Cardiac Resynchronization Therapy in Non-Ischemic Cardiomyopathy
Miriam Shanks, MD, PhD, Victoria Delgado, MD, PhD, Jeroen J Bax, MD, PhD
University of Alberta, Mazankowski Alberta Heart Institute, Edmonton (Canada) and Heart Lung Center, Leiden University Medical Center, Leiden (The Netherlands).
Cardiac resynchronization therapy (CRT) is an established therapy for heart failure patients who remain symptomatic despite optimal medical therapy, have reduced left ventricular ejection fraction (<35%) and wide QRS duration (>120 ms), preferably with left bundle branch block morphology. The response to CRT depends on the cardiac substrate: presence of correctable left ventricular mechanical dyssynchrony, presence of myocardial fibrosis (scar) and position of the left ventricular pacing lead. Patients with non-ischemic cardiomyopathy have shown higher response rates to CRT compared with patients with ischemic cardiomyopathy. Differences in myocardial substrate may partly explain this disparity. Multimodality imaging plays an important role to assess the cardiac substrate and the pathophysiological determinants of response to CRT.
Key Words : Cardiac Resynchronization Therapy, Echocardiography, Magnetic Resonance Imaging, Heart Failure.
Correspondence to: Jeroen J Bax, Department of Cardiology,
Heart Lung Center, Leiden University Medical Center;
Albinusdreef 2, 2300 RC Leiden,
The Netherlands.
Non-ischemic cardiomyopathy includes five major phenotypes: hypertrophic cardiomyopathy, dilated cardiomyopathy, restrictive cardiomyopathy, arrhythmogenic right ventricular cardiomyopathy and left ventricular non-compaction.1 The clinical manifestations of these cardiomyopathies vary largely within each form of cardiomyopathy. However, progression to overt heart failure and development of high likelihood of sudden cardiac death are common outcomes to these cardiomyopathies and cardiac resynchronization therapy (CRT) and implantable cardiac defibrillator (ICD) devices may be indicated in selected patients. The current review is focused on the experience with CRT in patients with non-ischemic cardiomyopathy.
The proportion of heart failure patients with non-ischemic cardiomyopathy who were included in large registries and landmark randomized controlled trials on CRT ranges between 33-66%.2-4 CRT has demonstrated similar improvement in all-cause mortality and heart failure hospitalizations of patients with ischemic and non-ischemic cardiomyopathy.4-6 However, in terms of left ventricular (LV) reverse remodeling and improvement in function, patients with non-ischemic cardiomyopathy exhibit larger benefit compared with patients with ischemic cardiomyopathy.3-5,7,8 The underlying differences in demographics (sex and age), comorbidities and cardiac substrate including type of conduction abnormality (left versus right bundle branch block), the presence of mechanical dyssynchrony, the presence and extent of myocardial scar (or more specifically diffuse fibrosis), the varying cardiac venous anatomy, and the LV pacing lead location may all influence the effects of CRT. However, the specific weight of each of these parameters has not been extensively evaluated (and will be difficult to do). In addition, the relationship between CRT and the various phenotypes of non-ischemic cardiomyopathy remains unknown and is limited to small series and case reports.9-16 Probably, the large majority of patients with non-ischemic cardiomyopathy who were enrolled in randomized trials on CRT, had dilated cardiomyopathy.
The present review article summarizes the evidence on the benefits of CRT in heart failure patients with non-ischemic (dilated) cardiomyopathy and discusses the potential role of imaging to improve selection of candidates for CRT.
Cardiac Resynchronization Therapy in Non-Ischemic Cardiomyopathy
Recent data from the National Cardiovascular Data Registry and the implantable cardioverter defibrillator (ICD) registry, including 31,892 heart failure patients treated with CRT, showed that the prevalence of non-ischemic cardiomyopathy was 43%.3 CRT has demonstrated to improve heart failure symptoms and LV systolic function, induce LV reverse remodeling and improve prognosis of these patients.5,17,18 In 191 patients with dilated cardiomyopathy, McLeod et al. showed improvement in LVEF by 18.1±17.1% and mean reduction in LV end-diastolic volume of 60.2±75.1 ml/m2 after a median follow-up of 7 months. Similar results were observed in larger series such as the InSync/InSync ICD Italian registry which included 635 patients with dilated cardiomyopathy.17 After a mean follow-up of 6 months, significant improvements in New York Heart Association (NYHA) functional class (from 3.0±0.6 to 2.0±0.8, p<0.05) and LVEF (from 26±7% to 35±11%; p<0.05) and reductions in LV end-systolic volume (from 147±93 ml to 118±82 ml, p<0.05) were observed. However, 37% of patients did not show any improvement in NYHA functional class or echocardiographic parameters or decrease in hospitalization for heart failure rates at follow-up. Similar percentages of non-response have been described in smaller series.18 The analysis of the cardiac substrate by non-invasive cardiac imaging may provide further insight into CRT response (which may potentially help to select patients).
