QT Prolongation Following Ectopic Beats: Initial
Data Regarding The Upper Limit Of Normal With Possible Implications For Antiarrhythmic Therapy And Concealed (Unexpressed) Long QT
Alyssa J. Reiffel, MD, James A. Reiffel, MD
The Division of Cardiology, Department of Medicine,Columbia University Medical Center,New York, New York.
Ectopic beats are frequently associated with morphologic repolarization alterations of ensuing sinus beats. Less is known about repolarization duration alterations of post-ectopic sinus beats. In one patient who developed long QT and torsades de pointes upon exposure to a class III antiarrhythmic drug, and was later genotyped as being a carrier for long QT syndrome (LQTS) type 1, review of a pre-drug Holter monitor study revealed marked QT prolongation of post-ectopic sinus beats. In wondering whether this might be a common clue to “concealed” unexpressed LQTS, we realized that we must first characterize the range of post-ectopic QT prolongation present in normals. Prolongation beyond the upper limit of this range might then raise suspicion of possible LQTS and alter the antiarrhythmic drug selection process for the suppression of atrial fibrillation or other arrhythmias.
Accordingly, we assessed the presence/degree of repolarization prolongation following premature ectopic impulses in 166 subjects with normal conduction intervals and normal repolarization on their resting 12-lead ECG, 75 of whom had no known associated cardiovascular disorder of any kind. That is, in our subjects, the maximal prolongation of the QT interval of the sinus beat following isolated ventricular and atrial premature complexes was characterized.
QT prolongation is common in post ectopic sinus beats. However, in our subjects the uncorrected QT interval of post-ectopic sinus beats never exceeded 480 ms in duration [which was much shorter than that seen (510-590 ms) in our gene carrier]. Conclusions: The QT interval in normal subjects may prolong following premature complexes but not to a value in excess of 480 ms.
Correspondence to: James A. Reiffel,161 Fort Washington Avenue,New York, New York 10032.
The long QT Syndrome (LQTS) results from a family of genetic ion-channel disorders that cause prolongation of the QT interval with an associated risk of developing polymorphic ventricular tachycardia of the torsades de pointes (TdP) variety, with possible syncope or death. Due to its variable severity and penetrance, LQTS is difficult to diagnose, as 5-10% of those with an LQTS gene do not present with a prolonged QT interval on their resting ECG,1 while others can have only mild to marked, or variable to persistent QT prolongation. This disorder may present with TdP upon a challenge, such as drug administration.2 Such TdP developed in one female patient we encountered who had a maximal QT of 450 ms on several 12 lead ECGs prior to therapy yet suffered TdP upon exposure to a class III AAD. Notably, we noted marked post-ectopic QT prolongation upon postevent review of a Holter monitor study she had done previous to therapy. The risk of such a cardiac event increases exponentially with QT length.3 Although there are specific diagnostic criteria for LQTS, the condition often evades diagnosis. This occurs for several reasons: First, the rate-corrected QT interval (QTc) of an individual may be variable over time and varies with electrolyte status and with heart rate and autonomic state.4 Such long-term variation, even in healthy patients, has not yet been fully quantified. Second, routine prolonged ambulatory ECG recordings display only a limited number of leads for analysis and they only rarely display asymptomatic TdP.3 Finally, genetic screening is prohibitively expensive and impractical on a widespread basis. Therefore, a simpler marker for this disease when sub-clinical would be advantageous.
Premature ectopic beats often cause altered repolarization of the next sinus beat, primarily morphologic. These have been assessed by Holter monitoring in normals and in subjects with LQTS where potentially diagnostic differences have been noted.5 Additionally, Vecchietti et al. have reported that ventricular ectopic beats may induce QT prolongation of the ensuing sinus beat.6 However, to our knowledge, the degree to which QT prolongation may be seen in post-ectopic sinus beats has not yet been studied. Because QT prolongation may occur following ectopic beats, as we noted in our one LQTS carrier, we postulated that such prolongation might be longer in many/most patients prone to not yet manifest long QT syndrome. To determine if this is the case, we realized that we first had to characterize the behavior of post ectopy QT prolongation in individuals without QT prolongation in their 12-lead ECG so as to establish a normal range prior to attempting to assess its behavior in long QT gene families. As such, for this report, we chose to study and characterize the normal population for the presence and extent of post-ectopic QT prolongation.
