The 894G Allele of the Endothelial Nitric Oxide Synthase 3 (eNOS) is Associated with Atrial Fibrillation in Chronic Systolic Heart Failure
Fuad Fares PhDa, Yoav Smith PhDb, Naiel Azzam PhDa, Barak Zafrir,MDc,d, Basil S. Lewis, MD, FRCPd, Offer Amir, MDc,d
aDepartment of Human Biology, Faculty of Natural Sciences, University of Haifa and Department of Molecular Genetics, Carmel Medical Center, Haifa, Israel.bGenomic Data Analysis Unit, Hadassah Medical School, Hebrew University of Jerusalem, Israel,.c Department of Cardiovascular Medicine, Lady Davis Carmel Medical Center, and Ruth and Bruce Rappaport School of Medicine, Technion‒Israel Institute of Technology, Haifa, Israel,.4 Heart Failure Center, Lin Medical Center, Haifa, Israel.
Background: Atrial fibrillation (AF) in patients with heart failure signals poor prognosis. The endothelial nitric oxide synthase (eNOS) enzyme is a key player in the counterregulation of oxidative stress, which is related in part to AF pathogenesis. The purpose of this study was to investigate a possible clinical association in heart failure patients between the presence of exon 7 G894T eNOS polymorphism, known to result in the Glu298Asp protein variant, and the occurrence of AF.
Methods: We analyzed the DNA of 344 patients with chronic systolic heart failure for exon 7 G894T eNOS polymorphism, using PCR. Odds ratios for AF were calculated for the homo- and heterozygous G-allele G894T variants relative to the TT variant.
Results: Of the 344 patients, 204 (59%) were homozygous for the G allele, 122 (36%) were heterozygous (GT), and 18 (5%) were homozygous for the T allele. AF episodes were documented in 73 patients (36%) with the GG genotype, in 35 (29%) with GT, and in 2 (11%) with TT. The odds ratio for AF, based on the presence of at least one G allele in the eNOS 894 gene, was 3.96 (95% confidence interval, 1.17‒13.56, p=0.04). Having two G alleles increased the odds ratio to 4.5 (95% confidence interval, 1.0‒20.0, p=0.02).
Conclusion: Patients with systolic heart failure demonstrate strong correlation between AF and the presence of a G allele in the exon 7 G894T eNOS genotype. These findings support the importance of eNOS polymorphism in the pathogenesis of AF in heart failure patients.
Correspondence to: Offer Amir, MD, Heart Failure Center, Cardiology Department, Lady Davis Carmel Medical Center, 7 Michal St, 34362 Haifa, Israel.
Inflammation and oxidative stress are known are known concomitants of heart failure (HF).1–3 The vascular endothelium uses a sophisticated system of enzymes that enrich local nitric oxide and serves as a protective mechanism against oxidative stress. Endothelial dysfunction, which may occur due to reduced NO bioavailability or increased endothelial NO synthase (eNOS)-dependent superoxide formation or both, predisposes the individual to major cardiovascular pathology.4,5 NOS, a key player in the counterregulation of oxidative stress, is one of the principal enzymes in the vascular endothelium because its products participate in the formation and degradation of NO. Accordingly, elucidation of the role of eNOS genetic polymorphism is of major clinical interest.6,7
Several eNOS genomic polymorphisms at different sites of the genomic code have been described in association with various pathological myocardial and vascular conditions, including T (786)C in the promoter, a variable number of tandem 27-base pair repeats in intron 4, and G894T in exon.7,8–11The clinical significance of exon 7 G894T eNOS polymorphism for coronary artery disease and HF has been assessed in several studies, with conflicting findings.12–14
HF and atrial fibrillation (AF) are notoriously related, as HF is a predisposing risk factor for AF and the latter is associated with high mortality.15,16 Accordingly, significant research efforts have been invested in improving our understanding of the interface between these two conditions. The impact of genetic polymorphisms on AF in HF patients has been previously studied in several reports.17
A possible relationship between eNOS polymorphism and AF has been described only in very few reports, and even in those the findings were inconsistent. One group reported the existence of such an association, but this was not confirmed by others.18,19 Accordingly, the purpose of the present study was to analyze the clinical association between exon 7 G894T eNOS (rs 57135373) polymorphism and AF in patients with chronic systolic HF.
