Atrial fibrillation (AF) is the most frequent sus- tained arrhythmia in clinical practice. The prev- alence of AF increases with age, from 0.5% at
40–50 years, to 5–15% at 80 years. Overall, it affects 1–2% of subjects. However, due to the con- tinuous ageing of the population, it is very likely that these numbers will increase in the follow- ing 50 years.1-3 Remarkably, the presence of AF doubles the mortality rates and is associated with a greater risk of stroke and heart failure.4,5
Hypertension is one of the main cardiovascular risk factors. However, hypertension does not only increase the risk of developing ischemic heart dis- ease, heart failure, stroke or renal insufficiency, but also is a risk factor for incident AF and for AF-related complications such as stroke and sys- temic thrombo-embolism.6 In fact, hyperten- sion is the most important risk factor for AF on
a population basis. Thus, although diabetes con- ferred a 1.4- (men) and 1.6-(women) fold risk, and hypertension a 1.5- and 1.4-fold risk, respectively, because of its high prevalence in the population, hypertension was responsible for more AF in the population (14%) than any other risk factor.7
Hypertension and AF are closely related. A sig- nificant proportion of hypertensive patients will develop AF, and vice versa, hypertension is a very common condition in patients with AF. Hyperten- sion causes structural and electrophysiological changes in the heart that promote the development of AF.8 This issue is very relevant, since the con- comitance of both markedly increases the risk of cardiovascular outcomes.6 However, does anti- hypertensive treatment change the clinical course and the prognosis of patients with hypertension and AF? In this review, the available evidence about the relationship between these conditions and the best therapeutic approach is analyzed.
Epidemiology, clinical profile of patients with hypertension and atrial fibrillation and risk factors for developing atrial fibrillation
The presence of hypertension increases the risk of development AF. Thus, in a recent study performed in primary care in 119,526 outpatients (mean age
52.9±15.2 years; 40.9% male), 7,260 subjects suffered from AF (6.1%). AF was more frequent in those pa- tients with hypertension (14% vs 1.9%; p<0.001),9 and when other comorbidities are present in hypertensive population, the risk of AF markedly rises. In a study performed in 2,024 patients with chronic ischemic heart disease and hypertension,
338 (16.7%) exhibited AF.10 On the other hand, in patients with AF hypertension is very frequent, in- creasing these numbers with the presence of other comorbidities. In a cross-sectional study performed in 32,051 outpatients and attended by 1,159 physi- cians specialized in primary-care
Table 1. Clinical profile of patients with chronic ischemic heart disease and hyperten- sion according to the presence of atrial fibrillation and clinical profile of patients with atrial fibrillation, according to the presence of hypertension (adapted from 9 and 13).
|
Patients with chronic ischemic heart disease and hypertension attended by cardiologists |
Patients with AF attended by
General Practitioners |
|
With
Hypertension |
Atrial Fibrillation |
P |
With
Hypertension |
P |
| Age (years) |
65.9 |
71.3 |
<0.001 |
72.3 |
66.7 |
<0.001 |
| Gender (men, %) |
71.0 |
54.7 |
<0.001 |
52.1 |
55.5 |
NS |
| Hypercholesterolemia (%) |
79.5 |
72.2 |
0.02 |
71.0 |
66.0 |
0.048 |
| Diabetes (%) |
30.1 |
44.6 |
<0.001 |
35.6 |
10.4 |
<0.001 |
| Ischemic heart disease (%) |
100 |
100 |
NS |
22.0 |
5.6 |
<0.001 |
| Heart failure (%) |
13.6 |
42.9 |
<0.001 |
22.5 |
6.1 |
<0.001 |
| Peripheral arterial disease (%) |
14.6 |
22.2 |
0.001 |
10.0 |
5.1 |
<0.001 |
| Renal disease (%) |
9.9 |
25.3 |
<0.001 |
12.3 |
4.1 |
<0.001 |
| Stroke (%) |
6.9 |
16.3 |
<0.001 |
11.5 |
5.1 |
<0.001 |
(79%) and cardiol- ogy (21%) in Spain, arterial hypertension was diag- nosed in 25% of the patients with AF.11 In a study performed in 756 patients with AF in France, car- diac disorders were present in 534 patients (70.6%), being hypertension (39.4%), coronary artery dis- ease (16.6%), and myocardial diseases (15.3%), be- ing the most common causes.12 In another study developed in a Primary Care setting in Spain, 92.6% of patients with AF had history of hypertension.9
But, does the clinical profile differ according to the presence of AF in patients with hypertension and vice versa according to the presence of hy- pertension in subjects with AF? Different studies have analyzed this issue. In patients with AF, the presence of hypertension was associated with a higher proportion of hypercholesterolemia, dia- betes mellitus, metabolic syndrome, sedentary life style, as well as more vascular diseases (heart fail- ure, ischemic heart disease, cardiac valve diseas- es, renal insufficiency, stroke, peripheral arterial disease and advanced retinopathy).9 Similarly, the presence of AF in patients with hyperten- sion and chronic ischemic heart disease was as- sociated with more diabetes and comorbidities (Table 1).13 This worse clinical profile found in patients with hypertension and AF may ex- plain at least in part the increased mortality rates of this population.14 Thus, not surprisingly, the death rates are doubled by AF, independent- ly of other known predictors of mortality.5,15
These data clearly show that AF is increased in patients with hypertension. But, which factors increase the likelihood of de- veloping AF in patients with hypertension?
