde AP effective refractory period (ERP) was shorter in the group with AF than in the control group, and that there were no significant differences in retrograde properties. Della Bella et al24also reported similar findings. They found that the anterograde ERP of the AP was significantly shorter in WPW patients with spontaneous AF that in those WPW patients without spontaneous AF. They also found that AF was more frequent in patients with manifest WPW than in those with concealed WPW syndrome. These findings suggest that the retrograde conduction properties of a single AP are not the critical determinants of AF. The study by Asano et al31 is in accord with this concept. Although they studied symptomatic and asymptomatic patients, they found that the incidence of spontaneous AF in the manifest WPW group was higher than in the concealed WPW group. However, this was not the same for the induction of AVRT in these two groups. The induction of AVRT was 75% in the manifest WPW group compared to 100% in the concealed WPW group. The mean AVRT cycle length was shorter in patients with concealed WPW than in the manifest WPW patients. This fact does not explain the lower incidence of AF in the concealed WPW group, since shortening of the cycle length is known to increase atrial vulnerability. Therefore, the genesis of AF in the WPW syndrome can not be solely attributed to the ocurrence of AVRT. Intra-atrial or inter-atrial conduction disturbances may be a possible explanation for the longer cycle length of AVRT in patients with manifest WPW syndrome. The anterograde AP conduction properties distinguished patients with and without AF. It is known that a shorter anterograde AP ERP allows faster ventricular rates during AF, therefore, the associated atrial stretch and hypoxia may contribute to sustaining the arrhythmia.
Atrial structural heterogeneities at the AP insertion. There is no detailed data on the structure of atrial tissue around the AP available currently. Most of the histopathological studies in patients with WPW syndrome have delt with the AP itself with no special description of the atrial tissue at the insertion of the AP. It is well known that structural heterogeneities play an important role in atrial reentry due to the influence of unidirectional block and conduction delay. Thus, it is possible that in patients with WPW syndrome, the increased structural heterogeneity created by the presence of the AP may play a role in the generation and maintenance of atrial reentry.32 In experimental studies of the canine heart model of WPW syndrome, structural differences in the AP apparently affected refractoriness and conduction properties of the AP.33 It was postulated that the AP is the result of an embriologic fault in the formation of fibrous tissue separating the atria and the ventricles.34 Therefore, developmental abnormalities may also be present in the atrial tissue adjacent to the AP, which may affect the functional electrical properties of the atrium close to the AP insertion. Dispersion of the refractory periods and conduction disturbances apparently occur around the interconnection between different tissues such as the atrium and the AP. Either anatomical or functional properties of the atrial tissue near the AP may play a role in the genesis of AF and may contribute to the different incidence of atrial vulnerability and AF in the WPW syndrome.
The anatomy, direction and location of the AP may play a role in the genesis of AF in the WPW syndrome. The AP may run in an oblique course rather than perpendicular to the transverse plane of the atrioventricular groove. As a result, the fibers may have an atrial insertion point that is transversely several centimeters removed from the point of ventricular attachment. The AP may occasionally exist as broad bands of tissue rather than discrete hair-like structures. Other than the anatomy of the AP, the location of the AP is better related to induction of AF. Several studies found different induction rates of AF depending on the exact location of the AP23-26 It was shown that patients with an anteroseptal AP had a high rate of inducible arrhythmia (62%). Patients with a right free wall AP had a rather low rate of inducible arrhythmia (21%). Patients with left free wall and posteroseptal AP had a 44% and 36% rate of induction, respectively.23-26 Patients with a right-sided AP had a lower inducibility of AVRT and a relatively long retrograde ERP over the AP. This allowed only relatively late PVCs to be conducted retrogradely over the AP to the atrium, wich might explain the lower rate of inducibility of AF in these patients.