Assessment of Cardiac Substrate before CRT Implantation in Non-Ischemic Cardiomyopathy
Assessment of LV mechanical dyssynchrony, scar (fibrosis) burden and location in relation to the LV lead position are important in determining the response to CRT and the imaging techniques to evaluate them will be discussed in this section.
Left Ventricular Mechanical Dyssynchrony
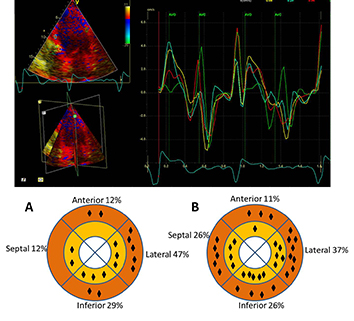
Current recommendations include QRS duration and morphology as criterion for LV dyssynchrony.19,20 It has been demonstrated however, that QRS duration or morphology do not accurately reflect LV mechanical dyssynchrony.21 Cardiac imaging conversely, permits characterization and quantification of LV mechanical dyssynchrony. Echocardiography remains the most widely used technique to evaluate LV mechanical dyssynchrony, and van de Veire et al. showed that in patients with dilated cardiomyopathy, the lateral wall is most often the latest activated segment, whereas the septum is the earliest activated segment
(Figure 1).22
Figure 1. Assessment of left ventricular (LV) dyssynchrony with triplane tissue Doppler imaging (TDI) in 17 patients with dilated cardiomyopathy and QRS duration >120 ms (A) and in 35 patients with ischemic cardiomyopathy and QRS duration >120 ms (B). The upper panel shows the assessment of LV dyssynchrony from the apical 4-chamber view placing 4 regions of interest in the basal and mid ventricular segments. The peak systolic velocity is measured for each mid and basal LV segment within the systolic interval demarcated in the time-velocity graph by the opening (AVO) and closing (AVC) of the aortic valve. The lower panel shows the distribution of the latest activated areas as assessed with triplane TDI in patients with dilated cardiomyopathy (A) and patients with ischemic cardiomyopathy (B). The basal lateral segment is more frequently the most delayed segment in patients with dilated cardiomyopathy whereas in ischemic heart failure patients the distribution is more variable
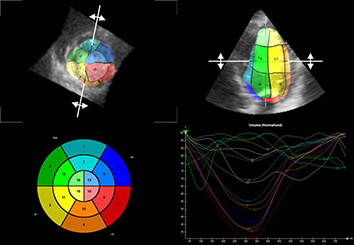
Different echocardiographic techniques have been used to assess LV dyssynchrony, including M-mode echocardiography or more sophisticated techniques such as tissue Doppler imaging (TDI) and 2D speckle tracking. Pitzalis et al. used M-mode echocardiography to show differences between the inward motion of the septum and the posterior wall, which correlated well with the reduction in LV end-systolic volume after CRT in 16 patients with dilated cardiomyopathy.23 Likewise, TDI was used to demonstrate differences in timing of peak systolic velocity of the septum versus the lateral wall, which was associated with response to CRT in large populations of heart failure patients (with both ischemic and non-ischemic cardiomyopathy).24 Patients with more than 60-65 ms difference between the peak velocities of the septum and lateral wall exhibited significant LV reverse remodeling after CRT.25,26 Despite significant evidence demonstrating the association between LV dyssynchrony and response to CRT, current guidelines do not include imaging techniques to improve patient selection for CRT.19,20 The results of the Predictors of Response to Cardiac Resynchronization Therapy (PROSPECT) trial showed limited reproducibility (high inter- and intra-observer variability) of the dyssynchrony parameters, and low predictive value (area under the curve ≤0.62 for all echocardiographic parameters) for clinical and echocardiographic improvement after CRT.27 However, the PROSPECT study had various technical limitations, including the lack of standardized data acquisition and analysis, as well as the use of varying echocardiographic equipment (different vendors) which may have affected particularly the TDI results. In addition, novel techniques such as strain and 3D echocardiography may improve assessment of LV dyssynchrony. 