Amiodarone Induced Thyrotoxicosis – Fluctuating RVOT and LV Scar VT
Jayasree Pillarisetti MD, Subba reddy Vanga MD, Dhanunjaya Lakkireddy MD.
Mid America Cardiology @ University of Kansas Hospitals, Kansas City, KS.
A 61 year old patient with non-ischemic cardiomyopathy and implantable cardioverter defibrillator presented with multiple shocks for ventricular tachycardia (VT). EKG revealed monomorphic sustained VT which was left bundle inferior axis that spontaneously changed into sustained VT which was right bundle superior axis. This was suggestive of an outflow tract VT transforming into a VT probably related to reentry from LV scar. The patient was transferred to our university for VT ablation. However, further investigation revealed amiodarone induced hyperthyroidism which was the cause of his ventricular tachycardia storm. Reversible causes of VT should be considered before proceeding with radiofrequency ablation.
Correspondence to:
Dhanunjaya Lakkireddy MD, FACC, Director – Center for Excellence in Atrial Fibrillation EP Research, Professor of Medicine, Bloch Heart Rhythm Center, Mid America Cardiology @ University of Kansas Hospitals, Kansas City, KS 66196.
A 61-year-old African- American male with non-ischemic cardiomyopathy (EF 30%) with ICD, hypertension and chronic renal insufficiency was admitted to a VA hospital with multiple ICD shocks for incessant VT. He received a single shock three years ago for which he was started on sotalol. Six months ago he had multiple inappropriate shocks when his ICD was interrogated and replaced. Sotalol was also switched to amiodarone 200mg twice daily. Three months ago he had 2 shocks and his amiodarone dose was increased.
The day before he presented to the VA hospital, he was in ventricular tachycardia (VT) storm and received 13 shocks over 12 hours. The shocks were effective but he continued to have recurrent VT with changing morphology. His amiodarone dose was further increased to 400mg twice daily and was also started on lidocaine 3 mg/min and mexiletine 150 mg twice a day . He was then transferred to our hospital for possible VT ablation.
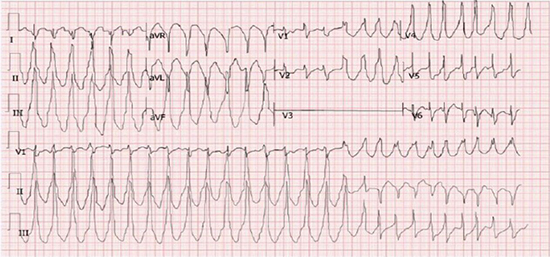
The patient upon arrival denied any chest pain. A recent stress thallium at his primary cardiologist office was negative for any reversible ischemia. His physical examination was unremarkable except for a soft systolic ejection murmur. Baseline ECG revealed normal sinus rhythm with rate of 75 beats per minute with normal axis, nonspecific intraventricular conduction delay, and nonspecific ST-T wave changes. QT interval was normal. Labs were unremarkable with a potassium of 4.1 mEq/L, magnesium of 2.2 mg/dL and a creatinine 3.24 mg/dL Recent echocardiogram showed EF of 30% with diffuse left ventricular hypokinesis. LV end diastolic diameter was 6cm.EKG revealed monomorphic sustained VT which was left bundle inferior axis at a cycle length of 360 msec (VT1). That spontaneously changed into sustained VT at 330 msec which was right bundle superior axis (VT2) (Figure 1). This was suggestive of an outflow tract VT transforming into a reentrant LV scar VT. Further workup showed markedly reduced TSH levels at 0.01 IU/ and elevated free T4 at 5 ng/dL indicating hyperthyroidism. Hyperthyroidism was most likely induced by amiodarone and was a reversible cause for his VT storm. All the VT episodes were always VT1morphology converting into VT2. We suspected that hyperthyroidism could be the precipitating factor in initiating VT1 (outflow tract origin) which in turn initiated VT2 that was more suggestive of reentry VT from LV scar.
Figure 1. EKG demonstrating RVOT VT (VT1) converting into scar VT with right bundle superior axis (VT2)
Amiodarone was then held, beta blockade was increased and endocrinology was consulted. They started him on propylthiouracil (PTU) 200mg three times daily. The decision was made to treat his hyperthyroidism before considering radiofrequency ablation of his VT. VT frequency dramatically decreased within 12 hours of initiating propranolol and PTU. Patient continued to have nonsustained runs of VT2 and was restarted on amiodarone at a low dose of 200mg daily after consultation with endocrinology. After 6 weeks of follow up his TSH and free T4 levels remained slightly above the normal range and he was switched to quinidine 300mg BID and mexilitine 200mg BID. At six months follow up no more VT was noted.
Our patient presented in RVOT VT which subsequentlykept fluctuating to a mid LV posterior break out consistent with the patients underlying LV scar. Most likely, Amiodarone induced thyrotoxicosis caused the RVOT VT and also provided the necessary trigger to sustain a VT circuit on the left side related to the scar. Suppression of the thyroid with drugs essentially removed the VT trigger and patient became arrhythmia free.
Few case reports have mentioned the change in morphologies of VT in different circumstances. One case report showed the change in axis during radiofrequency ablation from RBBB left axis to RBBB right axis. Another case reported alternate beats of different morphologies, LBBB with superior axis converting to LBBB with inferior axis produced by two different pathways with different refractory periods.1,2 Our case was similar where LBBB with inferior axis converted into RBBB with superior axis.
Amiodarone is a known cause of hyperthyroidism in 1%-23% of patients.3 In a Japanese study 31% of the patients with amiodarone induced hyperthyroidism (AIH) developed ventricular tachyarrhythmias compared to 3% when they were euthyroid.4 Hence it is important to have strict thyroid surveillance on a regular basis after initiating amiodarone. In our case the patient’s only presentation of AIH was VT storm. Therapy for AIH should be individualized on a case by case basis. Because amiodarone has a long elimination half-life, discontinuation of the drug may not immediately resolve the thyrotoxicosis. Often, anti-thyroid medication is given in conjunction with continued amiodarone in case of recalcitrant arrhythmias.5
Though ablation can be a curative treatment of VT in some cases, potentially reversible conditions causing VT should always be excluded. Our case represents one of the best examples of iatrogenic VT which could have been easily diagnosed and treated prior to considering ablation.
Reversible causes of VT should be considered before proceeding with radiofrequency ablation.
No disclosures relevant to this article were made by the authors.