The study population comprised 344 patients who were followed at our HF out-patients center due to chronic systolic HF, defined as HF syndrome persisting for more than 3 months and left ventricular ejection fraction (LVEF) of less than 40%. Blood samples were taken from each patient and their DNA was analyzed for the presence of exon 7 G894T eNOS polymorphism. In addition, 96 healthy subjects who were ethnically matched to the patient group underwent similar analysis for the presence of the polymorphism and served as a control group.
Each patient underwent a full medical examination, including detailed anamnesis, echocardiography, Holter recording, and serial 12-lead electrocardiography. Diagnosis of AF (paroxysmal, persistent, or chronic) was based on documentation of the arrhythmia by a senior cardiologist who reviewed the electrocardiograms or the Holter recordings or both, and was blinded to the results of the patients’ genetic analyses. The patients’ clinical characteristics are listed in Table 1.
The study was approved by the Institution Review Board (Helsinki Committee) of Lady Davis Carmel Medical Center. All patients signed their informed consent to participate.
Table 1. Baseline Patient Characteristics
| Variable |
Patient group, no.(%) (n = 344) |
Mean ± SD |
| Age (years) |
|
64 ± 13.2 |
| Body mass index (kg/m2) |
|
28.4 ± 5.3 |
| LVEF (%) |
|
25.1 ± 7.1 |
| LVEDD (cm) |
|
6.1 ± 0.8 |
| Left atrial dimension |
|
4.5 ± 0.6 |
| Hemoglobin (g/dl) |
|
12.5 ± 1.7 |
| Creatinine (mg/dl) |
|
1.3 ± 0.6 |
| NYHA grade |
|
2.7 ± 0.9 |
| Male gender |
284 (83%) |
|
| H/O myocardial infarction |
204 (59%) |
|
| Hypertension |
193 (56%) |
|
| Diabetes mellitus |
148 (43%) |
|
| Atrial fibrillation |
110 (32%) |
|
| ACEI / ARB |
312 (91%) |
|
| Spironolactone |
102 (30%) |
|
| Beta blockers |
330 (96%) |
|
| ICD/CRT |
144 (42%) |
|
LVEF = left ventricular ejection fraction; LVEDD = left ventricular end diastolic dimension; NYHA = New York Heart Association; ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; ICD = implantable cardioverter defibrillator; CRT = cardiac resynchronization therapy
Genomic DNA was extracted from whole blood leukocytes using the High Pure PCR Template Preparation Kit (Roche, Mannheim, Germany).Extracted DNA was stored at ‒20oC. Substitution of the amino acid Asp for Glu298 was detected by PCR, using 500 ng of genomic DNA as a template, with the following primers: forward, 5`- GTG GTC ACG GAG ACC CAG CCA ATG AGG -3`; reverse, 5`- CCA GCG CAG GCC CAG GGC TGC AAA CCA -3`. The conditions used for PCR (Eppendorf Thermocycler, Hamburg, Germany) were as follows: (pre-denaturation) at 94°C for 3 min, followed by 30 repeated cycles of denaturation at 94°C for 1 min, annealing at 63°C for 1 min, extension of 45 s at 72°C, and finally extension of 10 min at 72°C. PCR products were analyzed by DNA sequencing using the sequencing services of Hylabs Laboratories, Rehovot, Israel
A computer program written in MATLAB(r2011a) scanned the input data columns and tabulated the allele and genotype frequencies (GG, GT, TT) in exon 7 G894T eNOS polymorphism in relation to documented episodes of AF.
The generic allele distributions in patients with AF, as well as hetero-, homo-, and serological odds ratios, were all calculated.20 The 95% confidence intervals (CI) for the odds ratios were determined.21 Fisher’s exact test was calculated using SISA (Simple Interactive Statistical Analsis). Chi square and Hardy-Weinberg equilibria were calculated using standard equations.22 A pvalue of <0.05 was considered statistically significant.