2D speckle tracking has been used to compare regional differences in timing of peak strain (reflecting active deformation, whereas velocities reflect both active and passive motion). Lumens et al. evaluated 81 heart failure patients with this technique and demonstrated that the time difference between peak longitudinal strain of the septum and the lateral wall was significantly related with LV reverse remodeling at follow-up.28 All these techniques rely on differences in timing of opposite walls rather than assessing the mechanical dispersion of the entire left ventricle. To overcome this limitation, 3-dimensional imaging (3D) has been used to derive a systolic dyssynchrony index, measured as the standard deviation of time to minimum regional volume of 16 segments
(Figure 2); the larger the dyssynchrony index was, the more favorable the response to CRT.29
Figure 2. Assessment of left ventricular dyssynchrony with 3-dimensional echocardiography. From the 3-dimensional full volume of the left ventricle, the time to minimum regional subvolume is calculated in 16 segments and the time-volume curves for each segment are plotted. The standard deviation of time to minimum regional subvolume of 16 segments is 13.8%
Other imaging techniques have also been proposed for assessment of LV dyssynchrony. Using MRI-myocardial tagging, Bilchick et al. proposed the circumferential uniformity ratio estimate (CURE) as a measure of LV dyssynchrony which is derived from the measurement of time to peak circumferential strain in 24 points of the LV myocardium in 3 evenly spaced myocardial slices.30 A CURE value close to 1 indicates perfect synchronicity whereas a value close to 0 indicates complete dyssynchrony. In 20 patients undergoing CRT implantation (60% with dilated cardiomyopathy) a cut-off value of CURE <0.75 was associated with high probability of response to CRT.30 Furthermore, LV dyssynchrony can be assessed with gated blood-pool ventriculography and single photon emission computed tomography (SPECT) myocardial perfusion imaging (MPI) phase analysis.31 A study of 64 patients (17 with non-ischemic cardiomyopathy) who met standard criteria for CRT and who underwent SPECT MPI demonstrated that the non-ischemic cardiomyopathy patients with QRS duration ≥150 ms had significantly more LV dyssynchronous activation than those with QRS duration between 120 and 150 ms.32 A study of 32 patients with non-ischemic cardiomyopathy used equilibrium radionuclide angiography to quantify LV intraventricular dyssynchrony by measuring standard deviation of LV mean phase angle.33 Receiver operating characteristics curve analysis demonstrated 95% sensitivity and 80% specificity at a cut-off value of 308 for standard deviation of LV mean phase angle in prediction of CRT response.33 In addition, patients with dilated cardiomyopathy and left bundle branch block (LBBB) may show reduced work in the early activated septum which is associated with decreased glucose utilization as measured by septal F-18-fluorodeoxyglucose (FDG) uptake on positron emission tomography (PET) relative to perfusion, a so-called reverse-mismatch.34 This indirect marker of dyssynchrony was recently studied by Bernie et al. who showed that septal reverse mismatch <17.2% had good sensitivity (92%) and specificity (78%) to predict response to CRT (defined as reduction in LV end-systolic volume >10% or increase in absolute LVEF ≥5%) in patients with non-ischemic cardiomyopathy.35
Finally, pathophysiological characteristics may also have contributed to non-response of CRT. These factors include the extent and location of macroscopic fibrosis (scar); in patients with dilated cardiomyopathy, macroscopic focal fibrosis (scar) or diffuse microscopic fibrosis may limit CRT response, specifically if the LV pacing lead is positioned in an area of significant fibrosis. In addition, venous anatomy may also affect response to CRT: if the segment with the latest mechanically activation is not in the vicinity of cardiac veins, then this myocardium may not be reached for synchronization. Particularly, cardiac CT may non-invasively provide a roadmap for the location and extent of cardiac veins.