Blood pressure control is crucial to improve car- diovascular prognosis in hypertensive popula- tion. Even small elevations above optimal blood pressure values increase the probability of cardio- vascular disease. In 1990, MacMahon et al. dem- onstrated that blood pressure reduction was criti- cal to decrease the risk of cardiovascular outcomes and
preventing major coronary events.16 How- ever, although blood pressure control is neces- sary, clinical practice guidelines agree that the aim of therapeutic approach in hypertensive popula- tion should not only be to control blood pressure but to reduce cardiovascular risk. Thus, a multi- factorial intervention is necessary to actually im- prove cardiovascular prognosis in this popula- tion, including the reduction of new-onset AF17
In a study that included 34,221 women participat- ing in the Women’s Health Study, after 12.4 years of follow-up, 644 incident AF events occurred. Blood pressure was strongly associated with incident AF, and systolic blood pressure was a better predictor than diastolic blood pressure. Even more, systolic blood pressure levels within the nonhypertensive range were independently associated with incident AF.18 In light of these results, some authors have suggested that it should be investigated whether AF is a marker of risk or directly a cardiovascular risk factor by itself in hypertensive patients and that fu- ture hypertension guidelines should assign a more important role to AF for cardiovascular risk strati- fication in this population.19 In another study aimed to determine whether the risk of incident AF among patients treated for hypertension differed by the degree of blood pressure control, uncontrolled elevated systolic blood pressure and systolic blood pressure <120 mm Hg, these variables were asso- ciated with an increased risk of incident AF.20
Unfortunately, the presence of AF is related with a worse blood pressure control.13
Chronic kidney disease is a powerful predictor of cardiovascular morbidity and mortality. Hyper- tension is one of the main causes of renal insuf- ficiency.17 In a study performed in 1,118 hyper- tensive patients, without previous paroxysmal AF, heart failure, myocardial infarction, or val- vular disease, the complication of chronic kidney disease, especially progressed renal dysfunction, was a powerful predictor of new-onset AF, inde- pendently of left ventricular hypertrophy and left atrial dilatation21 Moreover, chronic kidney disease increases the risk of thromboembolism in patients with AF, particularly in patients with hy- pertension, which markedly increases morbidity and mortality in this population.22 As a result, to reduce the risk of new-onset AF in hypertensive patients, one of the goals should be to prevent or atleast delay the development of renal dysfunction. Left ventricular hypertrophy is the most impor- tant subclinical cardiac organ damage in hyper- tensive population.23 Its early detection and treatment is essential in clinical practice, not only because LVH regression is associated with a marked improvement in cardiovascular progno- sis, but also because it may reduce some poten- tially related complications, including AF.24 In a study performed in 2,482 hypertensive subjects, after 16 years-period follow-up, a first episode of AF occurred in 61 subjects at a rate of 0.46 per 100 person-years. Age and left ventricular mass (both P<0.001) were the sole independent predictors of AF. For every 1 standard deviation increase in left ventricular mass, the risk of AF was increased 1.20 times (95% CI, 1.07 to 1.34). AF became chronic in
33% of subjects, and age, left ventricular mass, and left atrial diameter (all P<0.01) were independent predictors for the development of chronic AF.25
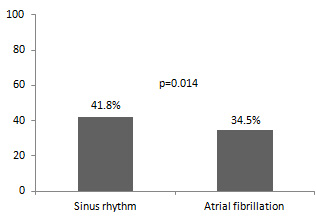
Figure 1 Blood pressure control rates in patients with hypertension and chronic ischemic heart disease according to the presence of atrial fibrillation (adapted from 13).