To establish the spectrum of post ectopy repolarization duration in normals, we examined 166 patients by 24-hour ambulatory (Holter) monitoring. All were without signs of LQTS by standard electrocardiography and without known clinically significant ventricular tachyarrhythmias. They were selected at random from those who came to the Holter laboratory for a 24-hour recording as part of their evaluation of non-specific symptoms such as palpitations, dizzy spells, and the like. Each subject had entirely normal conduction and repolarization during sinus rhythm. Mean age was 54 and ranged from 21 to 86 years. One hundred seventeen were women. Underlying cardiovascular diagnoses obtained by review of the subject’s clinical records included: hypertension, left ventricular hypertrophy, congestive heart failure, hyperlipidemia, aortic valve disorder, mitral valve disorder, valve replacement, hypercholesterolemia and rheumatic mitral insufficiency. Seventy-five patients were without any underlying cardiovascular disease. Patient identities were protected by assigning code numbers to patients in accordance with HIPAA regulations. Institutional Review Board approval was received prior to the collection of this information.
For each patient, several intervals surrounding multiple supraventricular and ventricular ectopic beats were measured. The RR and QT intervals were measured for: (a) sinus cycles preceding all ectopic beats (RR, QT); (b) all ectopic beats (RR’ [the coupling interval], QT’); and (c) the sinus beat immediately following all ectopic beats (R’R”, QT”) (Figure 1). Corrected QT intervals were calculated by Bazett’s formula: QTc, QTc”. The data was sorted into two groups according to the origin of the ectopic beat: ventricular or supraventricular. The ratio RR’/RR was used as an indicator of the relative prematurity of the ectopic beat. Postectopic QT intervals, QT”, were normalized for baseline QT with the ratio QT”/QT. All trend lines were calculated with Microsoft Excel 2003 SP2 using a linear least-squares fit. Mean (+/- standard deviation) changes for QT” and common statistical analyses related to such were not calculated for this study as: (a) we were assessing only the upper boundary of QT”, and (b) mean (+/- standard deviation) would be influenced by preceding sinus cycle length and the coupling interval of the ectopic complex which we noted could vary in the same patient over the 24 hour recording and certainly varied among patients (see below). Upon completion of this study, one additional subject was studied in an identical manner: she is a known LQTS type 1 gene carrier.
Figure 1. Intervals measured: RR, RR’, R’R”, QT, QT’, QT”
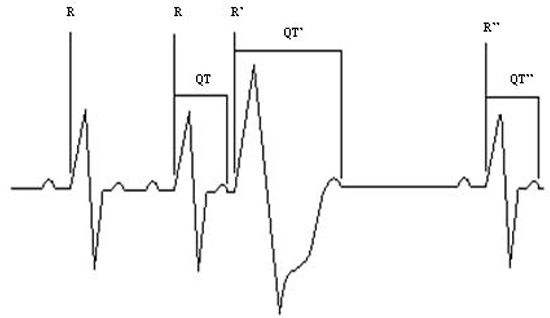
The data revealed the following (Figures 2-5): The QT interval of the post-ectopic beat commonly increases following ventricular or supraventricular ectopic beats. The amount of the increase in QT is variable among patients and in a single patient during a 24-hour cycle. The change in QT duration, compared with the sinus beat immediately preceding the ectopic beat, ranged from a 40 ms decrease to a 100 ms increase following supraventricular premature depolarizations and a 40 ms decrease to a 140 ms increase following ventricular premature depolarizations across our 166 patients. When normalized for baseline QT, the percent change ranged from an 11% decrease to a 27% increase following supraventricular premature depolarizations and an 11% decrease to a 41% increase following ventricular depolarizations. The amount of variability within a single patient ranged from 0 to 120 ms (0 to 27%) following supraventricular ectopic beats and from 0 to 150 ms (0 to 35%) following ventricular ectopic beats, when at least 3 ectopic beats of either respective origin were present during the Holter recording. In this group of normals, the post-ectopic QT never exceeded 480 ms after either supraventricular or ventricular ectopic impulses (Figures 2,4). In contrast, in the one gene carrier of LQTS type 1 described above, in whom the longest QT in sinus rhythm was 450 ms, post ectopic QT intervals ranged from 510-590 ms (Figure 5).