Figure 2 Atrial endocardial mapping sites
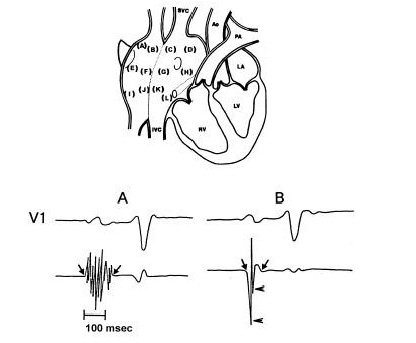
The upper part of the figure shows 12 endocardial mapping sites in the right atrium. The atrial endocardial electrograms were recorded in each patient from the anterior, lateral, posterior and medial aspects of the high right atrium (a,b,c,d), mid right atrium (e,f,g,h) and low right atrium (i,j,k,l). SVC= superior vena cava; IVC= inferior vena cava; Ao= aorta; PA= pulmonary artery; LA= left atrium; RV= right ventricle; LV= left ventricle.
Intrinsic atrial muscle vulnerability in the WPW syndrome
The persistance of AF in certain patients with WPW syndrome despite the successful abolition of the AP may be explained by the presence of an underlying atrial disease considering the AP as an innocent bystander.13,28 Patients with the WPW syndrome associated with AF were found to have a high incidence of electrophysiological abnormalities of the atrial muscle. This intrinsic atrial muscle vulnerability certainly plays an important role in the occurrence of AF in these patients. AF has a particular prognostic significance in patients with the WPW syndrome, and its incidence is unusually high in the absence of any clinical evidence of organic heart disease. Ablation of the AP is very effective in the abolition of conduction through the AP, and it has been shown that recurrences of AF after succesful AP ablation occur at a low incidence. Haissaguerre et al12 have documented a reduction in AF inducibility following catheter ablation in patients with WPW syndrome. Sharma et al11 found a reduction in AF inducibility following elimination of AP by surgical ablation. Other studies have also demonstrated a reduction in AF inducibility after successful AP ablation.11-13 Indeed, ablation of the AP is very effective in the elimination of clinical episodes of AVRT and AF; however, it does not prevent recurrences of AF in certain patients. Therefore, it is very important to determine all possible mechanisms for the development of AF in the WPW syndrome patients. An explanation suggested, in certain patients, is the presence of an underlying intrinsic atrial disease.13,28 In the absence of structural atrial disease, clinical electrophysiologic studies have not clearly defined atrial features that can predict spontaneous occurrence of AF. Some investigators have studied the atrial vulnerability showing that the induction of sustained episodes of AF was more frequent in patients with a history of spontaneous AF. Others have analyzed the atrial electrophysiological substrate that may predispose to AF. They evaluated atrial refractoriness, intra-atrial and interatrial conduction times, and several electrophysiological parameters elicited with programmed atrial stimulation with single extrastimulus. Important information about intrinsic atrial muscle vulnerability was obtained by atrial endocardial electrograms morphology recorded by atrial endocardial catheter mapping during sinus rhythm (Figure 2).
Atrial refractorines dispersion. Nonhomogeneity of ERP of contiguous cells causes a slower conduction velocity of the stimulus that propagates through partially repolarized cells, allowing the genesis of unidirectional blocks and the appearance of multiple reentries.35 In experimental studies with a computer model of AF, Moe et al35 demonstrated that an atrial condition characterized by short and nonhomogeneous atrial ERP, associated to intra-atrial conduction disturbances, is considered an important factor in the appearance and maintenance of AF. These findings were later corroborated by other investigators.36 In a landmark paper from Allesie’s laboratory, Konings KT et al37 described various types of AF in humans with the WPW syndrome. They induced AF by rapid atrial pacing in 25 patients with WPW syndrome undergoing surgery for interruption of their AP. The free wall of the right atrium was mapped using a spoon-shaped electrode containing 244 unipolar electrodes. Based on the complexity of atrial activation, they defined three types of AF. In type I (40%), single broad wave fronts propagated uniformly across the RA. Type II (32%) was characterized by one or two nonuniformly conducting wavelets, whereas in