Of the 344 HF patients, 204 (59%) were homozygous for the G allele of the exon 7 G894T eNOS 894 genotype, 122 (36%) were heterozygous (GT), and 18 (5%) were homozygous for the T allele. Of the 96 healthy control subjects, 42 (44%) were homozygous for the G allele, 46 (48%) were heterozygous (GT) and 8 (8%) were homozygous for the T allele Table 2..
There was no deviation from Hardy-Weinberg equilibrium in either the patient group (frequency of T/G alleles, 0.23/0.77; expected % genotype frequencies for TT/GT/GG, 5/36/59; χ2 = 0.0, p = 0.99) or the control group (frequency of T/G alleles, 0.32/0.68; expected % genotype frequencies for TT/GT/GG, 8/48/44; χ2 = 0.45, p = 0.79). Allele and genotype frequencies from the Single Nucleotide Polymorphism Database (dbSNP), using data for HapMAP CEU and CEPH samples as well as for Caucasian or European groups, show similarities to our healthy control group. Furthermore, the prevalence of the GG subtype in our control group was similar to that reported for other healthy populations.23 Allele frequencies did not differ between patients and controls (p=0.15; Table 2). However, the two groups differed significantly with respect to the distribution of eNOS genotype subtypes (p= 0.02; Table 2).
The proportions of patients suffering from AF differed significantly between the different eNOS subtypes. Episodes of AF were documented in 73 patients (36%) with the GG genotype, in 35 (29%) with the GT subtype, and in 2 (11%) with the TT genotype subtype. Compared to those with the TT subtype, a significant proportion of HF patients with at least one G allele had experienced AF episodes (χ2= 3.80, p = 0.03; Table 3, Fig. 1).
Figure 1.
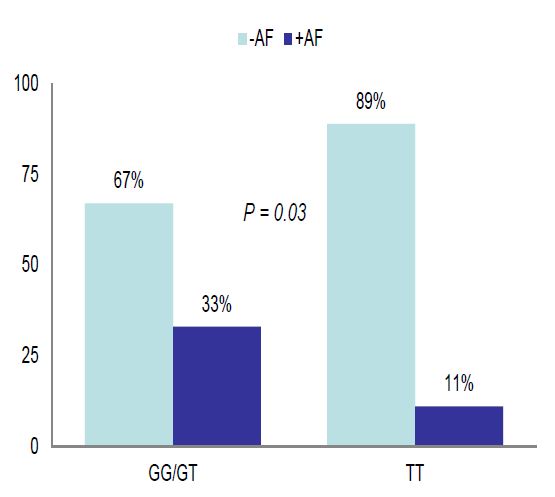
Prevalence of Atrial Fibrillation in Chronic Systolic Heart Failure Patients in Relation to the Presence or Absence of the G allele in 7 G894T eNOS Polymorphism {GG/GT vs. TT}
Table 2. Distribution of eNOS G894T Genotype in Patients and Controls
| eNOS-894T/G Genotype |
Number (%) |
p Value |
Allele Frequency f (T)/f(G) |
p Value |
|
TT |
TG |
GG |
|
|
|
| Patients (n = 344) |
18(5) |
122(36) |
204(59) |
0.02 (χ2 = 7.52) |
0.23/0.77 |
0.15 (χ2 = 2.03) |
| Controls (n = 96) |
8(8) |
46(48) |
42(44) |
0.32/0.68 |
|
AF = atrial fibrillation
Table 3. Frequency of Atrial Fibrillation in Heart Failure Patients According to eNOS Genotype
| eNOS Genotype (n) |
Patients with AF n (%) |
Patients without AF n (%) |
p Value |
| TT (18) |
2 (11) |
16 (89) |
0.03 |
| GT/GG (326) |
108(33) |
218 (67) |
χ2 = 3.80 |
AF = atrial fibrillation
The odds ratio for AF based on the presence of at least one G allele of the eNOS 894 genotype as compared to the TT genotype was 3.96 (95% confidence interval, 1.17‒13.56, p=0.04). Having two G alleles at this position of the eNOS gene increased the odds ratio to 4.5 (95% CI = 1.0‒20, p=0.02). A comparison of the GG/GT and TT allelic subtypes of the HF patients for several other clinical parameters known to be associated with AF yielded no significant differences between them (Table 4).
