The Role of Atrial Fibrillation Catheter Ablation in Patients with Congestive Heart Failure: “Burning”for a Cure
Dimpi Patel, Mohammed Khan
Cleveland Clinic, Cleveland, OH
.
Atrial Fibrillation (AF) and congestive heart failure (CHF) often co-exist. Catheter ablation is increasingly used to cure AF related to CHF.Clinical evidence supports the feasibil- ity of catheter ablation as a treatment option in drug refractory AF patients with CHF.Investiga- tors have reported an improvement in ejection fraction, quality of life, and functional capacity
Correspondence to: Mohammed Khan, Cardiovascular Associates, Elk Grove Village, IL 60007, USA
The interaction between atrial fibrillation (AF) and congestive heart failure (CHF) is complex. There are many issues surrounding the pathophysiol- ogy, epidemiology, and treatment which are still debated. Nevertheless, the pernicious impact of the interplay between AF and CHF in terms of mor- bidity and mortality in patients’ lives is irrefutable. At present, patients with AF and coexistent CHF have several rate versus rhythm control op- tions available to them which use pharmacolog- ic and non-pharmacologic treatments. Rhythm strategies include antiarrhythmic medications, maze procedure, catheter ablation for AF, and implantable atrial defibrillator. Rate strategies include drugs and atrioventricular junction- al ablation (AVA) with permanent pacemaker. Antiarrhythmic drugs are often ineffective and have adverse effects. While surgical maze is very effective, it is technically complex and invasive. Pacing and atrial defibrillation can be somewhat effective; however, there are disadvantages such as warfarin therapy and implantation of a pacemak- er. Consequently, catheter ablation is increasingly being performed. In a direct comparison, pulmo- nary vein isolation (PVI) was shown to be supe rior to AVA with biventricular device (BI-V).1
This review article will address the emerg- ing role of catheter ablation in the treat- ment of AF in patients with coexistent CHF.
The AF and CHF Cardiovascular Epidemics:
AF affects 2.3 million individuals and accounts for over 350,000 U.S. hospitalizations annually.2 Two thirds of patients with AF are over the age of 65.3 Having CHF increases the risk of AF 4.5 fold in males and 5.9 fold in females.4 CHF affects over 5 million North Americans and accounts for over 995,000 U.S. hospitaliza- tions annually. The prevalence of AF directly in- creases with New York Heart Association Class Association (NYHA) severity. Ten to 26% of pa- tients have AF with NYHA Class II-III and 30-
50% patients have AF with NYHA Class IV.5-9
AF as a Predictor of Worse Outcomes in
Patients with CHF:
At present, there is no consensus as to whether
the presence of AF is an independent predictor for mortality in patients with CHF. In the Vasodilator Heart Failure Trial (V-HeFT), the presence of AF in patients with mild to moderate CHF was
not associated with worse outcome10 Coversely, in the larger Studies of Left Ventricular Dysfunction (SOLVD) trial, AF was an independent predictor for all-cause mortality, the com-bined endpoint point of death, and hospitalization for heart failure.11 In the Carvedilol or Metoprolol European Trial (COMET) having AFsignificantly increased the risk for death and heart failure hospitalization.However, after adjusting for confounding factors, AF was found not to be an independent risk factor for mortality.12 Middlekauf et al. and Correll et al. reported that the presence of AF in patients with CHF was associated with increased mortality. Additionally,in patients with mild to moderate CHF, AF seemed to be a stronger predictor of negative outcome compared with patients with severe heart failure. The findings from most of these studies suggest that having AF is an independent risk factor for mortality in congestive heart failure. Moreover, in terms of mortality, the effect of AF is inversely proportional to the severity of CHF.13,14,15