type III (28%), activation of the RA was highly fragmented and showed three or more different wavelets that frequently changed their direction of propagation as a result of numerous arcs of functional conduction block. They found significant differences among the three types of AF in median intervals, variation in AF intervals, incidence of electrical inactivity, and reentry, and average conduction velocity during AF. Therefore, they could demonstrate that from type I to type III, the frequency and irregularity of AF increased, and the incidence of continuous electrical activity and reentry became higher. These various types of AF in humans appear to be characterized by different numbers and dimensions of the intra-atrial reentrant circuits. Clinical electrophysiology has identified several atrial features that may lead to the appearance and maintainance of AF, sometimes with conflicting results. These different results may be due to multiple factors, including different stimulation protocols and nonhomogeneous groups of patients. Some investigators reported short atrial ERP in patients with PAF,38 while others did not.39 Thus, it is controversial to utilize atrial ERP as a useful measure of atrial vulnerability. Several studies have shown conflicting results regarding refractoriness in AF. The measurement of atrial ERP in AF patients in only one site does not necessarily represent atrial refractoriness since these patients have a wide dispersion of atrial refractoriness. Therefore, it is not comparable in different sites of the atrium neither in different patients. It has been shown that the atrial ERP physiologically shortens with increasing heart rate.40 This rate adaptation is less evident in AF patients, as well as, in isolated cellular preparations. Riccardi et al41 evaluated the rate adaptation of ERP in WPW patients with and without AF, analyzing the gradient between two different atrial pacing cycle lengths. They found that the functional refractory period increased in most AF patients (81%) with an increase of the atrial stimulation rate, while this absent rate adaptation was observed only in few patients (24%) without AF. The functional refractory period expresses the time needed for the electrical stimulus to be conducted from the distal pair of electrodes to the proximal pair of electrodes, so it is a local intraatrial conduction parameter in a relative refractory condition. The fact that WPW patients with AF showed higher values of refractory periods which became even higher with increasing heart rate,41 suggests the concept of AF as based on slow con conduction through partially recovered myocardium.
The ablation technique utilized for the AP ablation may produce different results regarding atrial vulnerability and AF induction. Muraoka et al 42observed that the atrial ERP was prolonged, the zones of atrial vulnerability were narrowed and the induction rate of AF was reduced following elimination of the AP by surgical cryoablation. However, these parameters were unchanged in patients that had their AP ablated by radiofrequency catheter ablation. Although, they could not clearly explain these different findings with the different ablation techniques, they argued that the prolongation of the atrial ERP played a key factor in the decrease of the AF induction rate in those patients ablated by surgical cryoablation. Probably, the larger myocardial injury created by surgical cryoablation, or dissection of the atrioventricular sulcus may be related to the lower incidence of AF. Another factor that might have influenced is that the radiofrequency applications were mainly delivered on the ventricular side of the atrioventricular valve annulus, while surgical cryoablations were performed directly on the atrial tissue. Therefore, the injury of the atrial tissue was greater in this latter group of patients. The resulting prolongation of the atrial ERP may prevent capture of short coupled premature atrial excitation and, therefore, may result in prevention of atrial electrical disorganization and AF. Tsuji et al38 also showed that the occurrence of AF depends on a short atrial ERP, and AF mainly originated in the high right atrium regardless of the AP location.