Figure 2. The post-ectopic QT interval, QT”, as a function of the coupling interval, RR’
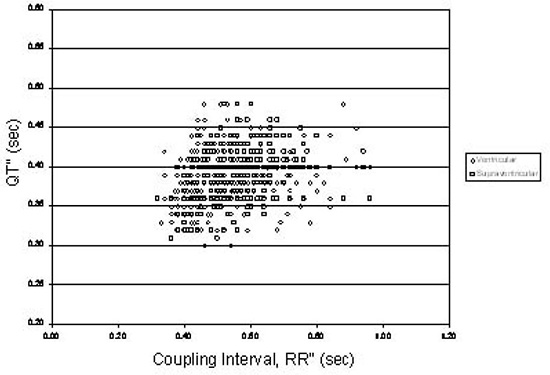
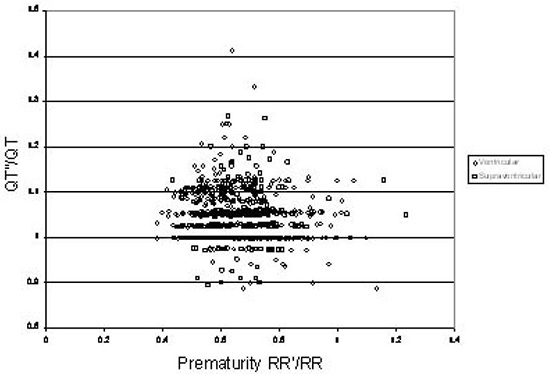
Figure 3. The ratio of the post-ectopic QT interval, QT”, to the QT interval of the last sinus beat before the ectopic beat, QT, as a function of the relative prematurity of the ectopic beat, RR’/RR
The above results clearly indicate that following an ectopic beat, whether supraventricular or ventricular in origin, the next sinus beat may reveal prolongation of repolarization, rather than just morphological alteration. It is also clear that within and among patients in our series without clinically recognized LQTS, the prolongation of repolarization following a post-ectopic beat can be variable but is finite. In addition, the duration of post-ectopic repolarization can be longer than the 440-450 ms limit usually applied as the upper limit of the normal QTc interval on the resting 12 lead ECG during sinus rhythm. Notably, however, in our subjects with normal resting ECGs and no history of LQTS, it never exceeded 480 ms in normals.
Figure 4. The post-ectopic QT interval, QT”, as a function of the pause length, R’R”
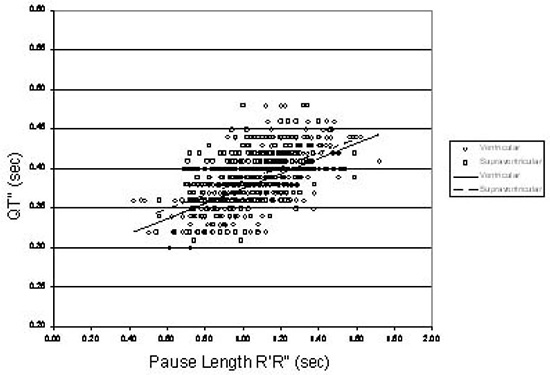
As one can see in more detail in Figure 2, both types of ectopy (ventricular and supraventricular) produce relatively similar behavior. In both groups, QT” decreased as the coupling interval decreased, although for any given coupling interval, QT” tended to be shorter after ventricular ectopic beats than after supraventricular ones. This is consistent with the potential repolarization shortening effect associated with wide QRS complexes previously described by Banker et al.7Figure 3 shows that in normals, there is virtually no difference between QT interval behavior after ventricular and supraventricular ectopic beats when corrected for baseline QT with the ratio QT”/QT. The shortening effect mentioned above is lost when intervals are normalized in this way. Figure 4, which displays QT” as a function of R’R” (the pause following the ectopic beat) shows the 480 ms demarcation line to appear enhanced. If LQTS gene-carriers and patients demonstrate different behavior (i.e., post-ectopic QT intervals greater than 480 ms), such a demarcation line may prove to be diagnostically useful and could be used to identify LQTS prone patients.