This is very relevant, since in hypertensive patients with left ventricular hypertrophy, the development of AF is associated with a worse prognosis, with a significant increase of fatal and non-fatal strokes.26 As previously commented, left ventricular hypertrophy is associated with an increased risk of AF and this association might be in part mediated via left atrial enlargement. Both, left ventricular hypertrophy and AF independently promote left atrial enlargement and left atrial enlargement fa- cilitates the development of new episodes of AF or chronic AF. It has been reported that persistence or development of new electrocardiographic left ventricular hypertrophy during antihypertensive therapy was associated with an increased risk of left atrial enlargement after 3-year follow-up, and, importantly, regression of left ventricular hyper- trophy was not associated with an increased risk of left atrial enlargement.27 With these results, authors suggested that these findings provided in- sight into a potential mechanism by which chang- es in left ventricular hypertrophy were associated with changing risk of developing AF. Moreover, it has been demonstrated that left atrial diameter/ height predicts risk of cardiovascular events inde- pendent of other clinical risk factors in hyperten- sive patients with left ventricular hypertrophy.28
Finally, different neuro-hormonal systems, such as renin-angiotensin system and sympathetic sys- tems have been implied in the development of AF29,30 Structural remodeling may be the main ar- rhythmogenic substrate perpetuating AF. Fibrosis, inflammation and oxidative stress appear strongly interconnected in the pathogenesis of remodeling- induced abnormalities in AF. Although drugs that block the renin-angiotensin system do not have a direct antiarrhythmic effect, it has been observed that atrial remodeling is at least partially induced by activation of the renin-angiotensin system.29As a result, the aim of the inhibition of the renin
-angiotensin system is to limit the structural re- modeling of the atrium in AF and secondarily, if possible, to have a preventive effect on the occur- rence of AF in at-risk patients, such as those with
hypertension, heart failure or ischemic heart dis- ease.31-33 AF occurs frequently after cardiac
surgery. In this context, the inhibition of sym- pathetic system may play an important role, as the use of beta blockers has been related with an amelioration of ischemia, an anti-inflammatory effect, and inhibition of sympathetic hypertonia in this context.34 On the other hand, the sym- pathetic nerve density endocardially and epicar- dially is significantly higher in rheumatic heart disease patients with AF when compared with rheumatic heart disease patients without AF.30
Therapeutic approach in hypertensive pa-
tients to prevent new-onset atrial fibrillation
Although attaining blood pressure goals should be the first target in the whole hypertensive pop- ulation, and in this context diuretics, angioten- sin-converting enzyme inhibitors, calcium an- tagonists, angiotensin receptor antagonists, and beta-blockers have been considered suitable for initiation of antihypertensive treatment, as well as for its maintenance, in specific situations, some antihypertensive agents could provide an ex- tra benefit35 On the other hand, the effects of some of these drugs on the prevention of new- onset AF have been analyzed in different clinical scenario, not only in hypertensive population.