Atrial response to programmed stimulation. The induction of AF during electrophysiological testing makes its evaluation difficult and may lead to the undiserable need for antiarrhythmic agents or electrical cardioversion. On the other hand, the induction of AF with programmed atrial stimulation with single extrastimulus is not always successful even in patients with clinically documented AF. Besides the use of rapid burst pacing of the atrium may induce nonspecific AF. Therefore, the analysis of other atrial electrophysiological parameters is useful as indicators of potential atrial vulnerability. There are several atrial electrophysiological parameters relating to AF which are elicited with atrial programmed stimulation. The inducibility of AF, fragmented atrial activity, repetitive atrial firing, and intraatrial conduc tion delay has been previously examined. With atrial programmed stimulation, transient AF was induced in 83% of the WPW patients with a history of clinically documented paroxysmal AF.14
Although, for most WPW patients the AP ablation is a curative solution for the AVRT, sustained episodes of AF still occur in certain patients despite the disappearance of the AP. In order to clearly assess the intrinsic atrial vulnerability in WPW patients is necessary to perform a complete electrophysiologic study before and after AP ablation. Hamada et al26 studied the existing electrophysiologic differences between WPW patients whose AF remained inducible, and those with AF that could not be induced following AP ablation. They demonstrated that WPW patients with AF had significantly longer maximal atrial conduction delay and wider conduction delay zone than controls. Considering only the patients with WPW syndrome and AF, ablation of the AP did not change the maximal atrial conduction delay and conduction delay zone in those patients whose AF remained inducible. However, AP ablation normalized the maximal atrial conduction delay and conduction delay zone in those patients whose AF remained noninducible. There was no significant difference in these parameters compared to controls. Therefore, they suggest that there is definitive electrophysiologic evidence of two different mechanisms for AF in the WPW syndrome, one is reversible and AP-dependent atrial vulnerability and the other is intrinsic and AP-independent atrial vulnerability.26 It is very interesting the finding that some WPW patients with AF that undergo AP ablation have their atrial vulnerability parameters normalized to the point that AF is no longer inducible. This strongly suggests the presence of reversible and AP-dependent atrial vulnerability as the mechanism for AF in the WPW syndrome. Now the question is ¿why does the AP causes increased atrial vulnerability that is reversible in some patients but not reversible in others? There are only speculations to try to answer this question. The AP refractoriness might play a certain role. There is a tendency to shorter AP ERP in the anterograde and retrograde conduction in those patients whose AF remained noninducible. Nevertheless, it is difficult to understand how a small AP could have such a profound effect on overall atrial conduction. Although the mechanisms remain unexplained, it was demonstrated that WPW patients with AF appear to have both reversible and intrinsic AP-related atrial vulnerability. The WPW patients with AF have intrinsic atrial muscle abnormalities and most of them present abnormally prolonged and fractionated atrial electrograms that are recorded with atrial endocardial catheter mapping during sinus rhythm.14
Figure 3 Induction of fragmented atrial activity (FAA)
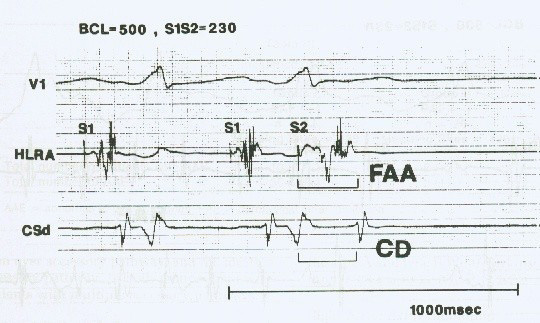
An example of the induction of fragmented atrial activity (FAA) as defined in the text. Surface electrocardiographic lead V1 is shown together with intracardiac electrograms from the high lateral right atrium (HLRA), and distal coronary sinus (CSd). S1 and S2 are, respectively, the driving and premature stimulus artifacts. The basic drive cycle length (BCL) was 500 ms and the coupling interval (S1 S2 interval) was 230 ms. There is a prolongation of the duration of atrial activity from 110 to 200 ms in the HLRA. CD indicates interatrial conduction delay. Reprinted with permission from Konoe A, Fukatani M, Tanigawa M, et al. Electrophysiological abnormalities of the atrial muscle in patients with manifest Wolff-Parkinson-White syndrome associated with paroxysmal atrial fibrillation. PACE 1992;15:1040-1052.
The role of an atrial firing focus as a trigger for AF initiation in the WPW syndrome is not well documented yet. AF can also be initiated by ectopic beats originating from the pulmonary veins, and elsewhere. The pulmonary veins are well established as the dominant sources of triggers in paroxysmal AF, in addition to their contribution to maintenance of AF.43 However, there is no available data suggesting that firing from the pulmonary veins is the main source of recurrent AF in WPW patients that had their AP ablated. The elimination of triggers of AF requires spontaneous firing to be readily identifiable during an ablation procedure. Ablation targeting the pulmonary vein-left atrial junction is effective in isolating the left atrium from proarrhythmic pulmonary vein activity. Despite the latest progress in AF ablation, there is limited knowledge of how to identify, map, and ablate the culprit atrial substrate in an individual patient, because AF is generally associated with locally complex electrograms of undefinable timing and sequence.43 This heterogeneity of substrate may explain why no single predetermined ablation technique is effective for all patients across the entire spectrum of AF. To the best of our knowledge, there is no detailed study addressing ablation of the pulmonary veins to suppress recurrent AF in WPW patients that had already undergone successful AP ablation.