Location and Burden of Myocardial Fibrosis
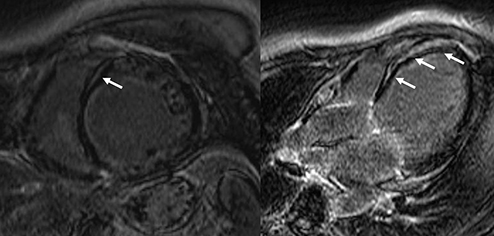
The presence of replacement myocardial fibrosis has been associated with lower rates of response to CRT.36,37 Currently, late gadolinium contrast-enhanced MRI permits localization and quantification of myocardial replacement fibrosis with high spatial resolution. In contrast to patients with ischemic cardiomyopathy, where replacement fibrosis (scar) follows subendocardial or transmural distribution along coronary artery territories, in patients with non-ischemic cardiomyopathy the distribution of replacement fibrosis is variable, does not follow the coronary artery territory and depends on the underlying etiology. In idiopathic dilated cardiomyopathy, a characteristic midwall septal fibrosis can be observed in 30% of patients
(Figure 3),38 whereas patients with sarcoidosis commonly show patchy fibrosis located in the basal septum (involving the conduction system) and lateral wall, whereas in patients with cardiac amyloidosis, circumferential subendocardial fibrosis is characteristic. The association between myocardial replacement fibrosis and response to medical or device therapy has been investigated mainly in patients with idiopathic dilated cardiomyopathy.39-42 In 97 patients with idiopathic dilated cardiomyopathy who received a CRT device, Leyva and coworkers reported a prevalence of midwall septal fibrosis on late gadolinium contrast enhanced (LGE) MRI of 21%.41 Compared with patients without fibrosis, patients with midwall myocardial fibrosis showed significantly larger LV volumes and worse LVEF and functional status (with worse quality of life scores or 6-minute walk distance). In terms of clinical response (defined by freedom from heart failure hospitalization 1 year after implantation, improvement in ≥1 point NYHA functional class and ≥25% increase in 6-minute walk distance), the response rate was lower among patients with midwall septal fibrosis (65% vs. 80%) compared with their counterparts. In addition, patients with midwall septal fibrosis did not show significant reduction in LV volumes or improvement in LVEF at follow-up whereas patients without replacement fibrosis showed significant LV reverse remodeling with reductions in LV end-systolic volume of ≥15%. Interestingly, these differences were accompanied by significant differences in survival: after a median follow-up of 2.8 years, the all-cause mortality rate of patients with midwall septal fibrosis was 50% compared with 6.5% of patients without fibrosis. On multivariate analysis, the presence of midwall septal fibrosis was significantly associated with increased risk of all-cause mortality (hazard ratio 18.1, p<0.001).
Figure 3. Assessment of myocardial fibrosis with LGE-MRI in dilated ischemic cardiomyopathy. A 53 year-old male with dilated cardiomyopathy and midwall fibrosis extending along the septum (arrows)
Nevertheless, in patients with dilated cardiomyopathy the amount of diffuse interstitial fibrosis may be larger than the presence of the focal fibrosis. Using T1 mapping MRI techniques, the extent of diffuse myocardial fibrosis can be quantified: in native data (pre-contrast), the T1 time values (relaxation of the myocardium) will increase along with the amount of diffuse fibrosis whereas in post-contrast data, the accumulation of gadolinium in the interstitial space will lead to a proportional decrease in T1 time values. Taking into consideration the hematocrit, the extracellular volume can be calculated from native and post-contrast T1 time values representing the amount of myocardial diffuse fibrosis. In 21 patients with dilated cardiomyopathy and 27 ischemic heart failure patients treated with CRT, Chen et al. showed that patients who showed LV reverse remodeling at follow-up tended to have lesser extent of diffuse fibrosis compared with patients who did not show LV reverse remodeling (0.30±0.06 vs. 0.34±0.06, p=0.043).39 However, on multivariate analysis, the association between diffuse myocardial fibrosis and LV reverse remodeling was not significant, probably due to the stronger association between the presence of macroscopic focal replacement fibrosis and absence of LV reverse remodeling at follow-up. Additional studies including homogenous populations of patients with dilated cardiomyopathy treated with CRT and controlling for other confounding factors may help to better understand the correlation between diffuse myocardial fibrosis and response to CRT.