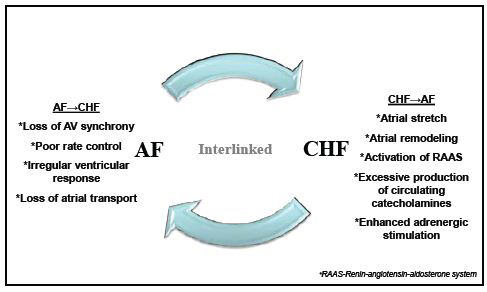
Figure 1 Schema depicting the integration of CHF and AF. A list of factors contribution to the exacerbation of AF and CHF
The Interplay between CHF and AF:
The causative relationship between the AF and CHF has not been fully elucidated. Their coexistence can be partially explained by shared risk factors such as age, hypertension, diabetes, obesity, valvular, ischemic and nonischemic structural heart disease. These conditions cause myocardial cellular and extracellular alterations and electrophysiological and neurohormonal changes which interplay to create an environment that predisposes the heart to CHF and AF.Tachycardia, increased cardiac filling pressures, irregular heart rate, loss in atrial transport, and atrioventicular desynchrony are all traits inherent to AF which can impair ven- tricular function and worsen CHF (Figure 1)15
CHF, through a series of physiological process- es, can cause AF or sustained AF. Sustained AF can result in electrical and structural remodel- ing of the left atrium. This environment pro- motes arrhythmogenesis which in turn exac- erbates CHF (Figure 2). Whether AF causes CHF or CHF causes AF is still debated.15
The Electrophysiology of the Pulmonary
Veins:
In 1998, Haissaguerre et al. observed that parox-
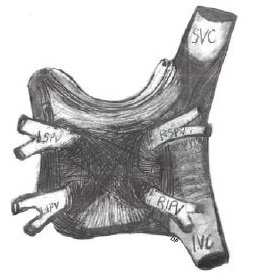
ysmal AF was focal in origin and was initiated by triggers in the pulmonary veins. These triggers could successfully be ablated with radiofrequency energy16.The anatomical substrate of these triggers is the pulmonary vein fascicles .17These fascicles are muscular sleeves which extend from the left atrium in a longitudinal and circular manner.The fascicles have patent elec- trical properties that allow rapid firing which is conducive to the initiation and propagation of AF.18,19 Because of the risk of PV stenosis, abla- tion techniques do not target the triggers within the vein, but rather electrically isolate the pulmo- nary veins by ablating all of the fascicles (Figure 3).
Catheter Ablation for Atrial Fibrillation:
There have been several advances in the field of
catheter ablation of atrial fibrillation in the last 10
years. Catheter ablation has evolved from an ex-
perimental therapy to one that is routinely performed in experienced centers worldwide Preliminary results from the Catheter Ablation vs.Antiarrhythmic Drug Therapy for Atrial Fibrillation(CABANA) trial suggest that catheter ablation is superior to drug therapy. Freedom from recurrence of symptomatic AF was significantly higher in the ablation group (65% vs. 41%; HR=0.42; 95% CI, 0.19-0.95). This exciting finding validates the benefits of catheter ablation result and may result in more procedures being performed annually and making catheter ablation a mainstay of AF treatment.20
Comparing Different Techniques:
Currently, there is no single accepted dogma on
catheter ablation. Catheter ablation strategies can be
divided into isolation of the pulmonary veins alone
and pulmonary vein isolation with additional lesion
sets. Most electrophysiologists create adjunctive
lesions particularly in patients with non-paroxys- mal AF; however, which sites and how to identify where to place these lesion sets are still debated.
Figure 2 Diagram of tFhigeurer1elationship between CHF and the pathophysiology of atrial remodeling. A list of fac- tors which contribute to atrial electrical and structural remodeling (gray shaded).
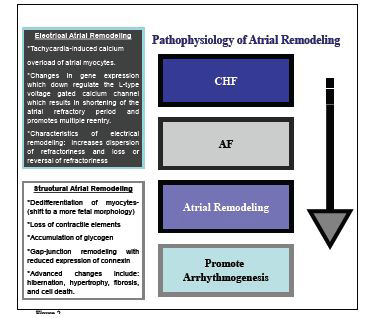
Figure 3 Sketch of the anatomy of the left atrium, pulmonary veins, and muscular fascicles (modified from 52). IVC- Inferior Vena Cava; SVC-Superior Vena Cava; RSPV-Right Superior Pulmonary Vein; RIPV-Right Inferior Pulmonary Vein; LSPV-Left Superior Pulmonary Vein; LIPV-Left Inferior Pulmonary Vein. Drawing recreated by Dimpi Patel.