Table 4. Patient Characteristics According to Prevalence of the G/T Alleles
| Variable |
GG/GT (n = 326) |
TT (n = 18) |
P value |
| Age (years)* |
64.2 ± 13.2 |
59.6 ± 12.1 |
0.15 |
| Gender (Male) |
267 (82%) |
17 (94%) |
0.59 |
| LVEF (%)* |
25.1 ± 7.1 |
24.6 ± 6.6 |
0.73 |
| LVEDD (cm)* |
6.1 ± 0.8 |
6.1 ± 0.9 |
0.92 |
| H/O Hypertension |
183 (56%) |
10 (55%) |
0.96 |
| H/O Diabetes Mellitus |
141 (43%) |
7 (39%) |
0.81 |
| Left Atrial Dimension (cm)* |
4.51±0.59 |
4.43±0.47 |
0.55 |
| Ischemic Etiology |
211 (65%) |
10 (55%) |
0.45 |
| Beta Blockers |
313 (96%) |
17 (94%) |
0.51 |
| ACEI or ARB |
296 (91%) |
16 (89%) |
0.68 |
| Spironolactone |
97 (30%) |
5 (28%) |
0.42 |
| NYHA Grade > 3 |
178 (54%) |
10 (55%) |
0.94 |
| Mortality |
99 (30%) |
6 (33%) |
0.79 |
*Mean ± SD. LVEF=left ventricular ejection fraction; LVEDD = left ventricular end diastolic dimension; ACEI = angiotensin-converting enzyme inhibitor; ARB = angiotensin receptor blocker; NYHA = New York Heart Association.
Using a computer program written in MATLAB (r2011b), we performed multiple linear regression analysis of the relationships between the following parameters and the presence of AF: age above the group median age of 54 years, LVEF less thanthe group median value of 30%, male gender, advanced-stage HF (NYHA class III or IV), and the presence of a G allele (GG/GT polymorphism). The coefficient estimate for the multilinear regression analysis was highest for the presence of a G allele (0.18; 95% confidence intervals for the coefficient estimates:-0.05-0.4), followed in order by older age (0.15; 95% confidence intervals for the coefficient estimates: 0.03-0.2), advanced NYHA class (0.11; 95% confidence intervals for the coefficient estimates: 0.11-0.2), male gender (0.06; 95% confidence intervals for the coefficient estimates: 0.07-0.1) , and low LVEF (0.01; 95% confidence intervals for the coefficient estimates: -0.15-0.1).
The main finding of our study was that chronic systolic HF patients who carry a G allele subtype of the exon 7 G894T (eNOS7) polymorphism have significantly higher rates of atrial fibrillation episodes than HF patients with the T allele. In HF patients with both G alleles, the relative risk for developing AF is up to 4.5 times higher than that in HF patients with the TT subtype. This finding was supported by our regression analysis, which identified the presence of a G allele as the predominant parameter associated with AF,even when compared to other well-known AF-related clinical parameters such as older age, advanced NYHA class, male gender and low LVEF.
It is important to note that the prevalence of the GG subtype in our control population of ethnically matched healthy subjects was similar to that reported in healthy populations.23 Moreover, although the G-allele frequency in the HF patients and the controls was similar, the genotype distribution in the HF group differed significantly from its distribution in the control group, in that the GG subtype was significantly more prevalent than the TT subtype in the HF group but not in the control group.