Figure 4 Induction of interatrial conduction delay (CD)
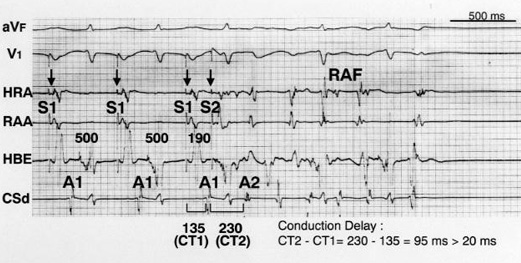
Atrial extrastimulus testing in a patient with paroxysmal AF showing atrial conduction delay (CD). S1 and A1 refer to the driving stimulus and the atrial electrogram, respectively, of the basic drive beat. S2 and A2 refer to the stimulus artifact and the atrial electrogram, respectively, of the induced premature beat. The atrial extrastimulus was programmed at a coupling interval of 190 ms with a driving cycle length of 500 ms. The S1-A1 interval in the distal coronary sinus was 135 ms. At the premature beat, S2-A2 interval prolonged to 230 msec. The maximum CD in this patient was 95 msec. This atrial CD led to repetitive atrial firing (RAF). HRA indicates high right lateral atrium; RAA, right atrial appendage; HBE, His bundle area; and CSd, distal coronary sinus. Reprinted with permission from Isomoto S, Centurión OA, Shibata R, et al. The effects of aging on the refractoriness and conduction of the atrium in patients with lone paroxysmal atrial fibrillation revealed with programmed atrial stimulation. Rev Soc Parag Cardiol 2005;3:25-30.
Figure 5 Induction of repetitive atrial firing (RAF)
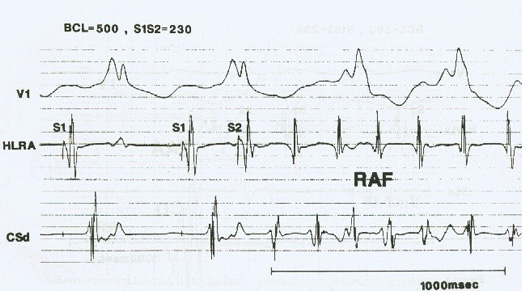
An example of the induction of repetitive atrial firing (RAF) as defined in the text. Surface electrocardiographic lead V1 is shown together with intracardiac electrograms from the high lateral right atrium (HLRA), and distal coronary sinus (CSd). S1 and S2 are, respectively, the driving and premature stimulus artifacts. The basic drive cycle length (BCL) was 500 ms and the coupling interval (S1 S2 interval) was 230 ms. Reprinted with permission from Konoe A, Fukatani M, Tanigawa M, et al. Electrophysiological abnormalities of the atrial muscle in patients with manifest Wolff-Parkinson-White syndrome associated with paroxysmal atrial fibrillation. PACE 1992;15:1040-1052.
Fragmented atrial activity
It is the widening of the local atrial electrogram in response to an atrial programmed extrastimulus testing. The mechanism producing fragmented atrial activity is not clear. Fragmented atrial activity might represent local continuous activity in response to premature beats. A single atrial extrastimulus delivered with a critical coupling interval often results in widening of the local atrial electrogram. Ohe et al44 defined it as the ocurrence of disorganized atrial activity ≥150% of the duration of the local atrial electro gram of the basic beat recorded in the high right atrium (Figure 3). Patients with WPW syndrome associated with AF have a wider fragmented atrial activity zone than those WPW patients without AF.14 This suggests that the widening of the fragmented atrial activity zone is closely related to the ocurrence of AF in patients with WPW syndrome.