Pulmonary Vein Ablation Alone:
Pulmonary veins/antrum ablation is performed
segmentally, guided by a circular mapping cath-
eter or by a continuous circumferential ablation
lines which are created to surround the right or
left pulmonary veins.21,22 The creation of the
circumferential ablation/isolation line is guided
by 3D electroanatomical mapping, fluoroscopy,
or by intracardiac echocardiography.23,24,25,13 Circumferential ablation targets ipsilateral
pulmonary veins separately or both ipsilateral
pulmonary veins together. The procedural end-
points are amplitude reduction within the tar-
geted area, elimination or dissociation of the
pulmonary vein potentials recorded from the cir-
cular mapping catheters, and/or exit block from
the pulmonary veins.27 At 6-month follow-up,
54% of patients who had circumferential pulmo-
nary vein ablation and 82% of patients who had
segmental PVI remained free of arrhythmia.28
Pulmonary Vein Ablation with Additional
Lesion Sets:
TPVI is a cornerstone of most ablation proce-
dures; however, if a focal trigger is identified out-
side the pulmonary veins it should be targeted
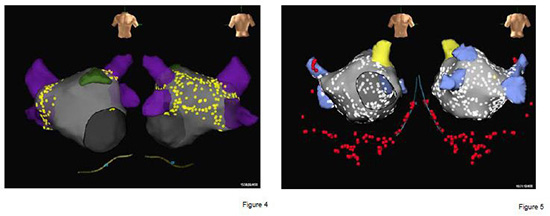
during the procedure (Figure 4 and 5). Non-PV
atrial triggers have been found in the posterior
wall of the left atrium, the superior vena cava,
the fossa ovalis, the coronary sinus, the ligament
of Marshall behind the Eustachian ridge, cris- ta terminalis, and adjacent to the AV valve an- nuli. An isoproterenol challenge (up to 20: µg/ min) can be used to find non-PV triggers.29-33
CFAE (complex fractionated electrical electro- grams) are electrograms with highly fraction- ated potentials or with a very short cycle length (≥120 ms) which can be targeted during ablation. It has been suggested that CFAEs represent sub- strate areas that perpetuate AF. The primary end- points are elimination of CFAEs areas, conver- sion of AF to sinus rhythm, and/or an inability to induce AF. In patients with paroxysmal AF, the procedural endpoint is noninducibility of AF. In patients with persistent AF, the endpoint is termi- nation of AF. If atrial flutter or atrial tachycardia ensues after elimination of the CFAE areas, the atrial arrhythmias are mapped and ablated.34,35,36,37.At the one year follow-up, 91% patients were free of arrhythmia and symptoms.34
A tailored AF ablation approach targets specific drivers of AF without excess anatomical abla- tion. An electrogram based approach is used in- stead of a standardized lesion set. The pulmonary veins are isolated first if a rapid electrical activity is found. If AF persists, complex electrograms in the left atrium, coronary sinus, and superior vena cava are ablated. In patients with paroxysmal AF, the endpoint is noninducibility of AF with isopro- terenol challenge. At 11±4 month follow-up, 77%
of patients were free from AF and/or atrial flut-
ter without the use of antiarrhythmic drugs.38
In patients with longstanding persistent AF, a step-wise approach is reported to be success- ful. The pulmonary veins are electrically isolated guided by a circular mapping catheter. If AF has not terminated, a roof line is made. If AF contin- ues, the coronary sinus and complex left atrium activities are targeted. If AF persists and there is perimitral macroreentry, mitral isthmus ablation is performed. If the AF cannot be resolved, an op- tional ablation of the right atrial/SVC can be done.