The conventional CRT practice places the LV lead in the (postero) lateral wall, which is presumably the site of latest mechanical activation due to LBBB and QRS prolongation. Lin et al. showed that such presumption may be more likely true in the non-ischemic cardiomyopathy patients.32 Several studies demonstrated that a concordant LV lead position with the latest activated LV segments was associated with the greatest improvements in clinical status and LV performance in heart failure patients treated with CRT.43-46 On the other hand, myocardial fibrosis (scar in ischemic heart failure patients) in the vicinity of the LV lead tip leads to a suboptimal response to CRT.47-49 The myocardial fibrosis patterns observed in patients with dilated cardiomyopathy (more frequently midwall fibrosis of the interventricular septum) reduces the probability of placing the LV lead in an area of transmural fibrosis. Research has focused on the use of imaging techniques to guide lead placement to maximize the effects of CRT. Recently, two randomized trials (Targeted left ventricular lead placement to guide cardiac resynchronization therapy [TARGET] and Speckle tracking assisted resynchronization therapy for electrode region [STARTER]) showed that LV lead placement guided by the site of latest activation on speckle-tracking imaging resulted in a larger proportion of a favorable LV lead position, greater LV reverse remodeling and improved survival, compared to standard coronary venography guided placement of LV lead into the lateral, posterior, or posterolateral region.44,45 Long-term (39 months) follow-up in the TARGET trial demonstrated 70% survival rate in the patients with concordant/adjacent LV lead compared to 38% in the group with a remote LV lead position (p=0.003).50 However, these studies included a majority of patients with ischemic heart disease. Experiences evaluating the role of non-invasive imaging to guide the positioning of the LV lead in non-ischemic cardiomyopathy patients are scarce.
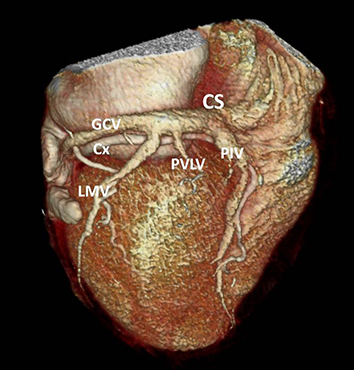
The particular coronary vein used for the LV lead is dependent on individual cardiac venous anatomy. Retrograde venography via the coronary sinus is currently the standard technique for defining cardiac venous anatomy just prior to LV lead implantation. Cardiac computed tomography is increasingly utilized to visualize the coronary veins for pre-procedural planning of LV lead placement
(Figure 4). Ricapito et al. demonstrated that cardiac CT was more sensitive for detecting posterior and left marginal veins compared to retrograde venography.51 In addition, the left marginal vein was less likely observed in the patients with ischemic cardiomyopathy as compared with non-ischemic cardiomyopathy (42.9% vs. 66.7%).51 In the study by van de Veire et al., the venous anatomy was strongly related to the presence of prior myocardial infarction, with left marginal vein present in only 22% of patients with anterior infarction and none of the patients with lateral infarction.52 Coronary venous anatomy can also be reliably demonstrated using a comprehensive MRI protocol which includes myocardial perfusion, LV function and myocardial fibrosis.53
Figure 4. Assessment of myocardial fibrosis with LGE-MRI in dilated ischemic cardiomyopathy. A 53 year-old male with dilated cardiomyopathy and midwall fibrosis extending along the septum (arrows)
Even though the ability to secure LV leads in a major cardiac vein through coronary sinus cannulation is increasingly feasible, up to 10% of the patients undergoing CRT implantation have a failure of coronary sinus cannulation.54 The possibility of direct surgical placement of the LV lead as rescue therapy for a failed transvenous approach has not only overcome the limitations imposed by coronary venous anatomy, but also potentially enabled easier targeting of the latest activated regions of LV.55
Current guidelines do not include imaging criteria to select heart failure patients for CRT.19,20 However, they underscore the evidence provided by several observational and prospective trials on the relevance of LV dyssynchrony assessment, evaluation of myocardial scar and identification of the target region for LV lead placement. Design of new trials randomizing heart failure patients to CRT versus ICD alone or optimal medical therapy based on several imaging criteria (including assessment of LV dyssynchrony, myocardial scar, and the latest mechanically activated segment) would need a large number of patients, particularly if only non-ischemic cardiomyopathy patients are included, and may not be feasible in the near future. However, it remains important to accurately evaluate the patients who are candidates to CRT, and assess the different aspects that may influence the response to CRT. Availability of imaging techniques and local expertise will determine which imaging modalities can be used for the evaluation of CRT candidates.