Interatrial conduction delay, measured from the stimulus artifact to the atrial electrogram at the distal coronary sinus level, reflects an actual interatrial conduction delay that is not influenced by local latency at the site of stimulation, since the stimulation is performed in the high right atrium. Interatrial conduction delay was defined as an increase in the S2 through A2 interval of the extrastimulus >20 ms compared with the S1 through A1 of the basic drive (Figure 4). Aytemir et al45 demonstrated a significant increased in the maximum P wave duration and P wave dispersion after AP ablation reflecting more inhomogeneous and prolonged atrial conduction in patients with the WPW syndrome and AF episodes. Therefore, this increased P max and higher P wave dispersion values in patients with previous clinical AF episodes suggest the important role of inhomogenous and discontinuous propagation of sinus impulses in the development of AF in patients with the WPW syndrome. They demonstrated that the maximum P-wave duration and P-wave dispersion are independent predictors of recurrence of AF in patients with the WPW syndrome after successful radiofrequency catheter ablation of the AP. Hiraki et al46 demonstrated in a prospective study that P wave signal-averaged electrocardiography predicts recurrence of AF in patients with WPW syndrome who underwent successful catheter ablation. In order to reduce interatrial conduction delay and decrease atrial vulnerability, bi-atrial pacing was developed as a technique of simultaneous activation of the right atrium and left atrium.47 It has been reported to prevent the recurrence of AF in paced patients with marked interatrial conduction delay.48 Thus, these facts indicate that the interatrial conduction delay can play an important role in the onset of AF. It was shown that WPW patients associated with AF have a wider interatrial conduction delay zone than those WPW patients without AF.14 This suggests that the patients with AF would have a greater tendency to develop slow interatrial conduction in the setting of WPW syndrome.
Figure 6 Normal atrial endocardial electrograms
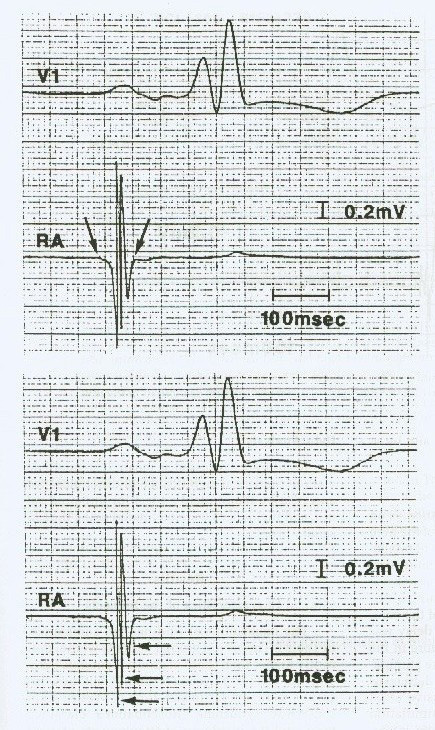
Examples of measurement of the duration (top), and the number of deflections (bottom) of the intraatrial electrogram. Surface electrocardiographic lead V1 is shown together with the right atrial electrogram (RA). In the top panel, the arrows show the onset and the end of the intraatrial electrogram. In the bottom panel, the arrows show the deflections of the intraatrial electrograms. Reprinted with permission from Konoe A, Fukatani M, Tanigawa M, et al. Electrophysiological abnormalities of the atrial muscle in patients with manifest Wolff-Parkinson-White syndrome associated with paroxysmal atrial fibrillation. PACE 1992;15:1040-1052.