Figure 4 and 5 3-D electroanatomical reconstruction of the left atrium in patients with paroxysmal AF and LSPAF
If AF is not terminated at that point, the patient is either electrically or pharmacologically cardio- verted. The endpoint of ablation is restoration of sinus rhythm, which normally occurs via one or more atrial tachycardia intermediates . At 1 year, after multiple procedures and with an- tiarrhythmic drugs when needed, 95% of LSPAF patients had freedom from arrhythmia.39,40,41
Performing Catheter Ablation in Patients with CHF:
PVI is an intricate procedure.Success is vari- able based on operator experience.Currently, the majority of the cases are performed in patients with normal systolic function.However, since there is an ever expanding popu- lation of patients with CHF and concomitant AF, more ablations are being performed in patients with depressed ejection fraction (EF)
Obstacles of Catheter Ablation in Patients with CHF
PVI in patients with CHF has its own unique set of obstacles. Patients with lower EFs tend to have larger pulmonary vein ostia and left atria, and con- sequently larger areas needs to be ablated. More- over, patients with left atrial dysfunction tend to have atrial remodeling, which could result in thickening of the areas that are targeted for abla- tion. CHF patients often have more complex atrial substrates. Therefore, ablation protocols need to include targeting non-pulmonary vein triggers and to completely isolate the posterior wall. The prevalence of non-PV triggers range from 30% to more than 50% in patients with non-PAF.42
Irrigated catheters are efficacious in this popula- tion because they are able to accurately deliver energy.On the other hand, externally irrigated catheters require a large infusion of saline during a procedure and CHF symptoms may be seen or ex- acerbated. Therefore, CHF patients should be carefully monitored and have aggressive postoperative management with diuretics. Patel et al. reported that despite routine administration of diuretics,4% of patients experience fluid retention requiring rehospitalization after ablation with an open irri- gation catheter. Most rehospitalized patients were obese males with chronic atrial fibrillation.43
Postoperative Management:
Postoperative management varies depending on
center protocol and physician’s discretion.How-ever, it is recommended that warfarin should beadministered for at least two months follow-
ing an AF ablation procedure.Whether to use warfarin longer than two months following ablation should be based on the patient’s risk factors for stroke and not on the presence or type of AF. Cessation of warfarin therapy after ablation is generally not recommended in patients who have a CHADS score ≥ 2. Considering this rec-ommendation and the common risk factors associated with CHF, many CHF patients are kept on warfarin indefinitely after catheter ablation.
Suppressive antiarrhythmic drugs are often used
during the first one to three months after abla- tion. Most electrophysiologists use drugs that have been used unsuccessfully prior to ablation
Patients should be seen in follow-up at a minimum of three months following the ablation procedure and every six months henceforth for at least two years. ECGs should be obtained at all follow-up visits. Patients complaining of palpitations should be evaluated with an event monitor. The most ef- fective way to monitor frequent asymptomatic recurrences is to use a 1 to 7 day Holter monitor.
There is no set protocol for imaging studies to screen for PV stenosis following ablation.Ide-ally, most patients should have computed to- mography at baseline and at 3 months after ab- lation to assess for pulmonary vein stenosis.