Several studies have reported that the preopera- tive administration of beta blockers leads to an effective modulation of severe blood pressure fluctuations and a reduction in the incidence of postoperative AF. When an AF episode occurs, although pharmacological or electrical cardiover- sion is an option, the use of intravenous digoxin, diltiazem, or beta blockers may be helpful to slow the ventricular response. In this context, digitalis is the least effective and beta blockers are the most effective for controlling the ventricular response during AF. Moreover, the use of beta blockers has been shown to accelerate the conversion of post- operative supraventricular arrhythmias to sinus rhythm compared with diltiazem.36-40 Howev- er, not all the beta blockers equally reduce the risk of AF. Thus, the incidence of post-discharge AF af- ter coronary artery bypass grafting in patients with decreased left ventricular function was lesser with bisoprolol when compared with carvedilol. 41By contrast, other studies showed that carvedilolwas superior to metoprolol in decreasing devel- opment of early postoperative AF after coronary artery bypass grafting.42,43 Moreover, in heart failure trials, carvedilol compared to metopro- lol decreased the risk of progression to AF.44
The effects of renin-angiotensin system inhibitors on prevention of new-onset AF have been specifi- cally analyzed in patients with heart failure. Thus, in TRACE (Trandolapril Cardiac Evaluation), the effects of trandolapril on the incidence of AF in patients with reduced left ventricular function sec- ondary to acute myocardial infarction was evalu- ated.45 Of the 1,749 patients included in the TRACE study, 1,577 had sinus rhythm on the elec- trocardiogram recorded at randomization. Dur- ing the 2- to 4-year follow-up period, significantly more patients developed AF in the placebo group than in the trandolapril group (5.3% versus 2.8%, respectively, P<0.05). Trandolapril significantly re- duced the risk of developing AF (RR 0.45; 95% CI,
0.26-0.76; P<0.01).45 In a retrospective analysis of the patients from the Montreal Heart Institute (MHI) included in the Studies Of Left Ventricular Dysfunction (SOLVD), after a mean follow-up of
2.9 years, 5.4% in the enalapril group and 24% in the placebo group (P<0.0001) developed AF (HR 0.22;
95% CI 0.11-0.44; P<0.0001).46 In Valsartan Heart Failure Trial (Val-HeFT), the occurrence of AF was evaluated based on adverse event reports in the patients with HF.47 During the mean 23 months of follow-up, AF was reported in 5.12% of patients allocated to valsartan and in 7.95% of those allocat- ed to placebo, p =0.0002. Valsartan treatment was independently associated with AF occurrence (HR
0.63, 95% CI 0.49-0.81).47 In the Candesartan in Heart Failure: Assessment of Reduction in Mortal- ity and Morbidity (CHARM) program, from 7,601 patients with symptomatic chronic heart failure and reduced or preserved left ventricular sys- tolic function, 6446 patients (84.8%) did not have AF on their baseline electrocardiogram. Of these,
392 (6.08%) developed AF during follow-up, 177 (5.55%) in the candesartan group and 215 (6.74%) in the placebo group (OR 0.81, 95% CI 0.66-0.99, P = 0.048). After adjustment for baseline covari- ates, the odds ratio was 0.80 (95% CI 0.65-0.99, P
= 0.039). Remarkably, there was no heterogene- ity of the effects of candesartan in preventing AF between the 3 component trials (P = 0.57).48
Another clinical scenario is the prevention of new AF episodes and the maintenance of sinus rhythm after cardioversion. In a study that included pa- tients with an episode of persistent AF for >7 days and scheduled for electrical cardioversion, two groups of patients were compared: Group I was treated with amiodarone, and Group II was treated with amiodarone plus irbesartan. The Kaplan-Meier analysis of time to first recurrence during the follow-up period (median time 254 days) showed that patients treated with irbesartan had a greater probability of remaining free of AF (79.52% versus 55.91%, P=0.007).49 In another study aimed to assess whether enalapril could im- prove cardioversion outcome and facilitate sinus rhythm maintenance after conversion of chronic AF, patients were randomly allocated to receive amiodarone or amiodarone plus enalapril 4 weeks before scheduled external cardioversion. After a median follow-up of 270 days, those allocated to enalapril showed a higher probability of remain- ing in sinus rhythm (74.3% vs 57.3%, P=0.021).50
What about hypertensive population? In patients with hypertension and permanent AF, beta block- ers and nondihydropiridine calcium antagonists (verapamil and diltiazem) remain important class- es of drugs in order to both control ventricular rate and reduce blood pressure values.17 In patients with hypertension at sinus rhythm, the first step to reduce the incidence of new-onset AF is to re- duce blood pressure values to recommended tar- gets. Several trials have tested different antihyper- tensive drugs in this setting. In CAPPP (Captopril Prevention Project), 10,985 patients aged25-66 years with a measured diastolic blood pressure