Figure 7 Abnormally prolonged and fractionated atrial endocardial electrogram
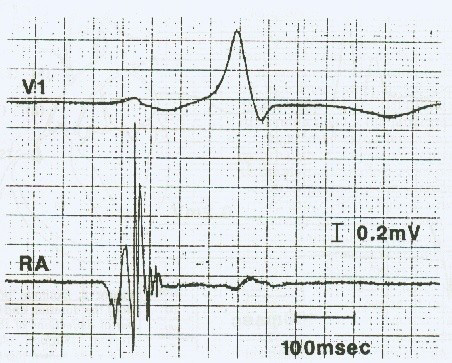
Example of an “abnormal atrial electrogram”. This abnormal atrial electrogram was recorded from high lateral right atrium (RA). Abnormal atrial electrogram as defined in the text. Reprinted with permission from Konoe A, Fukatani M, Tanigawa M, et al. Electrophysiological abnormalities of the atrial muscle in patients with manifest Wolff-Parkinson-White syndrome associated with paroxysmal atrial fibrillation. PACE 1992;15:1040-1052.
Repetitive atrial firing is defined as the occurrence of two or more successive atrial complexes with a return cycle of <250 ms and a subsequent cycle length of <300 ms(Figure 5). The maximum conduction delay refers to the maximum difference between the conduction time of the extrastimulus and that of the basic driven beat measured at the distal coronary sinus. These results suggest that the occurrence of repetitive atrial firing requires the presence of a short refractory period at the pacing site and prolongation of the maximum conduction delay. It was shown that WPW patients associated with AF have a wider repetitive atrial firing zone than those WPW patients without AF.14 This suggests that the patients with AF would have a greater tendency to develop repetitive atrial firing in response to an atrial premature contraction in the setting of WPW syndrome.
Abnormal atrial endocardial electrograms in sinus rhythm
The fractionated and prolonged duration of the abnormal atrial endocardial electrograms may indicate the presence of areas that possibly predispose the occurrence of reentrant circuits. At the time of atrial endocardial catheter mapping during sinus rhythm, the recording of an abnormally prolonged and fractionated right atrial electrogram may reflect slow and anisotropic conduction through a diseased atrial muscle.49,50 Tanigawa et al49 made the first attemp to define quantitative chracteristics of normal atrial endocardial electrograms with a catheter electrode mapping technique of the right atrium during sinus rhythm. They recorded atrial endocardial electrograms from the anterior, lateral, posterior and medial aspects of the high, middle, and low right atrium. The duration of the atrial electrograms was defined as the time from the beginning of the earliest electrical activity that deviated from the stable baseline to the last point of the atrial electrogram that crossed the baseline. The number of fragmented deflections was measured by counting the number of downward deflections (Figure 6). An abnormal atrial electrogram was defined as that having a duration ≥100 ms and 8 or more fragmented deflections (Figure 7). In a pathological study of fatal cases with WPW syndrome and sudden cardiac death, Basso et al51 observed a 50% incidence of isolated atrial myocarditis. Sudden death was the first manifestation of the disease in 40% of the cases. This finding of atrial inflamatory infiltrates in patients with the WPW syndrome supports the hypothesis that atrial inflammatory foci may act as a trigger of AF, which in turn precipitates sudden cardiac death due to rapid ventricular conduction that degenerates into ventricular fibrillation.52
Electrophysiological abnormalities of the atrial muscle in the WPW syndrome were identified by endocardial catheter mapping of the right atrium during sinus rhythm. Abnormally prolonged and fractionated atrial electrograms were frequently (83%) recorded in WPW patients associated with AF. However, these abnormal atrial electrograms were significantly less common (10%) in WPW patients without any evidence of AF. These electrophysiological abnormalities of the atrial muscle were more frequently and significantly found in the high right atrial sites distant from the atrioventricular groove and AP location. Since abnormally prolonged and fractionated atrial electrograms were also frequently found in patients with AF not associated to the WPW syndrome,49,50 it is suggested that the mechanism of abnormal atrial electrograms may not relate to the AP. Therefore, patients with the WPW syndrome associated with AF have a significantly high incidence of electrophysiological abnormalities ofthe atrial muscle which certainly play an important role in the occurrence of AF in these patients.
As suggested by one group, visualization and reatment needs further clarification.