Early recurrences of AF and/or atrial tachy- cardia are often seen in the first two to three months after AF ablation. Recurrences of AF during this blanking period are not consid- ered procedure failure. Therefore, repeat abla- tion procedures should be postponed for at least three months following the first procedure44
Complications of Catheter Ablation:
Table 1. Studies of patients with low ejection fractions undergoing atrial fibrillation ablation
|
Number of patients |
EF Pre-ablation (%) |
LA (cm) |
EF Post-ablation (%) |
AF Free (%) |
| Hsu23 |
58 |
35 |
5 |
56 |
69 |
| Chen22 |
94 |
36 |
4.7 |
41 |
73 |
| Tondo24 |
40 |
33 |
4.8 |
47 |
62 |
| Gentlesk25+ |
67 |
42 |
- |
56 |
86 |
| Khan1 |
41 |
27 |
4.9 |
35 |
88 |
| Bortone26* |
6 |
25 |
- |
54 |
100 |
+Freedom from AF reported with some patients on antiarrhythmics *5 out of 6 patients had redo procedures. 1 patient had an post procedural EF of 30. It is not included in the mean
Pulmonary vein stenosis, atrioesophageal fistula, pericardialeffusion,cardiactamponade,hematoma, and cerbrovascular accident are all possible compli- cations of PVI. There are no differences in the rates of complications in patients who underwent PVI with CHF compared to those without CHF.44,45
Clinical Evidence Supporting the Feasibility of Pulmonary Vein Isolation as a Treatment Strategy in Patients with CHF
Several studies have assessed the feasibility of pul-
monary vein isolation in a CHF population (Table 1).
Hsu et al. compared 58 patients with CHF to 58 case controlled patients without CHF that underwent catheter ablation. CHF patients had an EF below45% and ≥ NYHA class II. Fifty percent of patients with CHF and 47% of patients in the control group underwent a second procedure.
One year after the final procedure, 78% of patients with CHF and 84% of the controls were free of AF (P=0.34). EF increased by an average 21%, left ventricular end- diastolic and end-systolic diameters decreased re- spectively by 7 and 9mm in the CHF group. Cath- eter ablation in this study involved PVI with one or more linear lesions, which include a roof line between the left and right superior pulmonary veins and a mitral isthmus line between the mi- tral annulus and left inferior pulmonary vein.46
Chen et al. studied 377 patients. Ninety-four pa- tients had EF < 40% versus 286 EF = 40%. All patients had symptomatic AF refractory to antiarrhythmic drugs and were rate controlled. PVAI with cavotri- cuspid isthmus line was performed. At 14 months,73% of the low EF groups were AF free compared to 87% of the normal EF group (p-value 0.03). Twenty-one of the patients with LV systolic dysfunction underwent repeat PVI. The overall cure rate in patients with LV systolic dysfunction after a second procedure was 96%. Nineteen of the study group had repeat procedures. The overall cure rate in the study group was 94%. The study group had a non- significant increase in EF of 4.6% and significant improvement in quality of life. Complication rateswere low with a 1% PV risk of PV stenosis.45
Unlike Hsu et al., more patients in Chen et al. had improvement in EF; however, this finding can be attributed to the smaller number of non-paroxys- mal AF patients in the study by Chen et al. The requirement for rate control in the study by Chen et al. may have limited the number of patients with tachycardia-mediated cardiomyopathy.45,46 Tondo et al. prospectively compared 40 patients with EFs of <40% to 65 patients with EFs =40%. A hybrid ablation procedure which included electro- anatomical mapping-guided PVAI, a mitral isth- mus line, and in most patients, ablation of the ca- votricuspid isthmus was performed. Eighty-seven percent of patients with impaired EF were arrhyth- mia free and had improvement in EF from 33±2% to 47±3% at 14±2 months. Ninety-two percent of pa- tients with normal EF were in sinus rhythm at the end of the follow up period with or without antiar- rhythmic drugs. Exercise capacity, symptoms, and quality of life scores improved significantly.47
Gentlesk et al. studied 67 patients with a mean EF of 42±9 compared to 299 with normal EF. Abla- tion consisted of proximal isolation of the pulmo- nary veins and non-pulmonary vein triggers. EF was assessed at 24 hours after ablation and then again at 6 months. At the end of the follow up period, 86% of the left ventricular dysfunction group was arrhythmia free compared to 87% of the control group. However, more repeat proce- dures were required in patients with left ventricu- lar dysfunction (1.6±0.8 vs. 1.3±0.6; P<or=0.05). In the lower EF group, EF increased from 42±9% to 56±8% (P<0.001) after ablation. These results im- ply that depressed EF is reversible with success- ful catheter ablation in many CHF patients with AF induced ventricular cardiomyopathy.48