≥100 mm Hg on two occasions were randomly assigned to captopril or conventional antihyper- tensive treatment (diuretics, beta-blockers). After a mean follow-up of 6.1 years, no significant dif- ferences were found between groups in the inci- dence of new-onset AF, a secondary endpoint of the study.51 The STOP-2 (Swedish Trial in Old Patients With Hypertension-2) trial was a pro- spective, randomized trial performed in 6,614 pa- tients aged 70-80 years with hypertension (blood pressure ≥180 mm Hg systolic, ≥105 mm Hg dia- stolic, or both). Patients were randomly assigned to conventional antihypertensive therapy (ateno- lol 50 mg, metoprolol 100 mg, pindolol 5 mg, or hydrochlorothiazide 25 mg plus amiloride 2.5
mg daily) or “newer” drugs (enalapril 10 mg or lisinopril 10 mg, or felodipine 2.5 mg or isradipine
2-5 mg daily). As in STOP-2, no differences were found in the incidence of AF along the study.52
L`Allier et al. performed a retrospective, longitu- dinal cohort study from a database of 8 million people in the U.S. Hypertensive patients age ≥18 years were included if they filled a prescription for either an angiotensin-converting enzyme inhibi- tor or a calcium channel blocker. A total of 10,926 patients were analyzed. The main results of this study showed that angiotensin-converting enzyme inhibition was associated with a reduced incidence of AF for patients with hypertension in usual care setting.53 In the LIFE (Losartan Intervention For End Point Reduction in Hypertension) study, 9,193 hypertensive patients with electrocardiographic left ventricular hypertrophy were randomized to once-daily losartan- or atenolol-based antihyper- tensive therapy. A total of 8,851 patients without AF by electrocardiogram or history, were followed for 4.8 years. The main findings were that in this population, new-onset AF and associated stroke were significantly reduced by losartan- com- pared to atenolol-based antihypertensive treat- ment with similar blood pressure reduction.54
Fogari et al. evaluated the effect of losartan com- pared with amlodipine, both associated with amiodarone, in preventing the recurrence of AF in hypertensive patients with a history of recent par- oxysmal AF. After 12 months of follow-up, blood pressure values were significantly reduced by both losartan (from 151.4/95.6 to 135.5/83.7 mm Hg, P
< 0.001 versus baseline) and amlodipine (from
152.3/96.5 to 135.2/83.4 mm Hg, P < 0.001 versus
baseline), with no difference between both groups.
At least one ECG-documented episode of AF was
reported in 13% of the patients treated with losar-
tan and in 39% of the patients treated with am-
lodipine, P<0.008.55 In the VALUE (Valsartan
Antihypertensive Long-Term Use Evaluation) tri-
al, a total of 15,245 hypertensive patients at high
cardiovascular risk received valsartan 80-160 mg/
day or amlodipine 5-10 mg/day combined with
additional antihypertensive agents. During anti-
hypertensive treatment, the incidence of at least
one documented occurrence of new-onset AF was
3.67% with valsartan and 4.34% with amlodipine
(HR 0.843, 95% CI 0.713-0.997; P = 0.0455).56 In
HOPE (Heart Outcomes Prevention Evaluation),
among 8,335 high-risk participants ≥ 55 years (47% with hypertension), without known heart failure or left ventricular systolic dysfunction and fol- lowed for a median period of 4.5 years, ramipril did not significantly reduce the rate of new AF compared with placebo (2.0% vs 2.2%; OR 0.92;
95% CI 0.68-1.24; P = 0.57).57 In the ONTARGET (Ongoing Telmisartan Alone and in Combination With Ramipril Global Endpoint Trial) study, which included more than 25,000 patients who had vas- cular disease or high-risk diabetes without heart failure (69% with hypertension), the incidence of new-onset AF, a predefined secondary endpoint, was similar in patients treated with ramipril (6.9%) and telmisartan (6.7%).58 In the TRANSCEND (Telmisartan Randomized Assessment Study in ACE Intolerant Subjects With Cardiovascular Dis- ease) trial including patients with vascular disease or high-risk diabetes without heart failure, intol- erant to angiotensin-converting enzyme inhibi- tors 76% of them with hypertension, no significant differences were found between telmisartan and placebo in the incidence of new-onset AF.59 The GISSI-AF (Gruppo Italiano per lo Studio Della So- pravvivenza Nell’Infarto Miocardico–Atrial Fibril- lation) study was a large, randomized, prospec- tive, placebo-controlled, multicenter trial aimed to test whether valsartan could reduce the recur- rence of AF in patients with underlying cardiovas- cular disease, diabetes, or left atrial enlargement (85% had hypertension) and who were in sinus rhythm but had had either ≥2 documented epi- sodes of AF in the previous 6 months or success- ful cardioversion for AF in the previous 2 weeks. A total of 1,442 patients were enrolled in the study. AF recurred in 51.4% of patients treated with val- sartan group and in 52.1% of patients treated with placebo (HR 0.97; 95% CI 0.83-1.14; P=0.73).60