The role of autonomic tone and advance age
Autonomic modulation of accessory pathway refractoriness and conduction became evident in experiments involving exercise, postural changes, and drugs.53,54 Time- and frequency-domain analysis of heart period variability performed in patients with paroxysmal AF suggests that autonomic modulation is important in selected patients55,56 Autonomic modulation as abnormal cardiac sympathetic activity may be related to the onset of AF in patients with WPW syndrome.57,58 It is relatively frequent to observe in the clinical setting that the onset of AF is associated to exercise or emotional stress in patients with WPW syndrome.11 Honda T et al.58 demonstrated an increased sympathoadrenal activity in WPW patients associated with AF, and concluded that augmented sympathoadrenal activity seems to play an important role in the genesis of AF in this syndrome. Patients with overt pre-excitation and spontaneous AF appear to exhibit predominance of sympathetic activity and vagal withdrawal which is consistent with shorter accessory pathway effective refractory periods, shorter cycle length of orthodromic AVRT, and shorter pre-excited RR intervals during AF in these patients.
Demonstration of electrophysiologic changes in the atrial muscle with age59,60 is consistent with the concept that electrical functional changes are related to histologic changes of the conduction system of the aging heart. Becker AE61 found that the structural atrial changes are fibrofatty replacement and patchy replacement fibrosis that involve the myocardial sleeves on pulmonary veins and sites of rapid conduction, such as the terminal crest and Bachmann’s bundle. Dagres N et al62 studied 116 consecutive patients with manifest or concealed accessory pathways and documented paroxysmal AF who underwent radiofrequency catheter ablation, and demonstrated that the recurrence rate of AF following successful ablation shows an age-related increase, being low in patients younger than 50 years of age and high in the older patients. The incidence of recurrent AF showed a statistical significant increase in patients older then 50 years (35%) as compare to those younger ones (12%). The recurrence rate of atrial fibrillation was even higher in patients older than 60 years (55%).
AF has a different dimension in the context of the WPW syndrome. Indeed, it may be life-threatening if an extremely rapid ventricular response develops in the presence of a fast AP degenerating into ventricular fibrillation. Therefore, it is very important to clearly understand the mechanisms involved in the development of AF in the WPW syndrome. AF has a reserved prognostic significance in patients with the WPW syndrome, and its incidence is relatively high in the absence of any clinical evidence of organic heart disease. Several mechanisms responsible for the genesis of AF in WPW patients were hypothesized, namely, spontaneous degeneration of AVRT into AF, electrical properties of the AP, the effects of AP on atrial architecture, the increased sympathetic activity and vagal withdrawal, the influence of advancing age, and intrinsic atrial muscle vulnerability. The existence of a retrograde multiple or multifiber AP is strongly related to AF inducibility, and the complex excitation inputs into the atrium over the retrograde multiple or multifiber AP facilitate the development of AF in WPW patients. The decrease incidence of AF after successful elimination of the AP, suggest that the AP itself may play an important role in the initiation of AF. However, AF still occurs in some patients with the WPW syndrome even after successful definitive elimination of the AP. There is an important evidence of an underlying atrial muscle disease in patients with the WPW syndrome. Abnormally prolonged and fractionated atrial endocardial electrograms are observed with a significantly higher incidence in WPW patients with documented episodes of AF. These electrophysiological abnormalities of the atrial muscle certainly play an important role in the occurrence of AF in these patients. Furthermore, the electrophysiological findings of altered atrial refractoriness, increased induction of repetitive atrial firing and increased intraatrial conduction delay suggest an intrinsic atrial vulnerability as the mechanism of AF in certain patients with the WPW syndrome. The atrial vulnerability in the WPW syndrome seems to be either, reversible and AP-dependent, or intrinsic and AP-independent atrial vulnerability. It is very interesting the finding that some WPW patients with AF that undergo AP ablation have their atrial vulnerability parameters normalized to the point that AF is no longer inducible. These facts strongly suggest the presence of different mechanisms of AF development in different patients with the WPW syndrome. A detailed electrophysiological examination before and after AP ablation could shed insight into the understanding of the mechanism for the genesis of AF in individual patients with the WPW syndrome.