The Pulmonary Vein Antrum Isolation (PVAI) ver- sus AV node Ablation with Bi-Ventricular (BI-V) Pacing for treatment of Atrial Fibrillation in Patients with Congestive Heart Failure (PABA-CHF) was a multicenter, randomized study that compared PVAI to AVA with BI-V in patients with a low EF and symptomatic AF. Forty-one patients underwent PVAI with a mean EF of 27±8 and 40 patients un- derwent AVA with a mean EF of 29±7. All patients had drug refractory AF and NYHA class II or III.1
Khan et al. found that the composite primary end-
point favored the PVAI group because they had greater improvement in the quality of life ques- tionnaire at 6 months (60 vs. 82 in the AVA group; P<0.0001), a longer 6-minute-walk-distance (340m vs. 297m; P<0.001), and a higher ejection fraction (35% vs. 28%; P<0.001). There were eight repeat procedures for recurrent AF (in four patients) and atrial flutter or atrial tachycardia (in four other patients) in the PVAI group. At 6 months, 88% of the PVAI group and 71% of the AVA group were free of AF without antiarrhythmic drugs.1
In the PVAI group, 2 patients had pulmonary vein stenosis, 1 had pericardial effusion, and 1 had pul- monary edema. In the AVA group, 1 had a lead dis- placement and the other had a pneumothorax.1
Bortone et al. studied six subjects with an EF of
25.8±7.3% who had drug refractory LSPAF. Five
patients had dilated cardiomyopathy and 1 pa-
tient had ischemic cardiomyopathy. Patients had
NYHA III-IV. All patients underwent stepwise
ablation. All patients with dilated cardiomypathy
had significant improvement in NYHA class and
EF. In the patient with the ischemic cardiomyopa-
thy, NYHA class improved but not the EF. Four
out of 5 patients in the dilated cardiomyopathy
group and the ischemic cardiomypathy group had
redo procedures. Sinus rhythm was maintained in
all patients. EF and NYHA improved in the dilated
cardiomyopathy group (54±4.4%, NYHA I-II) thus,
precluding the need for an implantable cardiovert-
er defibrillator (ICD). EF remained at 30% in the
patient with ischemic cardiomypathy, thus an ICD
was implanted. While this study was extremely
small, it demonstrated that even more severe pa-
tients can benefit from catheter ablation.49
The results from these studies stalwartly suggest the benefits of restoring and maintaining sinus rhythm with catheter ablation in patients with CHF. Moreover, these studies suggest that repeat procedures in this population are very effective.
Conclusions: Burning for a Cure for CHF
coexistent AF
CHF and AF are noxious to patient well-being, overall quality of life and health care cost. Per- haps the continual advances in ablation technol- ogy and the broadening indications for treatment may reduce the deleterious effect of CHF and AF.
Fairly recently, advances have been made that focus on enabling inexperienced operators to perform the procedure safely and effectively. Three-dimensional electroanatomical imaging has been integrated with other imaging modali- ties such as CT and MRI, allowing for better vi- sualization of the left atrial anatomy. Electroana- tomical mapping has been particularly beneficial in patients with CHF since extensive ablation and navigation in this anatomy can be difficult.
Robotic technology has emerged as a powerful device for mapping and ablating AF. There are two robotic systems that are being used for cath- eter ablation: Stereotaxis remote magnetic naviga- tion and Hansen Sensei robotic catheter system. Early clinical experiences with these devices are promising. Robotically guided mapping and ab- lation may improve both the ease and outcome of complex AF ablations. At present, there are no reported clinical trials focusing on the efficacy of robotic systems in CHF populations.50,51
Presently, catheter ablation for AF in CHF pa- tients is considered second line therapy.None- theless, as experience grows in this population and more favorable evidence continues to mount, this will change.In our opinion, it is possible that in the future, catheter ablation may become the treatment of choice in most patients with AF and concomitant CHF; henceforth, “burn- ing” could incinerate the AF with CHF epidemic.