In another study aimed to determine the relative risk for incident AF among hypertensive patients who received antihypertensive drugs from dif- ferent classes, 4,661 patients with AF and 18,642 matched control participants from a population of 682,993 patients treated for hypertension were included for the analysis. Patients with clini- cal risk factors for AF were excluded. Long-term therapy with angiotensin-converting enzyme in- hibitors (OR 0.75; 95% CI 0.65-0.87), angiotensin II-receptor blockers (OR 0.71; 95% CI 0.57-0.89), or beta-blockers (OR 0.78; 95% CI 0.67-0.92) was associated with a lower risk for AF than current
exclusive therapy with calcium channel blockers.61 A population-based case-control study aimed to determine whether antihypertensive treatment with angiotensin-converting enzyme inhibitors/ angiotensin II-receptor blockers or beta-blockers, compared with diuretics, was associated with the risk of incident AF in a community practice set- ting, showed that single-drug users of angioten- sin-converting enzyme inhibitors/ angiotensin II- receptor blockers had a lower risk of incident AF compared with single-drug users of a diuretic (OR
0.63; 95% CI 0.44-0.91), while single-drug use of beta-blockers was not significantly associated with lower AF risk (OR 1.05; 95% CI 0.73-1.52). Also, none of the most commonly used two-drug regi- mens was significantly associated with AF risk, in comparison with single-drug use of diuretic.62
A number of meta-analyses have studied the ef- fects of renin-angiotensin system inhibition on the prevention of new-onset AF.63-65 Healey et al. analyzed a total of 11 studies, which included
56,308 patients: 4 in heart failure, 3 in hyperten- sion, 2 in patients following cardioversion for AF, and 2 in patients following myocardial infarc- tion. Overall, renin-angiotensin system inhibi- tors reduced the relative risk of AF by 28% (95% CI 15%-40%, p = 0.0002). Reduction in AF was similar between angiotensin converting enzyme inhibitors and angiotensin receptor blockers and was greatest in patients with heart failure (rela- tive risk reduction 44%, p = 0.007). Despite there was no significant reduction in AF in the overall hypertensive population (relative risk reduction
12%, p = 0.4), in patients with hypertension and left ventricular hypertrophy there was a significant reduction of 29%.63 Schneider et al. analyzed a total of 23 randomized controlled trials with 87,048 patients. Overall, renin-angiotensin system inhibi- tors reduced AF by 33% (p < 0.00001), but there
was substantial heterogeneity among trials. In pri- mary prevention, renin-angiotensin system inhi- bition was effective in patients with heart failure and those with hypertension and left ventricular hypertrophy but not in post-myocardial infarction patients. In secondary prevention, renin-angioten- sin system inhibitors were often administered in addition to antiarrhythmic drugs, including ami- odarone, further reducing the odds for AF recur- rence after cardioversion by 45% (p = 0.01) and in patients on medical therapy by 63% (p < 0.00001) (Table 2).64 More recently, Huang et al. analyzed
21 clinical trials including 91,381 patients and 5,730
AF events. Renin-angiotensin system inhibitors
reduced the relative risk of AF by 25% (primary
prevention by 24% and secondary prevention by
27%). Relative risk reduction was 0.71 in patients
with hypertension (95%CI: 0.54-0.92), 0.58 in pa-
tients with chronic heart failure (95%CI: 0.39-0.87)
and 0.71 in those with AF (95%CI: 0.52-0.96).
Table 2. Effects of renin-angiotensin system inhibitors (angiotensin-converting enzyme inhibitors and angiotensin receptor antagonists) on occurrence of AF (adapted from 64).
| Clinical Situation |
Odds Ratio |
95%CI |
| Hypertension (overall) |
0.89 |
0.75-1.05 |
| Hypertension (LVH) |
0.65 |
0.52-0.80 |
| Heart Failure |
0.52 |
0.31-0.87 |
| Postmyocardial Infarction |
0.72 |
0.41-1.27 |
| Postcardioversion |
0.55 |
0.34-0.89 |
Aliskiren is the first oral direct renin inhibitor available, and its current licensed indication is es- sential hypertension. Although no clinical trials have specifically analyzed the effects of aliskiren on the prevention of new-onset AF, experimen- tal data have reported that aliskiren may have anti-arrhythmic and anti-heart failure properties . A cross-sectional survey has recently suggested that aliskiren might reduce the risk of developing permanent AF in patients with par- oxysmal or persistent AF.9 On the other hand, it has been suggested that agents with anti-aldo- sterone properties should be the preferred diuret- ics for reducing hypertension related AF.