The effect of eNOS7 polymorphism on cardiovascular diseases remains unclear.24–26 Relatively few studies have investigated the presence of exon 7 G894T eNOS polymorphism in HF populations. Interestingly, a recent analysis of the genomic DNA isolated from myocardial tissue samples showed no detectable change in either eNOS mRNA or protein expression associated with exon 7 G894T eNOS polymorphism.27 In the A-HeFT trial, the presence of exon 7 G894T eNOS polymorphism in Afro-American HF patients was associated with a better treatment response outcome. Other authors, however, have suggested that this polymorphism is associated with poorer prognosis in HF patients, particularly inpatients with non-ischemic cardiomyopathy.13,14
The relationship between exon 7 G894T eNOS polymorphism and AF has been investigated in very few studies.19,28 In two of them, no association was found between this polymorphism and AF.19,28 consistently with our present findings. Nevertheless, several important differences between those three studies and our work should be noted. Two did not evaluate HF patients at all,19,28 and in the third study, which did ,18 the prevalence of AF was only 15%, which is well below the reported prevalence of AF in advanced HF.15,16 The low prevalence might be explained by the fact that AF diagnosis in that study was based on a single electrocardiogram at enrolment. In our study, in contrast, diagnosis of AF was based on reviews of several electrocardiograms as well as on Holter recordings in each patient. Another major difference was the reduced rate of beta-blocker usage (23%) in the study of Bedi et al.,18 which was significantly lower even than that of the non-AF HF patients in the same study (p=0.003). This dosage regime, which may reflect changes in treatment guidelines, inevitably interferes with realistic evaluation of AF prevalence. We believe that a more accurate reflection of the actual situation in HF populations is provided by our study, in which the prevalence of AF in the HF patient group was estimated at 32%, the large majority (96%) of HF patients was on beta blockers, and yet exon 7 G894T eNOS polymorphism was found to be strongly associated with AF.
Atrial fibrillation is mediated through atrial electrical and mechanical remodeling, and there is increasing recognition of the role of oxidative stress in this process.29 Nitric oxide is traditionally considered to play a defensive role in the vascular endothelium and to protect organs from oxidative stress. However, the nitric-oxide/oxidative-stress balance system is complex. For example, when eNOS is deprived of its critical cofactor tetrahydrobiopterin or its substrate L-arginine, it may produce large amounts of reactive oxygen species such as peroxynitrite rather than NO, leadJournaling to NOS uncoupling and causing tissue damage that facilitates pathological remodeling of the myocardium.30,31 Moreover, certain manipulations of NOS2 in an animal model of HF have been shown to promote the propensity to develop AF.32
The G894T polymorphism in exon 7 of the eNOS gene leads to an amino acid change from glutamate to aspartate at position 298 on the eNOS protein (Glu298Asp). Because the biological effects of this change are still obscure, the functional significance of this single-nucleotide polymorphism remains controversial. Homozygosity for the Asp298 variant was suggested to increase susceptibility to proteolytic cleavage, which can lead to reduced enzyme activity and decreased production of NO.33 However, others have found that in the presence of the Asp298 variant the NO production and enzyme activities remain unchanged, leading them to conclude that intracellular cleavage mechanisms are unlikely to account for associations between the eNOS7 polymorphism and cardiovascular diseases.34 Thus, we still lack a clear understanding of the clinical significance of these two eNOS protein variants, glutamate or aspartate, at position 298. We suggest that in patients with HF, the combined presence of the GG polymorphism (which results in glutamine at position 298 of the eNOS protein) and elevated oxidative stress may facilitate eNOS uncoupling, with increased production of reactive oxygen species predisposing to AF.We believe that this hypothesis is worth testing in future studies and future functional assays are required to complement this data.
Our study has certain limitations. First, although our data were recorded blindly with respect to the genotype analysis, the study analysis of AF episodes was retrospective. Secondly, the association observed here between AF and exon 7 eNOS polymorphism may have been influenced by other genetic ethnic factors specific to our cohort of patients. Thirdly, although our population respects the Hardy Weinberg equilibrium, the TT group was relatively small.
The data derived here from patients with chronic systolic HF support an association between the G allele in exon 7 G894T eNOS polymorphism and AF. The GG subtype that we found to be to be significantly associated with AF was also significantly more prevalent than the TT subtype in our group of HF patients than in the control group. A better understanding of the triad of NO, oxidative stress, and the biological change that results from Glu298Asp polymorphism in the eNOS protein is likely to shed more light on the implications of this genetic polymorphism for AF in HF patients.
The study was supported by a grant from the NOFAR Program for Applied Academic Research in Biotechnology and Nanotechnology, Office of the Chief Scientist, Ministry of Industry, Israel.
Dr Smith and Dr Azzam were paid for their working hours.
No Disclosures for other authors.