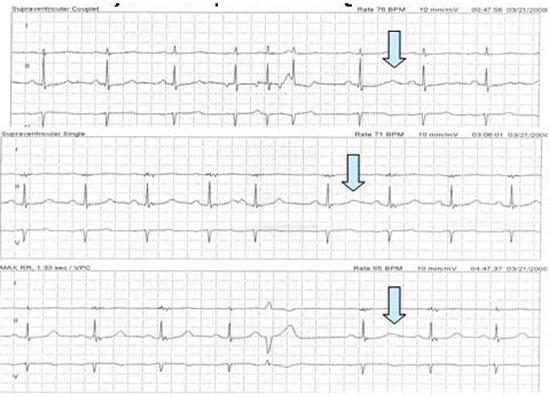
Figure 5. Rhythm strips (from Holter monitoring) in a LQTS carrier demonstrating a greater prolongation of the post-ectopic QT interval
There is an inherent limitation in the use of the coupling interval RR’ when comparing QT lengths at differing heart rates. It is largely the interval between the ectopic and the post-ectopic beat, the pause, which affects the subsequent QT interval. Both the sinus rate before and the origin of the ectopic beat determine the length of this pause. A coupling interval may be identical for two ectopic beats in two different patients or even for two ectopic beats within the same patient, after two very different sinus rates. The pause after these ectopic beats would be longer in the patient with the slower sinus rate because the ectopic beat would be more premature and the intrinsic sinus rate slower. This would elicit a post-ectopic beat with a longer QT interval than would be elicited in a patient with a faster initial sinus rate. Such variation renders comparisons between QT interval lengths at different coupling intervals potentially more difficult to interpret. This limitation also leads to difficulty using the relative prematurity RR’/RR in comparisons. Trends in QT length when compared against the coupling interval do not necessarily hold when compared against RR’/RR due to the fact that all QT lengths were measured at different heart rates and leads to the division of the coupling interval by a nonconstant function essentially random in nature. This potentially masks any previously existing relationships. We found that in addition to using the raw data, the most meaningful way to compare QT lengths was against R’R”, the pause length. Notably, the common way to compare or “correct” QT intervals so as to make inter-patient or intercondition comparisons, as by the application of Bazett’s or other common correction formulae to QT,” is not applicable to our data analysis because these calculations assume stable sinus rhythm rather than a post-ectopic beat and cannot take into account the relative prematurity of the ectopic beats.
Beyond the above, and most notably, we do not know how representative our one gene carrier is of the overall population of LQTS carriers. We have not yet completed studies in other gene carriers in our center and there are no analyses similar to ours in such patients in the literature. Thus, additional studies will be required to truly characterize this population as contrast to our normal subjects.
This study examined QT prolongation after ectopic beats in many ways, including as raw data, as a function of prematurity, normalized for baseline QT, and by utilizing a correction formula. In our series of patients without LQTS, post-ectopic intervals greater than 480 ms were not noted. In our one LQTS gene carrier, values of 510 ms and longer were noted. While it is clear that additional studies will be required to characterize the behavior of LQTS carriers of all recognized genotypes, for the moment and in light of the one carrier we encountered as noted above, our results would suggest that caution be exercised when giving a potential QT prolonging drug (AAD or otherwise) to a patient if QT prolongation >480 ms is noted in post-ectopic sinus beats on the ECG.






